
Abstract
Background:
The effect of surgeon experience on patient outcomes after surgical Achilles tendon rupture (ATR) repair has so far been unknown.
Purpose:
To examine whether patient-reported and functional outcomes as well as adverse events after surgical ATR repair differ between orthopaedic specialist surgeons and resident surgeons.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
We retrospectively analyzed data from 295 patients treated with surgical ATR repair with standardized techniques. The level of surgeon experience (specialist vs resident) and number of adverse events (rerupture, infection, and deep venous thrombosis) were recorded. Patient-reported and functional outcomes were assessed 12 months postoperatively using the validated Achilles tendon total rupture score (ATRS) and the heel-rise test, respectively. Analysis of covariance was used to compare differences in outcomes between specialist surgeons and resident surgeons. Pearson chi-square or Fisher exact test was used for analysis of adverse events.
Results:
The mean ATRS at 12 months for patients operated on by resident surgeons was significantly higher compared with specialist surgeons (85.9 [95% CI, 80.3-91.5] vs 77.8 [95% CI, 73.8-81.9]; P = .028). In addition, the lateral difference (operated vs unoperated side) in mean total concentric work and number of heel-rise repetitions at 12 months was smaller in patients operated on by resident surgeons (P = .011 and 0.015, respectively). The number of adverse events did not differ significantly between the 2 groups.
Conclusion:
Resident surgeons achieved patient-reported and functional outcomes at least as good as those of specialist surgeons in surgical ATR repair, with a similar risk of adverse events.
Keywords
Patient outcomes after surgical repair of acute Achilles tendon rupture (ATR) vary, and long-term functional deficits are common. 13,16 Increased understanding of factors influencing outcomes is crucial to develop clinical practices.
There is evidence that delay from injury to surgery and short duration of surgery are associated with inferior patient outcomes after ATR in addition to older age, obesity, and presence of deep venous thrombosis (DVT). 2,12,17,20 –22,26 Ideally, surgical training should not affect patient outcomes significantly. In orthopaedic surgery, however, there is some evidence that the level of surgeon experience may influence long-term outcomes. 4,8,9,11 It is plausible that the impact of level of surgeon experience depends on the type of surgical procedure. When it comes to surgical ATR repair, the effect of level of surgeon experience on patient outcomes and patient safety has been unknown.
In Sweden, an orthopaedic surgeon must accomplish a 5-year residency before receiving a specialist license issued by The Swedish National Board of Health and Welfare. Surgical training starts by assisting specialist surgeons, whereafter residents perform surgical procedures more independently. Surgical ATR repair is technically relatively simple and is therefore often considered a suitable surgical procedure for orthopaedic residents to perform, ideally with supervision and assistance from a specialist surgeon as needed. Differences in level of surgeon experience could theoretically be among the factors contributing to variations in patient outcomes after surgical ATR repair.
The aim of this study was to examine whether patient-reported and functional outcomes as well as number of adverse events differ between patients with ATR operated on by orthopaedic resident surgeons and those operated on by specialist surgeons.
Methods
Study Population
This study was a retrospective analysis of patient data from randomized controlled trials (RCTs) investigating different treatment protocols after surgical repair of acute ATR. 6,24 The surgical procedures were performed in Stockholm, Sweden, mainly at Karolinska University Hospital but also at Danderyd Hospital, between 2011 and 2014. Ethical approvals were obtained from the regional ethical review committee, and the studies were registered at http://ClinicalTrials.gov. All participants received oral and written information about the study procedure and provided written informed consent before surgery.
The following inclusion and exclusion criteria were applied to the RCTs. 6,24 Inclusion criteria were acute ATR, age of 18 to 75 years, and surgery performed within 4 days to 1 week following injury. 6,24 Exclusion criteria were anticoagulant therapy, known kidney failure, heart failure with pitting edema, thrombophlebitis, any thromboembolic event during the previous 3 months, other surgery during the previous month, known malignancy, hemophilia, pregnancy, unwillingness to participate, inability to follow instructions or give informed consent, and follow-up at another hospital. 6,24 An additional inclusion criterion applied in this retrospective analysis was knowledge of the level of surgeon experience. Characteristics of patients operated on by residents and specialists in this retrospective analysis are shown in Table 1.
Characteristics of Patients Operated on by Resident Versus Specialist Surgeons a
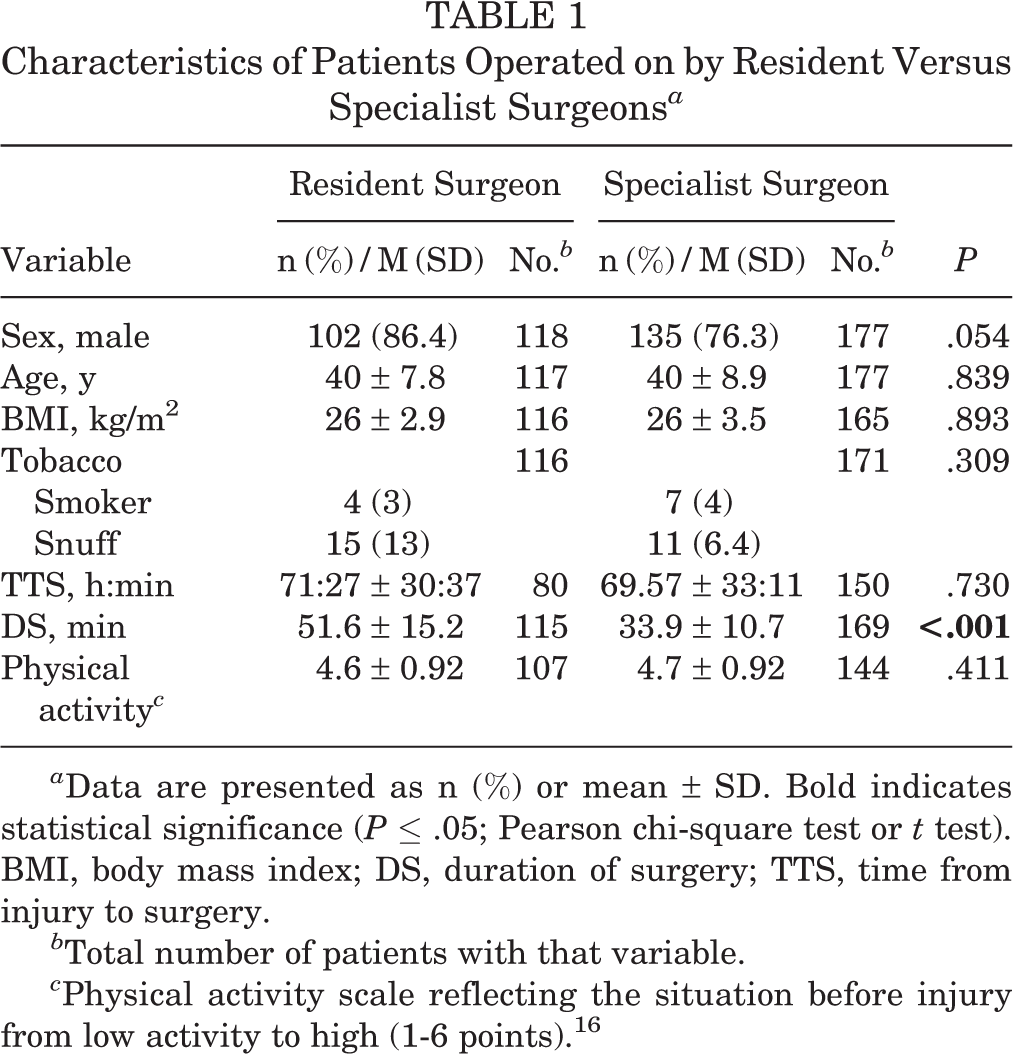
a Data are presented as n (%) or mean ± SD. Bold indicates statistical significance (P ≤ .05; Pearson chi-square test or t test). BMI, body mass index; DS, duration of surgery; TTS, time from injury to surgery.
b Total number of patients with that variable.
c Physical activity scale reflecting the situation before injury from low activity to high (1-6 points). 16
A flowchart of patients in this retrospective analysis is shown in Figure 1. 6,24

Flowchart of patients included in this retrospective analysis. In addition, a couple of patients had data on some subscores of patient-reported or functional outcome. Lost to follow-up: resident group 16% (19/118), specialist group 23% (40/177). ATR, Achilles tendon rupture; ATRS, Achilles tendon total rupture score; DVT, deep venous thrombosis.
Dropout Analysis
All participants were invited to a 12-month follow-up. Comparison of Achilles tendon total rupture score (ATRS) data between patients with and without the 12-month follow-up showed no significant differences in patient characteristics or postoperative treatments within the resident or specialist patient cohorts.
Surgical Procedure
The surgical ATR repair was performed by the surgeon scheduled on the day of surgery, and neither surgeon nor patient could influence these conditions. The study protocols in the RCTs included standardized anesthetic and surgical techniques. 6,24 Before surgery, local anesthetics with adrenaline was injected into the skin and peritendinous space. A longitudinal 5- to 10-cm incision was made in the dorsomedial part of the lower calf, followed by a midline incision in fascia cruris and paratenon. The tendon ends were then sewn together using a modified Kessler suture with two 1-0 polydioxanone (PDS II) sutures (Ethicon). The paratenon and fascia cruris were closed using Vicryl 3-0 (Ethicon) and the skin was closed using Ethilon 3-0 (Ethicon) single-interrupted sutures. No anti-inflammatory or thromboprophylactic drugs were given postoperatively. 6,24 Duration of surgery started when the scalpel was introduced to the skin and ended when the incision was closed.
To ensure that the protocol of the standardized surgery was followed, a review of the surgical reports was performed. It was recorded in the medical records whether the surgeon reported using 2 PDS II sutures, closing the fascia cruris, and closing the paratenon.
Postoperative Treatment
In the RCTs, patients were allocated into 3 different postoperative treatment protocols for the first 6 weeks after surgery. 6,24 The first protocol included a plaster cast with 30° equinus in the ankle for the first 2 weeks. After 2 weeks, the plaster cast was replaced by an orthosis with heel wedges (Aircast Air Select Elite; DJO Global) and full weight-bearing was allowed. The second protocol included an orthosis with heel wedges (Aircast Air Select Elite; DJO Global) for 6 weeks with weight-bearing as tolerated and intermittent pneumatic compression (IPC) on both calves daily during the first 2 weeks. The third protocol included functional weight-bearing mobilization with an ankle-mobile orthosis (VACOPed; OPED Medical) for 6 weeks.
In total, 124 patients received a plaster cast, 95 an ankle-mobile orthosis, and 74 the IPC treatment. Data on postoperative treatment group was missing on two patients in specialist surgeon group. The postoperative treatment groups were significantly related to surgeon experience; IPC was significantly more common in patients operated on by specialists (P = .001) and ankle-mobile orthosis was more common in patients operated on by residents (P < .001). Proportions of plaster cast did not differ significantly. Calf-IPC and early functional mobilization in ankle-mobile orthosis have been associated with similar outcomes as plaster cast in previous studies. 1,3
Level of Surgeon Experience
The level of surgeon experience and the presence of an assistant were registered in a review of medical records. The surgeons were divided into 2 groups according to their level of experience: specialist or resident. If a resident surgeon was scheduled on the day of surgery, then he/she became the responsible surgeon, with a possibility to have a specialist surgeon as an assistant. Specialist surgeons were assisted by residents or, in some cases, by medical students.
Patient-Reported Outcomes
Patient-reported outcomes at 12 months postoperatively were evaluated with the ATRS (Swedish, version 6) which is a validated, self-administered questionnaire. 6,15,24 The ATRS evaluates limitations experienced due to ATR on a 10-step scale ranging from 0 (very limited) to 10 (no limitation). ATRS includes 10 questions, and 100 is the maximal score. 15 ATRS subscales include strength in the calf, tiredness in the calf, stiffness in the calf, pain in the calf, limitations in activities of daily living, limitations on uneven surface, limitations in stairs/hills, limitations when running, limitations when jumping, and limitations in physical work. It has been suggested that a 10-point difference in ATRS is clinically significant. 15
Functional Outcomes
Functional outcomes at 12 months were evaluated with a heel-rise test using MuscleLab dynamometer (Ergotest Technology). 6,24 The heel-rise test has previously been used to evaluate the outcome after ATR and is considered reliable. 19 In the heel-rise test, the height and number of heel-rises are recorded using a linear encoder connected to footwear via a spring-loaded string. Concentric work (in joules) was derived from height (in centimeters), weight (in kilograms), and time (in seconds) measurements. Lateral difference in functional outcome was calculated as performance on the unoperated side minus performance on the operated side.
Adverse Events
In this study, an adverse event refers to either a DVT at 2 or 6 weeks, a surgical site infection (SSI) during the first 6 weeks, or a rerupture during the first year. All patients were screened for a DVT using compression sonography with color Doppler (Philips CX 50 ultrasound machine; Philips Medical Systems) on the injured side at 2 and 6 weeks postoperatively. 6,24 The diagnostic criteria for DVT have been described previously. 6,10 The symptomatic or asymptomatic nature of DVT was not recorded in the trials. Patients who developed DVT received low-molecular-weight heparin according to hospital protocol. The surgical wound was inspected at 2 and 6 weeks, and a clinical suspicion of infection was confirmed by a swab culture of the wound. Culture-confirmed SSIs were treated with adequate antibiotics. 18
Statistical Methods
Statistical Package for Social Sciences (SPSS, version 27.0; IBM Corp.) was used for all descriptive and statistical analyses. Analyses were conducted in collaboration with a statistician (G.E.). The sample size was calculated on a 10-point expected difference in ATRS between the groups. A total of 48 patients in each group were required to detect a difference of 10 points in ATRS (2-sided type 1 error rate = 5%; power = 90%).
Categorical variables were summarized with frequencies and percentages. Continuous variables were checked for skewness and summarized with means and standard deviations. Patient characteristics were compared using Pearson chi-square test or Student t test.
Analysis of covariance adjusted for duration of surgery, postoperative treatment, patient sex, and patient age was used to analyze associations between level of surgeon experience and treatment outcomes. Both adjusted and unadjusted P values were presented. Differences in adverse events between patients operated on by resident and specialist surgeons were analyzed with the Pearson exact or Fisher exact test. The level of significance in all analyses was P ≤ .050 (2-tailed).
Results
Outcomes
The patient-reported and functional outcomes are presented in Table 2. Patients operated on by residents exhibited a statistically significantly higher mean ATRS at 12 months than patients operated on by specialists (P = .028). Patients operated on by a resident had a significantly smaller lateral difference in mean total concentric work (P = .011) and in the number of heel-rise repetitions (P = .015) than patients operated on by specialists.
Patient-Reported and Functional Outcomes at 12-Month Follow-up a

a Data are reported as mean (95% CI). Bolded P values indicate statistically significant difference between groups (P ≤ .05; analysis of covariance adjusted for patient sex and age, duration of surgery, and postoperative treatment). ATRS, Achilles tendon total rupture score.
b Lateral difference (unoperated minus operated side) on heel-rise test.
Adverse Events
The risk of any adverse event did not differ between patients operated on by resident and specialist surgeons (Table 3). The risk of a DVT was 46% in the specialist cohort and 43% in the resident group (P = .623). Risk of SSI was 4% in both the resident specialist groups (P > .99). The number of reruptures was one in the resident cohort and two in the specialist cohort (Table 3).
Adverse Events a

a DVT, deep venous thrombosis; n, number of patients with the condition; N, total number of patients; SSI, surgical site infection.
bP values from Pearson’s chi-squared test or Fisher’s exact test.
Duration of Surgery
Duration of surgery was significantly longer for resident surgeons compared with specialist surgeons (P < .001) (Table 1).
Presence of an Assistant Surgeon
In total, 65 surgeons participated in this study and some performed surgery on multiple occasions; 30 of them were specialist surgeons and 35 were resident surgeons. An assistant specialist surgeon was present in 44% (52/117; 95% CI, 35.4%-53.4%) of the surgical procedures performed by resident surgeons. An assistant surgeon was present in 21% (36/174; 95% CI, 14.7%-26.7%) of the procedures performed by specialist surgeons. Resident surgeons were assisted significantly more often (P < .001). No significant differences in outcomes between resident and specialist surgeons were found in surgical procedures performed with or without an assistant surgeon; however, the power was low (Table 4). Similarly, no significant differences in outcomes between assisted and nonassisted procedures were found within resident or specialist surgeon groups (see Appendix Table A1).
Comparison of Outcomes Between Resident and Specialist Surgeons in Procedures Performed With or Without an Assistant Surgeon a

a Data are reported as mean (95% CI). ANCOVA, analysis of covariance; ATRS, Achilles tendon total rupture score.
b ANCOVA adjusted for patients’ sex and age, duration of surgery, and postoperative treatment.
c Lateral difference (unoperated side minus operated side) on heel-rise test.
Adherence to Surgical Protocol
A review of surgical protocols concluded that resident and specialist surgeons demonstrated similar adherence to the predefined surgical protocol regarding closing of the fascia cruris (68% vs 51%; P = .084), closing of the paratenon (88% vs 88%; P = .897), and using 2 PDS II sutures (87% vs 89%; P = .531).
Discussion
The study findings showed that both patient-reported and functional outcomes were significantly better for patients operated on by a resident surgeon compared with a specialist surgeon, while the risk of adverse events was similar in both groups. Duration of surgery was significantly longer for resident surgeons.
The most important finding of this study that patients operated on by resident versus specialist surgeons exhibited significantly better ATRS at 12 months. The mean ATRS was 8 points better for patients operated on by residents compared with those operated on by specialists, but only a minimum 10-point difference had been suggested previously to reflect a clinically significant difference. 15
There is earlier evidence that orthopaedic resident surgeons may perform as well or slightly poorer than specialist surgeons when it comes to long-term patient outcomes. 4,8,9,11 Outcome for intramedullary nailing after tibial shaft fractures was not influenced significantly by level of surgeon experience, 11 which supports our conclusion that resident surgeons are able to achieve outcomes at least as good as those of specialist surgeons. There is some evidence that a higher level of surgeon experience may slightly improve patient outcomes after hip arthroplasty. 8,9 In adolescent idiopathic scoliosis surgery, residents seem not to be able to achieve outcomes similar to those of specialists, but this latter result may have been influenced by study limitations. 4 Total hip arthroplasty and scoliosis surgery are more complicated procedures than intramedullary nailing and ATR repair. It is plausible that several years of experience is especially important when performing complicated surgery.
A second main finding of this study was that patients operated on by residents exhibited significantly smaller lateral differences in functional outcomes compared with patients operated on by specialists. The differences could potentially influence a patient’s everyday life and performance in sports. These observations support the main finding of a difference in patient-reported outcomes between resident and specialist surgeons. This study could not give an exact answer as to why these differences exist, but possible explanatory factors are discussed below.
A factor that may affect outcomes positively is the presence of a surgical assistant. In this study, residents were assisted more frequently than specialist surgeons, which may have affected the outcome. There was no assistant in the majority of surgical procedures performed by residents, and there was a trend toward a significant difference in total concentric work in favor of residents when no assistant was present, suggesting that a surgical ATR repair can be performed by a resident autonomously with a good outcome. In additional analyses, assistance did not significantly influence patient outcomes either in the resident- or specialist-surgeon group. However, it is still plausible that surgical assistance is advantageous and may explain some of the observed differences in outcomes between resident and specialist surgeons since residents had an opportunity to call in a specialist at any time during surgery as needed.
The mean duration of surgery was significantly longer for resident surgeons. This observation is in line with evidence from other surgical fields showing that experience correlates with faster surgical procedures. 4,5,7,23 Interestingly, longer duration of surgery has been shown to correlate with increased metabolic response in the healing Achilles tendon and improved patient outcomes in a study by Svedman et al. 22 However, the difference in the duration of surgery was considered in the statistical analyses in this study. It is therefore unlikely that the difference in duration of surgery explains all the variation in outcomes.
Ability to work faster and to minimize surgical tissue trauma may be achieved by experience. It can be hypothesized that less experienced surgeons may, by an especially meticulous approach or by some other surgical details, promote the healing process independent of duration of surgery and assistance. 22 According to additional analyses, resident and specialist surgeons demonstrate similar adherence to the predefined surgical protocol in this study, suggesting no major differences in surgical technique. However, a slight tendency for residents to more often suture the fascia cruris may reflect a larger difference in surgical techniques than captured in the review of surgical reports. Fascia cruris is attached to Achilles tendon posteriorly, and there is evidence that tears of fascia cruris are a cause of Achillodynia. 25 Therefore, it is plausible that closing the fascia cruris may be important for patient outcomes. 14
The third main finding of this study was the similar degree of adverse events between both surgeon groups. The observation of a similar rate of SSIs, reruptures, and DVTs among patients operated on by specialists versus residents suggests that ATR surgery performed by resident surgeons does not pose a threat to patient safety. In other surgical areas, comparative infection rates (resident vs specialist) have been reported previously, 4,11 which strengthen the observations from this study.
A limitation in this study is that the ATR repair volume of each surgeon was not specified. It is possible that the frequency of performing this procedure, regardless of specialist or resident status, may be an important factor influencing the outcome. It is also plausible that resident surgeons receive assistance primarily at the beginning of their training, but this was not analyzed further. The difference between a junior resident and senior resident may also be larger than the difference between a senior resident and a specialist surgeon. However, classification into resident or specialist surgeons is intuitive and relevant in a clinical context, which is the reason why this division was used. This study had several strengths, such as both subjective and objective evaluation of outcomes validating each other. The cohort was also large, several surgeons were included, procedures were performed using standardized surgical protocols, and DVT screening was included.
Conclusion
Resident orthopaedic surgeons, with currently available assistance and supervision, demonstrated clinical outcomes at least as good as those of specialists in the surgical repair of acute ATR. Risk of adverse events did not differ, but duration of surgery was longer for resident surgeons. These results are encouraging for orthopaedic surgeons in their early career.
Footnotes
Final revision submitted November 19, 2021; accepted December 19, 2021.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Regional Ethics Commission of Stockholm (protocol 2013/1791-31/3, 2009/2079-31/2).