
Abstract
Background:
Tendon healing differs between the sexes. Comparisons in outcome between the sexes after an Achilles tendon rupture are often not possible because of the small cohort (<20%) of women.
Purpose:
To evaluate whether there are any differences in outcome between the sexes by combining the data from 2 large randomized controlled trials that used identical outcome measures.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
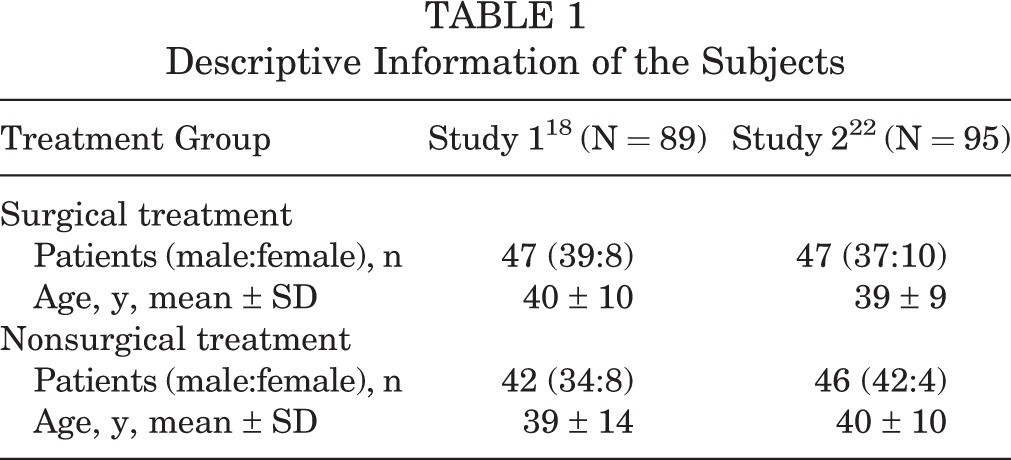
Included in the evaluation were patients from 2 consecutive randomized controlled trials comparing surgical and nonsurgical treatment performed at our research laboratory. Patients who had a rerupture were excluded from analysis. A total of 182 patients (152 males, 30 females), with mean ± SD age of 40 ± 11 years, were included; 94 (76 males, 18 females) were treated with surgery and 88 (76 males, 12 females) nonsurgically. Patient-reported outcome was evaluated using the Achilles tendon Total Rupture Score (ATRS), and the functional outcome was measured with a heel-rise test (measurement of muscular endurance and heel-rise height) at 6 and 12 months after injury.
Results:
Male patients had a greater improvement in heel-rise height at 12 months (P = .004). When each treatment group was analyzed separately, it was found that female patients had significantly (P < .03) more symptoms after surgical treatment (mean ± SD ATRS, 59 ± 24) compared with males at 6 (73 ± 19) and 12 months (74 ± 27 vs 86.5 ± 17). This sex difference was not found in the nonsurgical treatment group. For the entire group, there were no significant differences between treatments on ATRS at 6 and 12 months. The surgical group had significantly better results compared with the nonsurgical group in heel-rise endurance at 6 and 12 months and in heel-rise height recovery at 6 months (P < .03 for both).
Conclusion:
Sex differences were demonstrated, and female patients had a greater degree of deficit in heel-rise height as compared with males, irrespective of treatment. Females had more symptoms after surgery both at 6 and 12 months, but this difference was not found when treated nonsurgically.
Clinical Relevance:
Further research is needed to determine whether women will benefit more from nonsurgical compared with surgical treatment after an Achilles tendon rupture.
Surgical or nonsurgical treatment of Achilles tendon rupture is currently a hot topic. The current evidence indicates that surgery might decrease the risk for rerupture but increase the risk for other complications, such as infection, sural nerve injury, and scar problems. 1,12 However, regardless of initial treatment (surgery vs no surgery), it has been demonstrated that the majority of patients have decreased function on the injured side. 13,18,22,31 The injury also affects their ability to return to previous levels of physical activity. 11,17 There are also large variations in outcomes between patients, that is, some patients are fully recovered while others have moderate to major functional deficits with residual symptoms 1 year after injury. 18,22
To further understand how to improve both the short- and long-term outcomes after an Achilles tendon rupture, a few studies have looked at predictors of outcome. 2,21 A recently published study found that treatment (nonsurgical or surgical) was a moderate predictor of symptoms and a weak predictor of function. 21 Other factors appear to be of greater importance, for example, increasing age being a strong predictor of reduced heel-rise height, and higher body mass index being a strong predictor of greater degree of symptoms. 21 This study, however, excluded female sex from the analysis, as the subgroup of women was small.
Other studies also support the argument that there are differences between the sexes in terms of outcome after an Achilles tendon rupture. 2,23 In 1 study, patients who were able to perform a single-leg heel-rise 3 months after injury were significantly younger, more often of the male sex, had less symptoms, and had a higher degree of physical activity. 17,20 In a follow-up study of 101 patients, Leppilahti et al 13 found that calf muscle weakness was greater in female patients compared with males. On the other hand, Bostick et al 2 found that male sex was a negative predictor of calf muscle endurance at 1 year.
To compare sex differences in outcomes in patients with an Achilles tendon rupture is difficult because there are fewer women who sustain an Achilles tendon rupture. In most studies, women account for less than 20% of patients. 5,8,9,12 Therefore, to reach an adequate cohort size to perform sex comparisons, one needs to either perform larger studies or combine data from various studies. It is often difficult to combine the data from different studies due to differences in outcome measures. However, 1 research group has performed 2 consecutive randomized controlled trials comparing surgical and nonsurgical treatment within a 6-year time span using identical outcome measurements, the same 2 independent evaluators, and the same equipment. 18,22 This circumstance therefore provides for a unique opportunity of combining the data to compare outcomes between sexes.
The purpose of this study was to evaluate whether there are any differences in outcome between men and women after an acute Achilles tendon rupture.
Methods
Included in the evaluation were patients from 2 consecutive randomized controlled trials comparing surgical and nonsurgical treatment performed in our research laboratory. 18,22 Patients who had reruptures were excluded from this study. Of the 12 patients with rerupture, only 2 were female, and were all in the study by Nilsson-Helander et al. 18 A total of 182 patients (152 males, 30 females) with mean ± SD age of 40 ± 11 years were included. There were 94 patients (76 males, 18 females) treated with surgery and 88 (76 males, 12 females) treated nonsurgically.
Treatment Procedure
Both of the randomized controlled trials are published, and the specifics of the different treatment protocols can be found in the original studies. 18,22 The inclusion criteria were identical for the 2 studies. All patients (age range, 18-65 years) with a unilateral closed midsubstance rupture were included. Patients were excluded if the rupture was older than 3 days (study 1) or 4 days (study 2) and if they had a prior Achilles tendon rupture. All subjects gave written informed consent, and the studies were approved by the regional ethical review board in Gothenburg, Sweden. Below is a brief description of the treatment protocols and designs of the 2 studies.
Study 1 18
Forty-seven patients were treated surgically with a modified Kessler suture (resorbable), and 42 were treated without surgery. Both groups were treated with a below-the-knee cast with the foot in an equinus position for 2 weeks, followed by an adjustable brace (Don Joy ROM Walker) for the following 6 weeks. The brace was set at free plantar flexion motion with dorsiflexion limited to –30° for the first 2 weeks, –10° the next 2 weeks, and +10° the last 2 weeks. Weightbearing as tolerated was allowed after 6 to 8 weeks. The brace was adjusted by a physical therapist. All patients followed a standardized rehabilitation protocol under the supervision of 2 experienced physical therapists.
Study 2 22
The intervention group was treated with a specifically designed surgical repair method followed by accelerated rehabilitation. These patients used a walker brace for 6 weeks postoperatively, they were allowed immediate full weightbearing, and started range of motion as well as strength training 2 weeks postoperatively. The patients in the control group were treated nonsurgically, used the same walker brace for 8 weeks, and were also allowed full immediate weightbearing. However, rehabilitation started after removal of the brace in this group. There were 47 patients from the surgical group and 46 patients from the nonsurgical group included in this study.
Evaluation
All patients were evaluated with identical outcome measures at 6 and 12 months after injury. Two experienced physical therapists who were not involved in the treatment performed all the evaluations at the Lundberg research laboratory.
Patient-Reported Outcomes
The Achilles tendon Total Rupture Score 19 (ATRS) was used to assess the patients’ symptoms. This measure has been found reliable and valid, and scores range from 0 to 100, with a lower score indicating greater limitations and more symptoms. 4,10
Functional Evaluation
The single-leg heel-rise test was used for evaluating calf and Achilles tendon function. This test was performed as previously described in the literature. 25 The MuscleLab (Ergotest Technology) measurement system with a linear encoder was used for data collection. A string was attached to the heel of the patient’s shoe. The string measured the height of every heel rise and also counted the number of heel rises. Since the resistance was known, it was also possible to evaluate the total amount of work (in joules) the patient performed on each side. The evaluator provided shoes for the evaluation, and the patients wore the same shoes on each testing occasion. The patients were standing on a 10° incline and instructed to perform as many and as high of heel rises as possible at a rate of 1 heel rise every 2 seconds, as indicated by a metronome. The maximal height of the heel rise and the number of repetitions and the total amount work performed was used for the evaluation.
Statistical Analysis
Descriptive data are reported as mean ± SD, median (interquartile range [IQR]), and frequency. The limb symmetry index (LSI) was calculated to compare the results from the heel-rise test between groups. The LSI value is defined as the ratio between the involved limb score and the uninvolved limb score, expressed as a percentage (involved limb/uninvolved limb × 100). The Mann-Whitney U test was use to compare the ATRS scores between groups. The independent-samples t test was used for comparing the heel-rise test between groups. The level of significance was set at P < .05.
Results
Descriptive data based on the different studies and treatments can be found in Table 1.
Descriptive Information of the Subjects
Surgical Versus Nonsurgical Treatment
There were no significant differences between the surgical and nonsurgical groups on the patient-reported outcome measure (ATRS) at 6 and 12 months (Table 2). The surgical group had significantly better results compared with the nonsurgical group in heel-rise endurance at 6 and 12 months and heel-rise height recovery at 6 months (Table 2).
Surgical Versus Nonsurgical Treatment a

a Boldfaced values indicate statistically significant differences between groups. ATRS, Achilles tendon Total Rupture Score; IQR, interquartile range; LSI, limb symmetry index.
Sex Comparison
When the entire cohort was analyzed, male patients had a greater improvement in heel-rise height at 12 months (Table 3). Analysis of the surgically treated subgroup demonstrated that females had significantly lower score on the patient-reported outcome (ATRS), but there were no significant sex differences in the heel-rise test (Table 4). Analysis of the subgroup treated nonsurgically demonstrated a trend indicating a higher ATRS score for female patients, but this was not significant (Table 5). At the 12-month evaluation, women had a significantly lower heel-rise height LSI compared with men (Table 5).
Comparison Between Sexes for the Entire Group a

a Boldfaced values indicate statistically significant differences between groups. ATRS, Achilles tendon Total Rupture Score; IQR, interquartile range; LSI, limb symmetry index.
Comparison Between Sexes for Patients Treated Surgically a
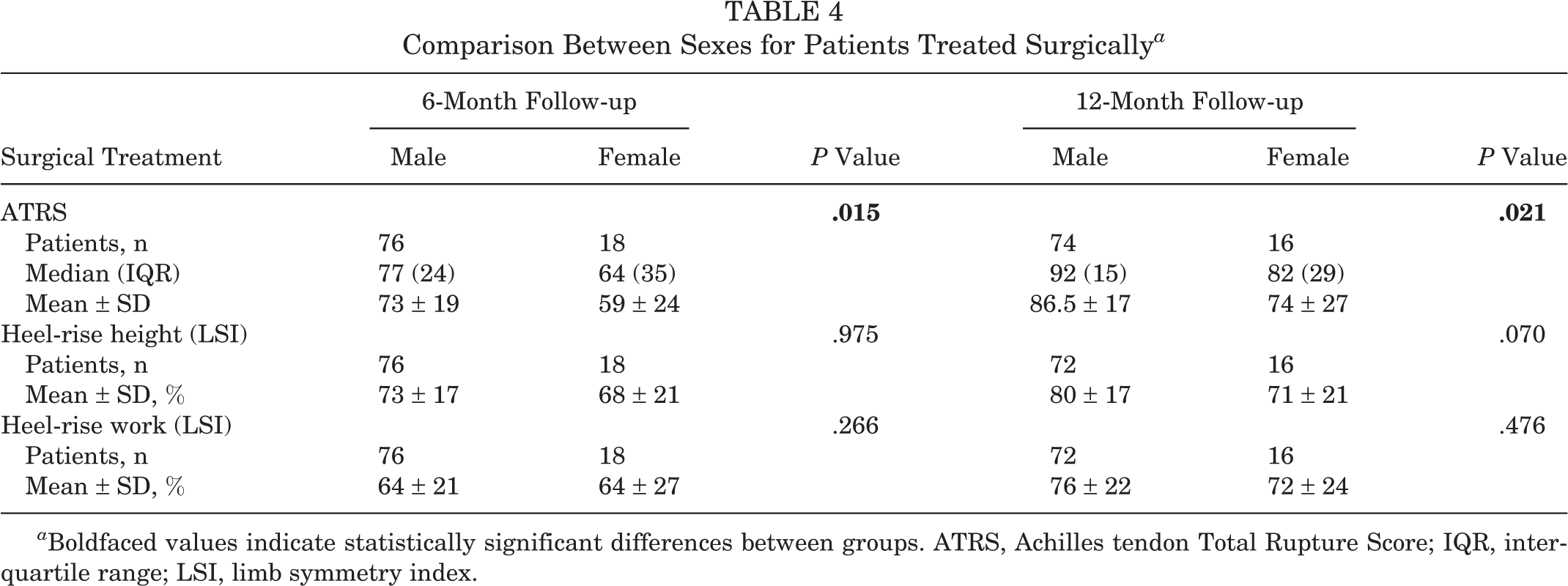
a Boldfaced values indicate statistically significant differences between groups. ATRS, Achilles tendon Total Rupture Score; IQR, interquartile range; LSI, limb symmetry index.
Comparison Between Sexes for Patients Treated Nonsurgically a

a Boldfaced values indicate statistically significant differences between groups. ATRS, Achilles tendon Total Rupture Score; IQR, interquartile range; LSI, limb symmetry index.
Discussion
When comparing the sexes, it was found that males had better heel-rise height at 12 months regardless of treatment, but no other significant sex differences could be demonstrated when the total cohort was analyzed. Females who received surgery had significantly more symptoms than did males, but this was not found in the nonsurgical group. There was no significant difference in symptoms between surgical and nonsurgical treatments, but the surgical group performed significantly better in terms of heel-rise endurance at 6 and 12 months.
Magnusson et al 14 found differences in tendon response to exercise between the sexes. Females had less hypertrophy and collagen synthesis in response to exercise and also lower mechanical tendon strength. Some proposed reasons for such differences are biomechanical, neuromuscular, and hormonal factors. 14,16,27,30 Load-bearing connective tissues of the body (eg, tendons and ligaments) contain heterogeneously distributed receptors that respond to estrogen. 6,16,32 Estrogen has been shown in several studies to have an inhibitory effect on collagen synthesis, and thus, reduces the amount of collagen present in tendons and alters connective tissue metabolism. 6,14,16,30 Whether these factors explain the differences that were found in terms of heel-rise height and symptoms is not known and needs further study.
One surprising finding of this study was that female patients who had surgery reported greater degree of symptoms than did males, but this difference was not found when comparing the sexes in the nonsurgical group. Whether these findings are due to differences in reporting symptoms, tendon healing, or other aspects of healing after surgery needs to be further studied. It has, however, previously been reported that women have a greater risk of wound complications after Achilles tendon repair. 3 Another study found that women were more likely to have predisposing comorbidities, such as systemic steroid and fluoroquinolone antibiotic use, compared with men. 29 However, no major wound complications or documented comorbidities in either sex were noted in the studies included in this analysis. It might also be of interest to determine whether these differences are similar after 2 to 5 years or if the females are just not fully recovered after surgery at 1 year.
A recent systematic review 7 comparing surgical and nonsurgical treatment for Achilles tendon rupture included 7 randomized controlled trials published in the past 10 years. All these studies included both sexes, and the percentage of females in these studies ranged from 14% to 37%. However, none of the studies performed a separate analysis of outcome of males and females. 11,15,18,22,24,28,31 The systematic review concluded that the differences in outcome between surgical and nonsurgical treatment are minor, but it is not known if the results might be different if males and females were analyzed separately. Since it is reported that the incidence of Achilles tendon rupture is increasing in women, future studies should consider controlling for sex when comparing treatments. 8,9,26
Despite combining the data from 2 large randomized controlled trials, the female cohort was still limited. Moreover, the treatments in the 2 different studies were not completely identical, so it is difficult to make any firm conclusions concerning the differences between the sexes. However, the outcome of this study does support previous studies indicating differences between sexes in the recovery from an Achilles tendon rupture. 2,23 Further studies are needed, however, to determine whether treatments should differ between men and women, and it might be relevant to perform separate statistical analyses in randomized clinical trials comparing treatment after an Achilles tendon rupture.
Conclusion
There appear to be differences in outcomes between sexes after Achilles tendon rupture. Female patients had a greater degree of deficit in heel-rise height irrespective of treatment. Females also had more symptoms after surgery both at 6 and 12 months, but this difference was not found in the subgroup treated nonsurgically. Further research is needed to confirm these findings and to determine whether these differences remain in the long term as well as whether males and females should be treated with different treatment protocols.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was supported by the Swedish National Centre for Research in Sports (CIF).