
Abstract
Background:
Randomized studies have so far failed to show a difference in outcome between operative and nonoperative management of Achilles tendon rupture, provided that no rerupture occurs. Percutaneous Achilles repair has been suggested to result in superior patient satisfaction compared with open repair in patients with an acute Achilles tendon rupture, but there are no outcome data available with validated methods describing the progression of recovery during the first year.
Purpose:
To evaluate the outcome of patients with a ruptured Achilles tendon, managed by percutaneous repair, during the first year following repair with a valid, reliable, and responsive outcome measure. Furthermore, the effects of time between injury and surgery, age, and complications on outcome were also evaluated.
Study design:
Case series.
Methods:
A total of 73 patients (60 males and 13 females) with a mean age of 45.5 years were included. Patient age, length of time between injury and surgery, and complications were documented. Patients were evaluated using the Achilles tendon Total Rupture Score (ATRS) at 3, 6, 9, and 12 months following repair.
Results:
The median ATRS results at 3, 6, 9, and 12 months were 42.5, 73, 83, and 89, respectively. The number of patients who reported excellent or good scores (ATRS >84) at 3, 6, 9, and 12 months were 3%, 36%, 57%, and 69%, respectively. There were no significant differences in outcome at each time point for those patients undergoing early (≤48 hours) compared with late surgery or between those <65 and those >65 years of age. The complication rate was 13.5%. Patients who had a complication had a lower ATRS result at 3 months following surgery, but there were no differences after that time point.
Conclusion:
The patients in the present study reported marked improvement in function between 3 and 6 months following surgery, with continuing but less steep improvement up to 1 year following surgery. The presence of a complication other than rerupture did not affect the end-stage outcome but did affect that at 3 months following surgery.
Clinical Relevance:
This study demonstrates improving scores with time over the first year following surgery, against which other treatment methods can be compared.
Randomized studies have so far failed to show a difference in outcome between operative and nonoperative management of Achilles tendon rupture. 6,11,21–23,30,31 A recent study showed improved plantarflexion strength and outcome score at 3 months in patients managed with operative intervention; however, most outcomes were measured at 6 and 12 months following injury. 11 Meta-analyses and systematic reviews have consistently reported reduced rerupture rates for patients managed with operative intervention at the expense of increased incidence of minor complications. 12,15,28,32
Meta-analyses comparing minimally invasive and percutaneous repair with open repair have shown no significant differences in rates of rerupture, tissue adhesion, sural nerve injury, deep infection, and deep vein thrombosis (DVT), while minimally invasive surgery has shown considerably reduced risk of superficial wound infection and a 3-times greater patient satisfaction rate. 13,19
The assessment of outcome following Achilles repair has focused on rerupture rates, complication rates, and patient subjective scores of function. Most scores are determined at a single point of follow-up and restoration of function for the cohort or function at 1 to 2 years following injury and repair.
Several studies have reported functional outcome at 3, 6, and 12 months, 7,14,21,30,31 but these have involved scores with both subjective and objective components. 10 In a systematic review of outcome measures, the Achilles tendon Total Rupture Score (ATRS) was identified as the only injury-specific outcome measure that has been developed and evaluated using recommended methods. 10 Based on the current evidence, the ATRS is the most appropriate outcome measure for evaluating the management of acute Achilles tendon rupture. 10 Functional outcome plateaus at 9 months following the commencement of management, 7 and yet outcome at this time point has rarely been studied.
The outcome of a series of patients with a ruptured Achilles tendon managed by percutaneous repair followed by early functional rehabilitation at 3, 6, 9, and 12 months following repair is reported. The effects of time of surgery, age of patient, and the presence of complications on outcome were also determined.
Materials and Methods
From April 2009 to April 2012, patients diagnosed with a rupture of the Achilles tendon were offered surgical treatment. Diagnosis was made according to the presence of a palpable gap within the tendon, the loss of the normal resting tone of the ankle, and lack of tendon continuity on performing a calf squeeze test. 16 Seventy-six patients requested surgical intervention following counseling regarding management options. Surgical repair was performed using an established percutaneous technique. 3
After the index procedure, patients followed a standardized postoperative protocol. Patients were given analgesics, but the use of nonsteroidal anti-inflammatory drugs was discouraged. Full weightbearing in a functional split synthetic cast in equinus was permitted, with the use of elbow crutches, immediately following surgery. At 2 weeks, the wounds were inspected, sutures were removed, and open kinetic chain mobilization exercises consisting of inversion, eversion, and plantar flexion were commenced by the patient to encourage early movement, improve proprioception, and reduce the formation of adhesions. Dorsiflexion was forbidden. Otherwise, the dorsal shell was left in position during weightbearing secured by either elasticated Velcro straps (Velcro USA Inc, Manchester, New Hampshire) or Tubigrip (Mölnlycke Healthcare, Gothenburg, Sweden) until 6 weeks following surgery (Cretnik A. “Functional Bracing Versus Rigid Immobilization After Percutaneous Achilles Tendon Repair Under Local Anaesthesia.” Presented at the 14th ESSKA Congress, 2010). At that stage, a progressive range of movement, proprioceptive, and strengthening exercise program was commenced. Several modifications to both the surgical technique and perioperative management were made.
Surgical Modifications
A tourniquet was no longer used, given the small incisions of this technique. A small midlateral incision 1.5 cm long allowed exploration, visualization, and mobilization of the sural nerve. This was facilitated by the injection of 5 mL of 0.5% bupivacaine with 1:200,000 epinephrine into this area to reduce bleeding. The aim of this was to reduce the risk of iatrogenic injury to the sural nerve at this site.
Management Modifications
A preoperative dose of intravenous prophylactic antibiotic (1 g flucloxacillin) was used in addition to 2 weeks of a once-daily dose of low-molecular-weight heparin (tinzaparin 5000 IU subcutaneously). Patients were encouraged to walk, and even jog, as comfort and confidence allowed once they were out of the cast. Plyometric exercises and sprinting were not allowed until 3 months following repair.
Follow-up
Patients gave consent for the collection of their demographic details and outcome scores in a database. This allowed continued evaluation of scores and awareness of postoperative complications. Patients were asked to complete a modified ATRS 5 before each outpatient visit at 3, 6, 9, and 12 months following repair.
Comparison
Patient outcomes were compared according to age (younger and older than 65 years), the timing of surgery (within 48 hours and within 7 days of injury), and the presence of surgical complication (those with and without a complication).
Statistical Analysis
For the data analysis of the outcome measure (ATRS), the last observed value was carried forward. There were 7 missing values for ATRS at 3 months, 9 missing values for ATRS at 6 months, 20 values missing for ATRS at 9 months, and 11 values missing for ATRS at 12 months.
Descriptive data are reported as means and standard deviations (SDs) for ratio data, medians and interquartile ranges (IQRs) for ordinal data, or frequencies. For comparisons between groups, the independent t test was used for ratio data, Mann-Whitney U test for ordinal data, and the Pearson chi-square test and Fisher exact test for dichotomous variables. The level of significance was set at P < .05. All data were analyzed using IBM SPSS Statistics 19 (Armonk, New York).
Results
During the 3-year patient enrollment period, 76 patients chose to undergo percutaneous repair of their Achilles tendon at Princess Royal Hospital, Telford, Shropshire, United Kingdom. Of those 76 patients, 2 were excluded from analysis because they were lost to follow-up prior to the 3-month evaluation and therefore there were no outcome (ATRS) data available. One patient had a rerupture at 8 weeks after injury and was not included in further analysis. The 3 excluded patients were all Caucasian males, with a mean (SD) age of 40 (11) years. Two had injured the right side and 1 the left side. The injury mechanism was sport for 2 of the patients and during activities of daily living (ADLs) for 1 patient.
The continued evaluation included 73 patients. Their demographic details are typical for a cohort of patients who have sustained a rupture of the Achilles tendon (Table 1). There was a bimodal age distribution (Figure 1). The most frequent activity during which the tendon ruptured was playing football (n = 16); other sports included badminton (n = 11), running (n = 6), rugby (n = 5), and squash (n = 4). All but 2 patients underwent surgery within 14 days of injury (mean, 6 days; range, 0-20 days).
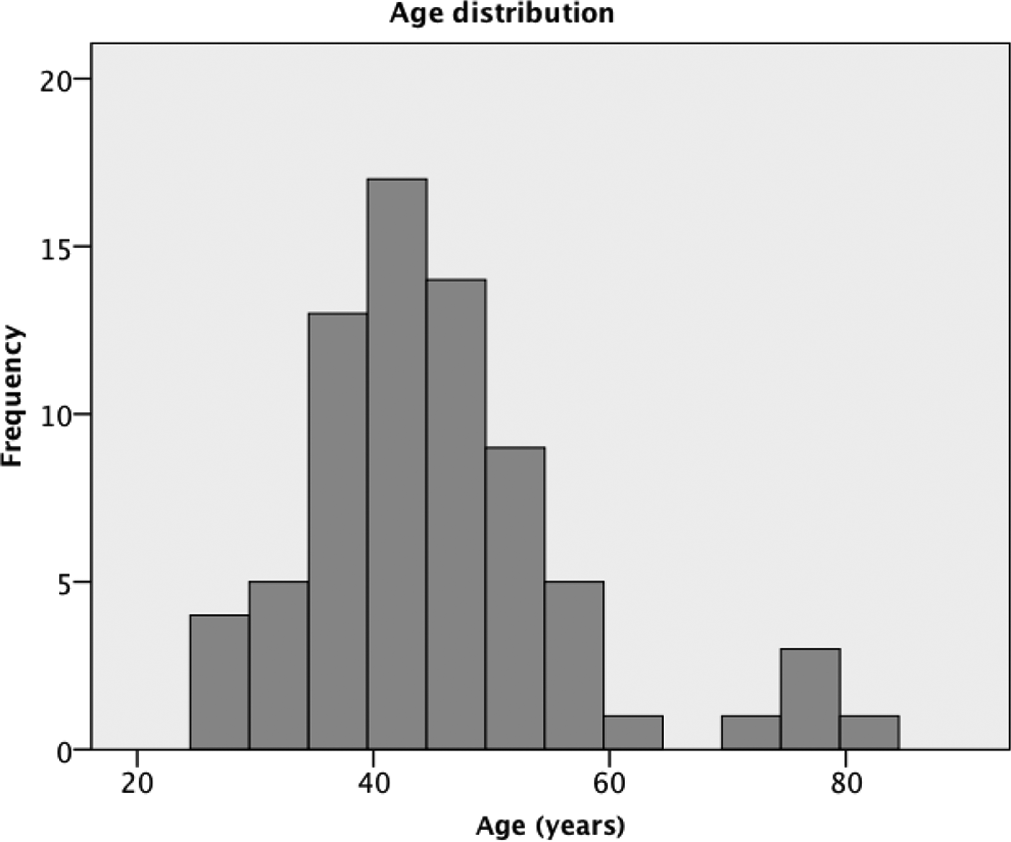
Bimodal age distribution.
Descriptive Statistics of the Study Population (N = 73) a

a ADLs, activities of daily living; SD, standard deviation.
Median ATRS results at 3, 6, 9, and 12 months are reported in Table 2 (Figure 2). The number of patients who reported excellent or good scores (ATRS >84) at 3, 6, 9, and 12 months were 3%, 36%, 57%, and 69%, respectively.

Patient-reported outcome, Achilles tendon Total Rupture Score (ATRS) over the first year following repair.
Patient-Reported Outcome (ATRS) a

a Values are expressed as median (interquartile range). ATRS, Achilles tendon Total Rupture Score.
Timing of Surgery
In all, 7 patients were treated within 48 hours and 50 patients within 7 days of injury. There were no significant differences between the groups in either time period (≤48 hours and <7 days of injury) concerning age, sex, injured side, mechanism of injury, or outcome (Table 3).
Comparison Between Patients Treated “Early” and “Late” a

a Values are expressed as median (interquartile range). ATRS, Achilles tendon Total Rupture Score; NS, not significant.
Patient Age
In this study, there was a bimodal age distribution. There were 5 patients aged 65 years and older. The older age group sustained rupture during ADLs rather than during sport (P < .00). There was also a significant difference for sex between the 2 age groups (Table 4). There was no significant difference in outcome at any time point.
Comparison Between Age Groups a

a ATRS, Achilles tendon Total Rupture Score; ADLs, activities of daily living; IQR, interquartile range; NS, not significant; SD, standard deviation.
Influence of Complications
Overall, 10 patients sustained complications on outcomes. There was 1 case of traumatic rerupture, 4 cases of sural nerve injury, 2 cases of superficial infection, 2 DVT, 1 prominent suture knot, and 1 patient had adhesions. One patient experienced a traumatic rerupture at 8 weeks following the initial repair and was excluded from further analysis. At open repair, reconstruction suture material was seen to pass through the sural nerve. Thus, this patient actually had 2 complications. One patient had a fatigue partial rerupture at 6 months following repair. The ATRS results of these patients are presented in Table 5. The overall incidence of patients having complications in this series is 13.5%, assuming a worst-case scenario.
Influence of Specific Complications on ATRS a

a ATRS, Achilles tendon Total Rupture Score; DNA, did not attend.
There was no significant difference in the demographic details of patients suffering complications compared to those without complications, and notably, there was no significant difference in outcome other than reduced outcome score in those sustaining a complication at 3 months (P = .005) (Table 6).
Comparison Between Patients With and Without Complications a
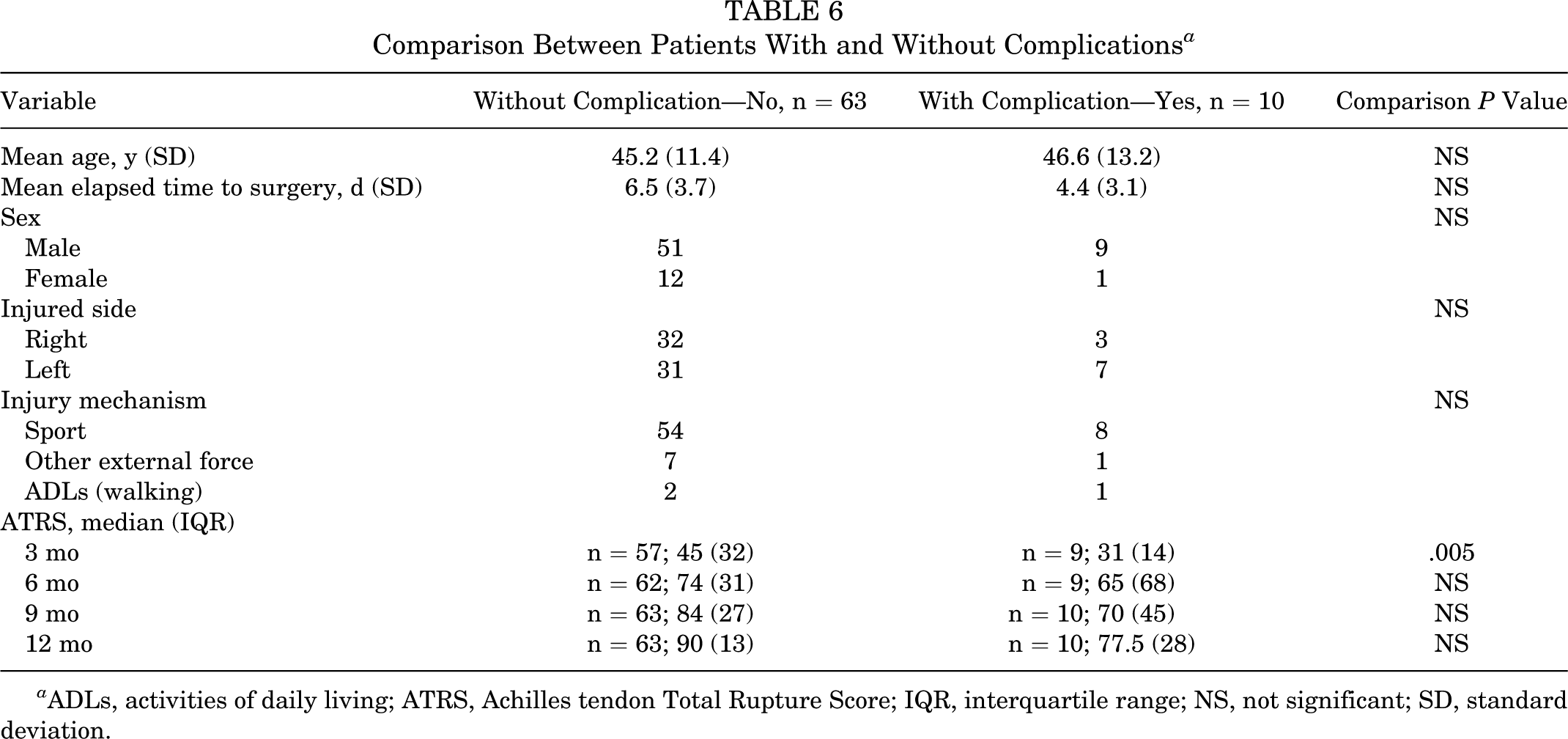
a ADLs, activities of daily living; ATRS, Achilles tendon Total Rupture Score; IQR, interquartile range; NS, not significant; SD, standard deviation.
Discussion
The main finding of the present investigation is that patients reported marked limitation of function by 3 months, little limitation of function by 6 months, and a near excellent/good outcome at 9 months following surgery. The greatest improvement in function happened between 3 and 6 months following surgery. The success of this treatment method is similar in younger and older patients, and the timing of surgery within a week of injury does not appear to influence the results. This method of percutaneous repair of the Achilles tendon rupture is a reliable and reproducible method of restoring good function, with minimal limitation or complications.
Several studies have assessed outcomes using the ATRS following its development. 9,17,18,20,22,24–26 In one randomized controlled study, ATRS results at 6 and 12 months were 72 and 88 for operative repair and 71 and 86 for nonsurgical management, respectively, which are almost identical to those reported in this series. 22 Olsson et al 25 found a comparable score of 38 at 3 months of follow-up and showed that heel rise ability was an important early factor and was reflective of patient-reported outcome and physical activity.
Several outcome studies have been performed using ATRS at a single time point. Metz et al 20 reported follow-up at a mean of 6.2 years after injury with a mean score of 84. Maffulli et al 18 reported good outcome in athletes, satisfactory outcome in elderly individuals (ATRS 69.4 at 7 years after repair), 17 and recently in a small cohort of the general population, an ATRS of 84 at a mean of 26 months following surgery. 9 These studies are useful for comparison as they feature a similar surgical technique.
Möller et al, 21 Twaddle et al, 30 Keating et al, 11 and Chandrakant et al 7 have all reported on early clinical evaluation at 3 months followed by long-term evaluation. Möller et al 21 showed incremental increases in visual analog score and a specifically developed functional index lower limb score, which almost decreased in value by one-half between 6 months and a year. Twaddle et al 30 assessed patients at 8 weeks and at 6 and 12 months and reported increasing function using the Musculoskeletal Functional Assessment Index, with scores of 15.2, 7.8, and 3.4, respectively. In the series by Keating et al, 11 the Short Musculoskeletal Functional Assessment at 3 months showed improved outcome in surgically treated patients (P < .03). Recently, Chandrakant et al 7 reported increasing American Orthopaedic Foot and Ankle Society (AOFAS) scores at 6 weeks and at 3, 6, and 12 months following repair, with a trend toward statistical significance between the AOFAS Ankle-Hindfoot scale and the time to reach a plateau of improvement (r = −0.2, P = .06). All of these scores show comparable changes in value during the first year, but the present study is the first to report Achilles tendon rupture–specific subjective functional outcome scores at 3, 6, 9, and 12 months following surgery using the ATRS. Thus, this study demonstrates improving scores with time over the first year following surgery, against which other treatment methods can be compared.
Silbernagel et al 27 and Olsson et al 25 recently commented that since strength deficits remain at 1 and 2 years following surgical management, treatment should be focused on improving function in the first year following surgery. Chandrakant et al 7 commented that the functional outcome of patients plateaus at 9 months following surgery and yet did not report outcome at this time point. Schepull et al, 26 however, commented that there may be a ceiling effect of the ATRS, which may influence outcome scores. Ongoing follow-up beyond 12 to 24 months has shown significant increases in ATRS (85-89; P = .017) in patients with Achilles tendon ruptures treated nonoperatively, whereas patients managed surgically did not report a significant increase in the ATRS (89-90; P = .321). 24 These small improvements may suggest that the ATRS may plateau beyond this 1-year time point.
Quenu and Stoyanovitch commented, “Achilles tendon ruptures should be operated on and without delay.” 29 Since then, Carden et al 2 recommended that repairs be performed within 48 hours of injury to improve outcome. It is generally recommended that percutaneous repairs are performed within 2 weeks of injury to reduce the risk of adhesion formation in the retracted state and to prevent end-to-end juxtaposition. 4 In this series, almost all patients were operated on within 14 days of injury. The outcomes of those operated within 48 hours of injury (n = 7) and within 7 days of injury (n = 50) were compared; we found that neither of these time points influenced the outcome. This would suggest that for percutaneous repair, as long as tendon end opposition occurs, patients do not benefit from urgent surgery.
Achilles tendon ruptures have a bimodal distribution, with a first peak of predominantly males (ratio, 16.7:1) in their fifth decade and a second peak of a much lower male to female ratio (1.6:1) in their seventh decade. 8 The current series reflects a second peak of predominantly female patients. Bergkvist et al 1 recently suggested that elderly female patients may benefit more from surgical intervention. Cretnik et al’s 8 series of 14 ruptures in patients over 60 years of age had a mean AOFAS score of 93.1 points, whereas Maffulli et al’s 17 series suggested reduced functional outcome with an ATRS of 69.4 at a mean follow-up of 49 months. Although the number of patients over 65 years of age in this series is small (n = 5), they do report relatively good outcomes based on ATRS. This was principally due to the patients reporting that factors other than their Achilles tendon caused limitation in activities. This age group tended to rupture their Achilles tendon during ADLs.
Using the ATRS, Metz et al 20 retrospectively studied patients who underwent minimally invasive repair; the mean ATRS was 84 for 211 patients, with a mean follow-up of 6.2 years (range, 3-10 years). Those patients without complications (64%) had an ATRS of 89, whereas those who sustained rerupture (8%) had a score of 71, those with sural nerve injury (19%) had an ATRS of 79, and those with a minor wound healing problem, for example, infection, had an ATRS of 80. Although complication rates are low (13.5%) in this series, they lead to lower ATRS results at 12 months. Patients with a sural nerve injury scored 75, those with infection scored 78.5, those with DVT scored 86.6, and those with adhesions scored 89. These were only significantly lower than the group without complications at the 3-month time point (P = .005). This may be due to the psychological influence of the complication and its influence on the score. At this time point, all patients were aware of their complication and yet had not showed the dramatic improvement in recovery noted between 3 and 6 months. The ATRS does not specifically score for the presence or absence of complications. The patient who had a traumatic rerupture underwent an augmented open repair using hamstring tendon at week 8. The ATRS for this patient was 55 at 12 months following surgery, but by 2 years the patient had returned to golf and walked without a limp.
The knowledge of the impact of complications is useful during the consent process, as patients can be counseled that, should a complication occur, it would be unlikely to affect the long-term outcome unless the patient sustained traumatic rerupture.
Strengths of this study are that it reports outcome in a systematic and validated fashion in a large population of patients. To avoid bias based on missing data, the data from the last assessment were carried forward prior to statistical analysis. This method gives a conservative estimate of the outcome at each time point, and still the data were comparable to that reported previously.
There are several limitations in this series. The first is the absence of a control group managed with the same accelerated rehabilitation pathway; however, this was restricted by patient choice for treatment. This means that we are unable to report direct comparisons of functional outcome. The second relates to the functional scoring of patients at 3 months from surgery. Two of the questions asked in the modified ATRS relate to the patient’s limitation with running and to jumping activities. In the rehabilitation protocol used, patients were asked to walk and jog as comfort and confidence allowed but to avoid plyometric exercises such as jumping and sprinting until after 3 months. Although many authors state that their athletes return to play within 6 months, 18 a consensus of experienced surgeons has stated that this is not recommended until 6 months. Three months is the time duration of a cycle of collagen healing and maturation; therefore, this was selected as a suitable time period to allow remodeling to occur (Muffuli N, Van Dijk CN, Calder J, Doral M. “Achilles Tendon Injuries: Return to Sport.” Presented at the 6th EFOST Congress, 2010). Olsson et al 25 found that, at this time point, 3 months following repair, only half of patients were able to perform a single leg heel rise. As the ATRS allocates 2 questions worth a total of 20 marks for running and jumping, patients reported limitation in this score for these questions based upon their current activity.
Conclusion
Following percutaneous repair of the Achilles tendon, patients report a marked improvement in function between 3 and 6 months following surgery, with continuing but reduced improvement up to 1 year following surgery. The majority of patients reported excellent or good scores beyond 6 months following repair and an ATRS results of 89 at 1 year. Urgent surgery (≤48 hours) did not result in improved early or end-stage outcome compared to prompt surgery (≤7 days) for percutaneous repair. The presence of a complication other than rerupture did not affect end-stage outcome but did affect outcome at 3 months following surgery.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.