
Abstract
Cheerleading is a highly popular youth sport in the United States and has been increasingly recognized in recent years for its athleticism and competitive nature. The sport has changed dramatically since its inception. When the sport of cheerleading was first developed, its primary purpose was to entertain crowds and support other athletes. Today, cheerleaders are competitive athletes themselves. Cheerleaders, most of whom are in the pediatric age group, and their parents commonly approach orthopaedic surgeons and sports medicine physicians with questions regarding the risks associated with participation in the sport. Appropriate clinical guidance is especially important for athletes returning to the sport after an injury. However, unlike other popular sports (eg, football, basketball, and volleyball), the intricacies of cheerleading are not well-known to those outside the sport, including many health care providers. Previous studies have reported on the epidemiological patterns of injuries associated with cheerleading and how such aesthetic sports affect the body, finding that fractures and concussions are prevalent and that catastrophic injuries are more common than in most other sports. Here, we provide an evidence-based discussion of 10 pertinent topics regarding cheerleading and its risks to the musculoskeletal system. The purpose of this review is to provide a comprehensive resource for orthopaedic surgeons and sports medicine physicians who care for these athletes.
Cheerleading attracts approximately 4 million participants annually in the United States. 141 Despite its more than 100-year history, cheerleading has only recently been considered a sport by the public and regulatory organizations, as the athleticism required of its participants has become evident through social media and docuseries. 54,131 Cheerleading involves the performance of various complex skills that contribute to its categorization as a high-risk sport for injuries. 7
Each year, approximately 35,000 cheerleading-related injuries, most commonly involving the extremities, are treated in emergency departments across the United States. 172 Specifically, cheerleading accounts for 65% of all catastrophic injuries—defined as severe spinal, spinal cord, or cerebral injuries—occurring in female athletes. 9,102 Such catastrophic injuries present acutely, but most injuries sustained in cheerleading are chronic and related to overuse. 144 Most cheerleaders fall into the pediatric age group, and they and their parents often approach their medical teams with questions regarding the injury profile specific to cheerleading.
The purpose of this review was to synthesize the available literature and present evidence-based guidance to orthopaedic surgeons and sports medicine physicians for the treatment and counseling of cheerleaders. To improve understanding of the circumstances of injury and how to approach the cheerleader as a patient, we provide evidence-based discussion of 10 pertinent topics regarding cheerleading and its risks to the musculoskeletal system.
Understanding the Context of Cheerleading Injuries
Cheerleading is uniquely defined by its combination of stunting and tumbling. A stunt is any skill in which a top person (flyer) is supported above the performance surface by 1 or more persons, commonly 2 bases and 1 backspot (Figure 1A). Stunts can be static, in which the flyer is held in one position (as in partner stunts) (Figure 1B), dynamic (as in airborne basket tosses) (Figure 1C), or both. Classically, pyramids that involve the connection of multiple stunts have both static and dynamic elements occurring in sequence (Figure 1D). Tumbling—or any hip-overhead skill not supported by a base that begins and ends on the performance surface—is an aspect shared with gymnastics. Skills vary in difficulty from cartwheels and handstands to combination passes involving the sequential performance of multiple skills. Routines also typically include coordinated dance movements and jumps (Appendix Table A1).

Illustration of cheerleading stunts. (A) Prep-level group stunt demonstrating basic stunt positions: a, top person/flyer; b, bases; and c, backspot. (B) Extended, single-leg partner stunt involving 1 female flyer and 1 male base. (C) Airborne toe-touch basket toss. (D) Two-and-one-half-high pyramid.
Three main types of cheerleading exist: recreational, scholastic, and all-star. 158 Although all types involve similar skills, they differ in setting and primary focus. Recreational and scholastic (including collegiate) types of cheerleading are affiliated with community youth organizations, such as the Pop Warner Little Scholars and schools, respectively. 156 These types may be competition-based (competing against other cheerleading teams), gameday-based (supporting another athletic team, most commonly football or basketball), or a combination of both. 156,158 Meanwhile, all-star cheerleading is strictly competitive and practiced in private gymnasiums. 156
In addition to the required athleticism, several other factors inherent to cheerleading contribute to high risks for injury and reinjury. Similar to athletes of other aesthetic sports (ie, sports in which scoring depends on subjective evaluation of skill competency and presentation), cheerleaders generally reach their athletic peak in their teens, typically between ages 12 and 18 years. 47,68,80,154 Cheerleading is also unique in that opportunities to pursue the sport professionally are limited because most teams affiliated with professional sports organizations, such as the National Football League or National Basketball Association, are actually dance teams without the tumbling and stunting components of cheerleading. 31 These circumstances, along with the inability of a team to perform a coordinated routine in the absence of any single member, put cheerleaders on an accelerated timeline for skill acquisition and injury recovery. This timeline may lead to impatience regarding skill training and progression, lack of compliance with return-to-sport guidelines after injury, and initiation of the sport at a young age. Additionally, cheerleading is a year-round sport without an off-season. 167 Currently, >30 states classify competitive high school cheerleading as an official interscholastic sport, which enables consistent safety regulation, training for coaches, and access to resources 53,104 (such as athletic trainers) that reduce the risk of injury. A new form of competitive collegiate cheerleading, called STUNT, has been recently named an emerging sport by the National Collegiate Athletic Association (NCAA). 157 However, cheerleading itself is not currently sanctioned as an NCAA sport nor is it recognized by Title IX guidelines. 54,157
Sports Medicine Essentials for Cheerleaders
1. Health Benefits
The high level of athleticism demanded by cheerleading involves endurance and strength training. 3,148 This athleticism contributes to cardiovascular and muscle fitness, 148 leading to a healthier cardiovascular profile in adulthood and a lower rate of early death from chronic diseases. 16,123 Cheerleading also has positive effects on bone formation and bone strength. 111,118 Cheerleaders measure substantially higher in all bone strength outcomes, including cortical content, compared with adolescents not exposed to high-impact activities. Improving bone strength in adolescence may prevent age-related osteoporosis. 50,169 In addition, for women, the culture of a structured, female-dominated sport may reduce the risks of future substance dependence, learning and memory impairments, and unintentional injury or death. 22,92,95,97
2. Health Risks
The combination of high-impact activities, negative social pressures, and immature physiological characteristics of young athletes can put cheerleaders at risk for conditions that can predispose them to orthopaedic problems. Relative energy deficiency in sport (RED-S)—a syndrome resulting from low energy availability—presents more frequently in athletes participating in aesthetic sports, such as cheerleading, than in athletes participating in nonaesthetic sports. 105,147
Energy availability is a concern for all growing athletes and can be affected by disordered eating behaviors. 45 The appearance demands of cheerleading are well-recognized and embedded in the culture of the sport, with cheerleaders reporting high rates of body dissatisfaction (46%) and disordered eating (33%). †† Cheerleaders, particularly those competing at elite levels, are at higher risk of low energy availability. 93
In RED-S, the inadequacy of energy impairs physiological function, most pertinently menstrual function and bone health. 99 Up to 33% of female cheerleaders report some form of menstrual dysfunction, which can present as amenorrhea or oligomenorrhea. 147 The associated low-estrogen state in women may affect normal skeletal development by decreasing bone mineral density (BMD). 35,85,106 Eating disorders and low testosterone levels in men are similarly associated with low BMD, so cheerleaders of both sexes are susceptible. 96 Low BMD may negate the positive effects of weightbearing exercises on bone strength. 21,28,81 Building BMD is most crucial during childhood and adolescence because approximately 90% of peak bone mass is accrued before 18 years of age 2 ; therefore, any conditions that impair bone mass accrual can increase later risk for stress fractures, acute fractures, and osteoporosis. 49 Therefore, orthopaedic surgeons and sports medicine physicians should be cognizant of risk factors for low BMD and counsel patients on the importance of healthy eating habits, current bone health, and its implications for future musculoskeletal injury. 38,49 Cheerleaders who have low BMD or are at risk for developing low BMD should be referred to a sports medicine physician who understands this condition and its treatment.
Patients who present with dysmenorrhea (ie, painful menstrual cramps) should be evaluated for pelvic floor dysfunction, because cheerleaders are at risk from the performance of high-impact maneuvers. 17,23 Pelvic floor dysfunction is associated with urinary and anal incontinence, sexual dysfunction, and reduced quality of life. 94,145 Referral to a gynecologist, gastroenterologist, or specialized physical therapist may be recommended.
3. Musculoskeletal Injury Patterns in Cheerleading
The incidence of cheerleading injuries is approximately 0.67 to 2.8 per 1000 athlete-exposures, with 1 athlete-exposure defined as 1 cheerleader participating in 1 cheerleading event. 128,136 Despite the low incidence of injury, mean sport participation time lost per injury is 29 days, with 78% of cheerleaders experiencing at least 1 injury during their athletic career. 1,67 Injuries occur more frequently during competition than during practice, and the most common mechanisms of injury are basing or spotting a stunt, falling, failing to complete a skill, tripping or twisting a body part, and colliding with another cheerleader. 163 Overuse injuries account for 66% of all cheerleading-related injuries treated at sports medicine clinics, 144 often presenting as a gradual onset of unspecified chronic pain. 20,33
The most common body areas injured are the ankle (22%-45%), wrist or hand (16%-21%), back (9.2%-16%), and knee (8.4%-15%). 39,66,67 The ankle is prone to sprains of the anterior talofibular or calcaneofibular ligaments and talar osteochondritis dissecans. Wrist and hand injuries often involve the interosseous ligaments, triangular fibrocartilage complex, distal radius (epiphysiolysis or gymnast’s wrist), or scaphoid (fractures). 59,62,66,67,110,128 The high frequency of ankle and wrist/hand injuries results from force overload on the joints given the weightbearing nature of tumbling and stunting. 24,39,136,162 The lower back is susceptible to muscle strains and pars interarticularis stress reactions, progressing to spondylolysis with or without spondylolisthesis, from the repetitive flexion, hyperextension, rotation, and compressive loading involved in tumbling and basing stunts. 59,87,98,121 One study 136 found that 66% of cheerleading-related recurrent injuries occurred around 1 of these 3 body areas. Knee injuries can present chronically as patellofemoral syndrome, Osgood-Schlatter disease, or patellar tendonitis or acutely as injury to the anterior or posterior cruciate ligaments (Appendix Table A2). 63,120
Overuse through large joint range of motion can result in shoulder pain or instability or hip flexor tendonitis caused by the increased muscle strength required to overcome soft tissue laxity associated with the joint hypermobility often seen in these athletes. 62,136,164 These conditions can manifest from cheerleading’s high range of motion and skill-landing strategies requiring joint control and force resistance. 46 The upper extremity weightbearing activities of cheerleading are further associated with stress fractures, with bones exposed to forces equal to as much as 12 times the cheerleader’s body weight. 81 Stress fractures most frequently occur in the upper extremity distal to the elbow. 139 Acute fractures also occur most commonly in the upper extremity, often secondary to falls on an outstretched arm. 68,90,126 Of cheerleading-related injuries treated at emergency departments nationwide, 14% to 17% were acute fractures; 62% of these fractures involved the upper extremity. 68,103,134 Other acute musculoskeletal presentations include soft tissue injuries (hematomas, contusions, crush injuries, and abrasions; 12%-22%), lacerations and avulsions (3.2%-6.0%), and acute dislocations (2.0%-2.2%). 62,68,103,128,134 The incidence of these injuries is likely higher than noted here because only approximately 28% of cheerleading injuries are treated in an emergency department. 55,128
4. Catastrophic Injuries in Cheerleading
The National Center for Catastrophic Sport Injury Research defines a catastrophic injury as any severe spinal, spinal cord, or cerebral injury incurred during sports participation. A mean of 3.6 catastrophic injuries per year were reported for cheerleading between 2002 and 2017, increasing from 1.95 injuries per year between 1982 and 2002. 9,173 Although the incidence is low, cheerleading accounts for 54% of all direct catastrophic injuries to female high school athletes and 56% to female collegiate athletes. 101 These injuries most often occur in the setting of stunts, particularly pyramid and basket tosses, when flyers fall from heights and land on the floor or their bases. 5,57 More than half (52%) of catastrophic cheerleading injuries occur to the head, often resulting in cerebral edema, hematoma, or skull fracture. 9 Approximately 54% of these injuries lead to permanent disability. The next most common catastrophic injury involves the cervical spine (32%), with 29% of such injuries resulting in permanent disability. 9 These injuries include cervical fractures, severe ligament injury, or spinal cord injury. 9 Injuries to other sections of the spine and internal organs, such as the lungs and heart, are less common. 40,173 Fatal injuries are rare. 9,100,102
5. Spotlight on Concussions
The incidence of concussions sustained by cheerleaders is 0.02 to 0.33 per 1000 athlete-exposures. 26,114,127 Similar to the risk of sustaining a catastrophic injury, the risk of sustaining a concussion in cheerleading has increased as the sport has evolved in difficulty and complexity. 103,134,172 This increase may also be related to greater reporting and awareness of concussions in recent years, as seen with other sports. 119 The national incidence of concussion has increased by >900% since 2000, from approximately 600 concussions that year (2.7% of all cheerleading injuries presenting to US emergency departments) to approximately 5500 concussions (18%) in 2019. 9,103,134,172 Of note, cheerleading’s concussion rate has continued to increase while the sport’s overall injury rate has decreased. 172,173
Concussions are the most common head injury in cheerleading, and 96% are secondary to stunt-related incidents. 132,133 When a stunt fails, flyers may fall from a height and hit their head on a hard surface, like a hardwood floor or concrete. Bases may similarly experience concussions if they are struck in the head by a falling flyer. 102 More concussions are reported during practices than during competitions, which may be explained by the lower regulation of practice surfaces and significantly higher proportion of time spent during practice each season. 68,103 Overall, cheerleaders are at high risk for repetitive head contact. Even subconcussive impacts are associated with lower neurocognitive functioning in adolescent athletes if they occur repeatedly. 151,153 Thus, it is essential to follow a graduated return-to-sport protocol to allow the brain to heal fully and minimize occurrence of second impact syndrome.
6. Risks of Starting Cheerleading at a Young Age
Participants can now begin cheerleading as young as 3 years of age, albeit at lower skill and competition levels than their older counterparts. Younger athletes (<12 years) have double the risk of moderate or severe injury, with 46% of their injuries falling into this category versus 28% for older athletes. 58 Cheerleaders younger than 12 are more susceptible to upper extremity fractures and dislocations than are their older counterparts. 76,122,134 The developmental stage of children younger than 12 years may explain their vulnerability to injury. Having not yet reached skeletal maturity, open physes are more susceptible to injury, and pediatric bone is structurally weaker and less dense than adult bone. 34,51 Increases in height and weight at this age may lead to a higher injury risk secondary to decreased proprioception and body awareness while performing demanding skills. 24 These athletes have not yet reached cognitive maturity, which is associated with decreased ability to plan movements and react to sensory stimuli. 14 Of note, the higher rates of severe injury in younger cheerleaders can be at least partially attributed to the learning curve associated with developing skills in a new athlete. Early specialization in a particular sport is further associated with higher risk for overall injury and overuse injury, a consideration for cheerleaders who hope to pursue the sport at high levels. 69,70,115
7. Injury Profile of All-Star Versus Scholastic Cheerleading
The incidence of cheerleading injuries per 1000 athlete-exposures increases from 0.5 in middle school to 0.9 in high school and 2.4 in college. All-star cheerleading has an injury incidence of 0.8 per 1000 athlete-exposures. 133 Although all-star cheerleading is more competitive, collegiate athletes are 3 times as likely to sustain a concussion and 5 times as likely to experience a catastrophic injury than are other types of cheerleaders. 9,133,135 These differences may be explained by the collegiate level’s incorporation of more advanced stunts, such as flipping basket tosses and two-and-one-half-high pyramids, that are not allowed at lower scholastic levels and are used only at the highest all-star levels (Appendix Table A1). 132 Although stunts are the most common mechanism of injury for all types of cheerleading, all-star athletes are more likely to be injured via tumbling. 133,136 This greater risk may be explained by the incorporation of more complex tumbling skills attributable to the use of a spring floor, similar to a gymnastics floor, versus harder surfaces, such as a basketball court in scholastic cheerleading.
8. Injury Profile of Bases Versus Flyers
Cheerleading requires every athlete to participate in stunts, tumbling, jumps, dance, and other aspects of a routine. Therefore, stunt position (base or flyer) is the main determinant of injury risk. Backspots are included as bases here. Contrary to common perceptions, bases have a higher rate of stunt-related injury (34%-46%) compared with flyers (30%-39%). 26,132,172 Injuries to bases most frequently occur to the head and neck (21%), knee (10%), and lower back (9%) as a result of improper technique in tossing, lifting, or catching. 132 Injuries to flyers most often occur to the head and neck (49%), followed by the upper extremity (20%), and result from falls. 135 Most concussions sustained by bases result from contact with another athlete, whereas most concussions sustained by flyers result from contact with the ground. 26 Because of their exposure to heights during stunts, flyers are at greater risk than bases for catastrophic injury. In fact, 70% of catastrophic injuries sustained during cheerleading occur to flyers. 173
9. Injury Profile of Cheerleading Versus Other Sports
Compared with other sports, cheerleading most closely resembles gymnastics. Both involve tumbling and substantial impact on the upper and lower extremities, leading to similar susceptibility to and patterns of injuries. 38,90,139,144 However, the added stunt component in cheerleading is associated with a higher risk for concussions and catastrophic injuries compared with gymnastics. 9,100,103,134,138
Regarding overall injury, cheerleading accounts for only 1.2% of annual sport-related injuries and ranks 18th of 22 high school sports for injury rate per 1000 athlete-exposures. 26,102 The risk of concussion was historically low, with rates similar to low-contact sports such as softball and track and field. 26,74,114,128,174 However, with increased reporting of injuries after formal recognition of cheerleading as a high school sport, recent data have indicated that cheerleading has surpassed football in concussion and catastrophic injury risk. 15,25,102,152,170 Cheerleading is associated with the highest number of direct catastrophic injuries, or those resulting directly from sports participation, for all high school and collegiate sports in which women participate. 5 Fewer data exist for male cheerleaders than for female cheerleaders or male athletes of other sports. Per proportion of overuse versus acute injuries, cheerleading ranks behind tennis, swimming, dance, running, and track and field. 144 Cheerleading presents a similar risk for lower extremity stress fractures as running and basketball, all 3 of which are higher risk than other high-impact sports. 38
10. Preventive Measures
Most methods to prevent injury and improve safety in cheerleading must occur at the administrative level from national cheerleading organizations and other institutions. These actions include establishing regulations for stunts and tumbling, hiring coaches with appropriate certification, ensuring facility safety, enforcing proper skill-technique training, designating cheerleading as an official sport, and providing access to appropriate medical resources. ‡‡
Athletes can take certain actions to reduce their risk of injury and reinjury. Patients should be advised on the following:
Understand the symptoms of concussion and be aware of the development, presentation, and timeline of concussions after a head injury.
Seek medical guidance after a musculoskeletal injury and perform rehabilitation exercises targeting the muscles around the joint to reduce laxity, increase stability, and avoid reinjury.
Incorporate appropriate rest and recovery into training schedules because excessive practicing increases injury from overuse, fatigue, and use of improper technique. Athletes should not practice more hours per week than their age (eg, no more than 5 hours per week for a 5-year-old cheerleader), and, if possible, they should take at least 1 month off from the sport per year. 69,70,115
Practice proper nutrition for adequate energy availability, including intake of protein, calcium, and vitamin D for bone and muscle healing.
Be patient with skill progression. Rapid progression or skipping simpler skills to compete at higher levels raises the risk of injury from poor technique.
Follow return-to-sport guidelines set by professionals after injury or surgery. Refer to Appendix Table A2 for evidence-based recommendations after common cheerleading injuries.
Obtain annual physical examinations and laboratory tests, if indicated, to screen for any predisposing factors to injury, such as low BMD.
Conclusion
This review provides orthopaedic surgeons and sports medicine physicians a basic understanding of cheerleading and answers to potential patient questions regarding the sport. Although overall injury incidence is low, concussions and musculoskeletal injuries are common. Cheerleading also accounts for the highest number of catastrophic injuries to female athletes and carries an especially high risk for RED-S. Cheerleaders should be advised about the importance of appropriate training and health behaviors, as well as rehabilitation and return-to-sport guidelines after injury.
Footnotes
Acknowledgment
The authors thank Paul D. Sponseller, MD, MBA, for recognizing the importance of a review on cheerleading and recommending its creation. For editorial assistance, we thank Jenni Weems, MS, Kerry Kennedy, BA, and Rachel Box, MS, in the editorial services group of The Johns Hopkins Department of Orthopaedic Surgery.
Final revision submitted September 1, 2021; accepted September 27, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.J.B. has received education payments from Arthrex and hospitality payments from Smith & Nephew. R.J.L. has received education payments from Arthrex and hospitality payments from Vericel. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
APPENDIX
Common Cheerleading Injuries a
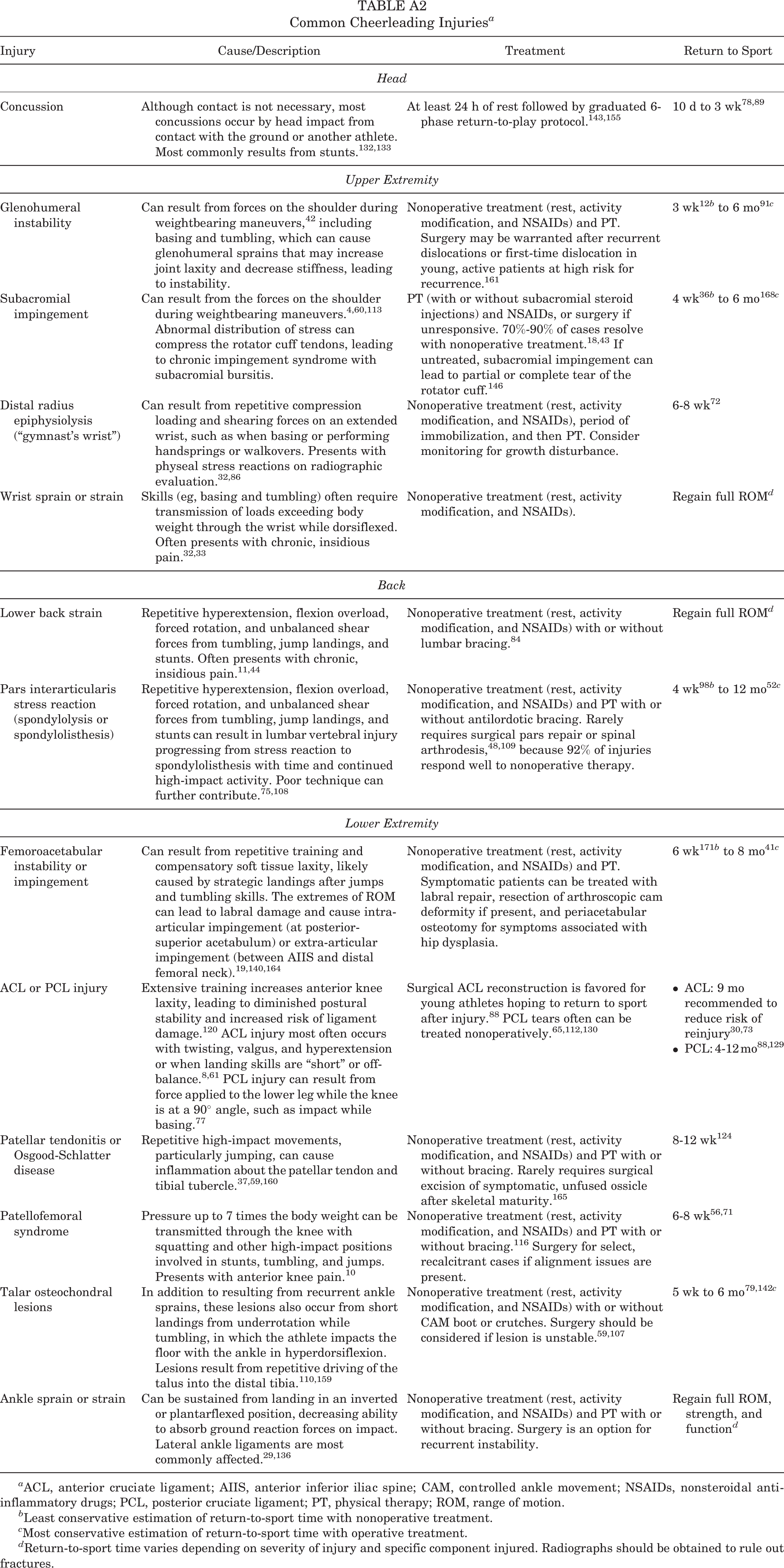
| Injury | Cause/Description | Treatment | Return to Sport |
|---|---|---|---|
| Head | |||
| Concussion | Although contact is not necessary, most concussions occur by head impact from contact with the ground or another athlete. Most commonly results from stunts. 132,133 | At least 24 h of rest followed by graduated 6-phase return-to-play protocol. 143,155 | 10 d to 3 wk 78,89 |
| Upper Extremity | |||
| Glenohumeral instability | Can result from forces on the shoulder during weightbearing maneuvers, 42 including basing and tumbling, which can cause glenohumeral sprains that may increase joint laxity and decrease stiffness, leading to instability. | Nonoperative treatment (rest, activity modification, and NSAIDs) and PT. Surgery may be warranted after recurrent dislocations or first-time dislocation in young, active patients at high risk for recurrence. 161 | 3 wk 12 b to 6 mo 91 c |
| Subacromial impingement | Can result from the forces on the shoulder during weightbearing maneuvers. 4,60,113 Abnormal distribution of stress can compress the rotator cuff tendons, leading to chronic impingement syndrome with subacromial bursitis. | PT (with or without subacromial steroid injections) and NSAIDs, or surgery if unresponsive. 70%-90% of cases resolve with nonoperative treatment. 18,43 If untreated, subacromial impingement can lead to partial or complete tear of the rotator cuff. 146 | 4 wk 36 b to 6 mo 168 c |
| Distal radius epiphysiolysis (“gymnast’s wrist”) | Can result from repetitive compression loading and shearing forces on an extended wrist, such as when basing or performing handsprings or walkovers. Presents with physeal stress reactions on radiographic evaluation. 32,86 | Nonoperative treatment (rest, activity modification, and NSAIDs), period of immobilization, and then PT. Consider monitoring for growth disturbance. | 6-8 wk 72 |
| Wrist sprain or strain | Skills (eg, basing and tumbling) often require transmission of loads exceeding body weight through the wrist while dorsiflexed. Often presents with chronic, insidious pain. 32,33 | Nonoperative treatment (rest, activity modification, and NSAIDs). | Regain full ROM d |
| Back | |||
| Lower back strain | Repetitive hyperextension, flexion overload, forced rotation, and unbalanced shear forces from tumbling, jump landings, and stunts. Often presents with chronic, insidious pain. 11,44 | Nonoperative treatment (rest, activity modification, and NSAIDs) with or without lumbar bracing. 84 | Regain full ROM d |
| Pars interarticularis stress reaction (spondylolysis or spondylolisthesis) | Repetitive hyperextension, flexion overload, forced rotation, and unbalanced shear forces from tumbling, jump landings, and stunts can result in lumbar vertebral injury progressing from stress reaction to spondylolisthesis with time and continued high-impact activity. Poor technique can further contribute. 75,108 | Nonoperative treatment (rest, activity modification, and NSAIDs) and PT with or without antilordotic bracing. Rarely requires surgical pars repair or spinal arthrodesis, 48,109 because 92% of injuries respond well to nonoperative therapy. | 4 wk 98 b to 12 mo 52 c |
| Lower Extremity | |||
| Femoroacetabular instability or impingement | Can result from repetitive training and compensatory soft tissue laxity, likely caused by strategic landings after jumps and tumbling skills. The extremes of ROM can lead to labral damage and cause intra-articular impingement (at posterior-superior acetabulum) or extra-articular impingement (between AIIS and distal femoral neck). 19,140,164 | Nonoperative treatment (rest, activity modification, and NSAIDs) and PT. Symptomatic patients can be treated with labral repair, resection of arthroscopic cam deformity if present, and periacetabular osteotomy for symptoms associated with hip dysplasia. | 6 wk 171 b to 8 mo 41 c |
| ACL or PCL injury | Extensive training increases anterior knee laxity, leading to diminished postural stability and increased risk of ligament damage. 120 ACL injury most often occurs with twisting, valgus, and hyperextension or when landing skills are “short” or off-balance. 8,61 PCL injury can result from force applied to the lower leg while the knee is at a 90° angle, such as impact while basing. 77 | Surgical ACL reconstruction is favored for young athletes hoping to return to sport after injury. 88 PCL tears often can be treated nonoperatively. 65,112,130 | |
| Patellar tendonitis or Osgood-Schlatter disease | Repetitive high-impact movements, particularly jumping, can cause inflammation about the patellar tendon and tibial tubercle. 37,59,160 | Nonoperative treatment (rest, activity modification, and NSAIDs) and PT with or without bracing. Rarely requires surgical excision of symptomatic, unfused ossicle after skeletal maturity. 165 | 8-12 wk 124 |
| Patellofemoral syndrome | Pressure up to 7 times the body weight can be transmitted through the knee with squatting and other high-impact positions involved in stunts, tumbling, and jumps. Presents with anterior knee pain. 10 | Nonoperative treatment (rest, activity modification, and NSAIDs) and PT with or without bracing. 116 Surgery for select, recalcitrant cases if alignment issues are present. | 6-8 wk 56,71 |
| Talar osteochondral lesions | In addition to resulting from recurrent ankle sprains, these lesions also occur from short landings from underrotation while tumbling, in which the athlete impacts the floor with the ankle in hyperdorsiflexion. Lesions result from repetitive driving of the talus into the distal tibia. 110,159 | Nonoperative treatment (rest, activity modification, and NSAIDs) with or without CAM boot or crutches. Surgery should be considered if lesion is unstable. 59,107 | 5 wk to 6 mo 79,142 c |
| Ankle sprain or strain | Can be sustained from landing in an inverted or plantarflexed position, decreasing ability to absorb ground reaction forces on impact. Lateral ankle ligaments are most commonly affected. 29,136 | Nonoperative treatment (rest, activity modification, and NSAIDs) and PT with or without bracing. Surgery is an option for recurrent instability. | Regain full ROM, strength, and function d |
a ACL, anterior cruciate ligament; AIIS, anterior inferior iliac spine; CAM, controlled ankle movement; NSAIDs, nonsteroidal anti-inflammatory drugs; PCL, posterior cruciate ligament; PT, physical therapy; ROM, range of motion.
b Least conservative estimation of return-to-sport time with nonoperative treatment.
c Most conservative estimation of return-to-sport time with operative treatment.
d Return-to-sport time varies depending on severity of injury and specific component injured. Radiographs should be obtained to rule out fractures.