
Abstract
Background:
Recent studies have suggested increased rates of lower extremity (LE) musculoskeletal injury after a diagnosed concussion, although significant heterogeneity exists.
Purpose:
To examine the current body of research and determine whether there is an increased risk for LE musculoskeletal injury after a concussion and to identify populations at an increased risk.
Study Design:
Systematic review; Level of evidence, 3.
Methods:
A systematic review of current literature using MEDLINE and PubMed databases was performed. Keywords included concussion, athlete, lower extremity injury, and return to sport. Inclusion criteria required original research articles written in the English language examining the rate of LE injuries after a diagnosed concussion.
Results:
A total of 13 studies involving 4349 athletes (88.1% male and 11.9% female; mean age, 19.8 years) met inclusion criteria. Athletes were classified as high school (46.1%), collegiate (17.0%), or professional (36.9%). Of the 13 studies, 4 demonstrated an increased risk of LE injury within 90 days of a diagnosed concussion (odds ratio [OR], 3.44; 95% CI, 2.99-4.42), and 6 revealed an elevated risk of injury within 1 year of concussion (OR, 1.85; 95% CI, 1.73-2.84). Increased risk was seen in professional (OR, 2.49; 95% CI, 2.40-2.72) and collegiate (OR, 2.00; 95% CI, 1.96-2.16) athletes compared with high school athletes (OR, 0.97; 95% CI, 0.89-1.05). A stepwise increase in risk of sustaining an LE injury was observed with multiple concussions, with increasing risk observed from ≥2 (OR, 2.29; 95% CI, 1.85-2.83) to ≥3 (OR, 2.86; 95% CI, 2.36-3.48) career concussions.
Conclusion:
An increased incidence of LE injuries was observed at 90 days and 1 year after the diagnosis of a concussion. Higher levels of competition, such as at the collegiate and professional levels, resulted in an increased risk of sustaining a subsequent LE injury after a diagnosed concussion. These results suggest an at-risk population who may benefit from injury prevention methods after a concussion. Future studies should focus on identifying which injuries are most common, during what time period athletes are most vulnerable, and methods to prevent injury after return to sports.
The understanding of the short- and long-term consequences of concussions has significantly evolved in recent years. Concussions occur commonly in athletes of all skill levels at a rate of 0.17 to 0.99 per 1000 athlete-exposures, with increasing incidence over time. 32,44 The most common cause of a concussion is direct, player-to-player contact. 26 Despite how frequently these injuries occur, concussions remain poorly understood and difficult to diagnose, with up to 52.7% of sports-related concussions going unreported. 28 Although return-to-play protocols have been designed to mitigate subsequent injury, athletes experience an increased rate of musculoskeletal injury after a concussion. 3,18,36
Concussive episodes produce myriad symptoms, including headaches, gait imbalances, dizziness, difficulties concentrating, irritability, and confusion. 42 Multiple theories 2,38,39 have suggested that concussions share similar pathophysiology and biological factors with injuries such as altered cerebral blood flow, diffuse axonal injury, and neuroinflammation. The acute effects of concussions can be detrimental to athletic performance, with prior studies 8,17,27,35 demonstrating alterations in reaction time, gait patterns, and postural stability after returning to play. These alterations not only adversely affect performance but also make the athlete more vulnerable to subsequent injury.
Recent literature 1,9,40 illustrates that neuromuscular impairment increases the risk of lower extremity (LE) injury. The purpose of this systematic review was to assess whether there is an elevated risk of LE injury after a sports-related concussion and identify which athletes harbor the highest risk of subsequent injury. We hypothesized that there would be an increased risk of LE injury after concussion at all levels of competition.
Methods
Research Framework
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were applied upon the review and evaluation of literature for this study. 23
Search Strategy
A systematic review of the Cochrane Database of Systematic Reviews, the MEDLINE/PubMed Database (U.S. National Library of Medicine, National Institutes of Health), Embase, and Web of Science electronic databases was performed in October 2020. Results were limited to articles in English published between January 1, 2000, and September 30, 2020. Titles and keywords were utilized to screen literature for inclusion. The following search terms were constructed for the search: (concussion OR head injury) AND (return to sport OR athletes baseball OR basketball OR bicycling OR cricket sport OR golf OR boxing OR football OR hockey OR martial arts OR racquet sports OR soccer OR track and field OR volleyball OR weight lighting OR youth sports) AND (lower extremity injury OR groin injury OR hip injury OR buttocks injury OR thigh injury OR knee injury OR ankle injury). Reference lists from all primary articles were checked by 4 of the authors (T.R.J., J.P.C., P.J.B., and Y.H.) to further retrieve articles that may not have been found in the initial search. The search yielded 278 potential articles, of which 13 articles were included after application of selection criteria (Figure 1).

PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) 2009 flow diagram of study selection.
Data Extraction and Synthesis
Data extracted from each study included the number of athletes, age, sex, sport played, level of play, odds ratio (OR) of injury, and number of concussions per athlete. Articles were reviewed by all authors, and agreement was reached regarding the data extracted. Because of the heterogenicity of patient populations, differences in sport played, and reported outcomes including types of LE injury, a meta-analysis was not performed. The statistics were primarily descriptive, and each study was evaluated qualitatively. Three authors (P.J.B., M.J.A., and Y.H.) assessed the eligibility and quality of studies for reporting LE injuries after concussions. Outcome data were extracted from the reviewed papers. Selected studies were grouped into categories, allowing results to be compared across studies and data to be weighted and pooled. Validity assessment and data extraction were reviewed by 3 additional authors (T.R.J., J.P.C., and K.R.O.). All discrepancies were resolved by reviewing the original source papers; discussion culminated with consensus reached among all authors.
Risk of Bias
Because of the heterogenicity of studies included in this review, the Methodological Index for Non-Randomized Studies (MINORS) instrument was utilized to evaluate the quality of the literature. 41 The MINORS instrument is a validated tool designed to evaluate the methodological quality of nonrandomized controlled studies; it contains a 24-point scale for comparative studies and a 16-point scale for noncomparative studies. 41
Results
Study Selection and Study Bias
All 13 of the included studies were comparative studies, with a mean MINORS score of 19.8 of 24 (range, 19-21). Of the total included studies, 10 examined college athletes, ∥ 2 focused on professional athletes, 32,34 and 1 studied high school athletes. 25
Study Characteristics
The collection of studies included a total of 4349 participants. Only 9 of the 13 studies included participant genders, of which 2066 (88.1% of reported) were men and 278 (11.9% of reported) were women (Table 1). ¶ In terms of skill level, 1604 participants were professional, 741 collegiate, and 2004 high school athletes. A mean age of 19.8 (SD, 19.3-20.1) years was reported among only 5 studies that reported age (391 total athletes). 4,5,11,14,24 Nine studies focused on multiple sports, including contact and noncontact sports. ¶ Two studies examined American football exclusively, 21,34 1 focused only on NBA athletes, 32 and 1 study explored National Collegiate Athletic Association (NCAA) Division I athletes but did not specify sports included. 29
Study Characteristics a
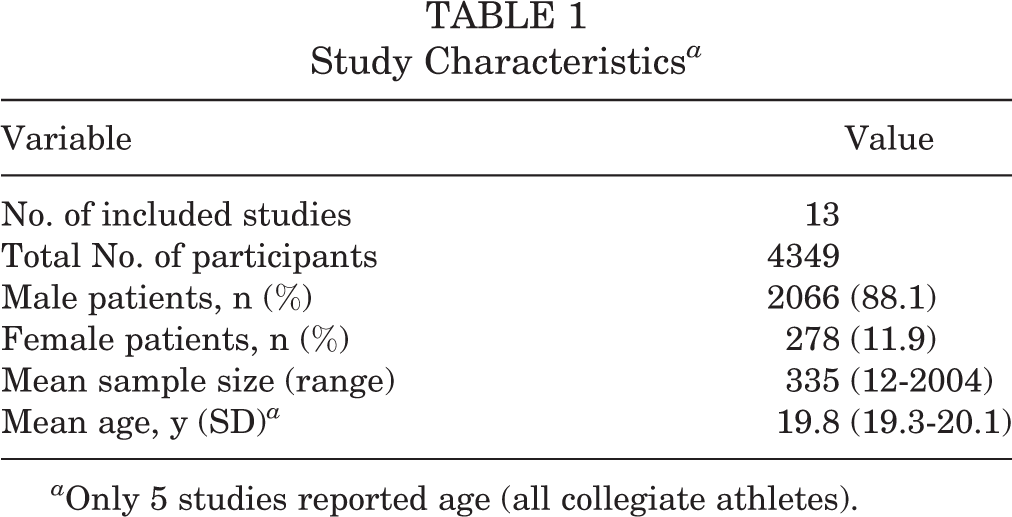
a Only 5 studies reported age (all collegiate athletes).
Relative Risk of LE Injury Within 90 Days of Return to Play After Concussion
Four studies 4,15,20,24 evaluated the 90-day window after return to play from a concussion and reported variable results. The OR in the 4 studies ranged from 1.47 to 4.69. The 3 studies examining collegiate athletics included a heterogenous grouping of sports, while the other study examined only professional athletes in the National Basketball Association (NBA). The pooled data from the 4 studies resulted in an elevated risk of LE injury (OR, 3.44; 95% CI, 2.99-4.42). The findings are summarized in Table 2.
Odds Ratio of Sustaining Lower Extremity Injury Within 90 Days After Concussion
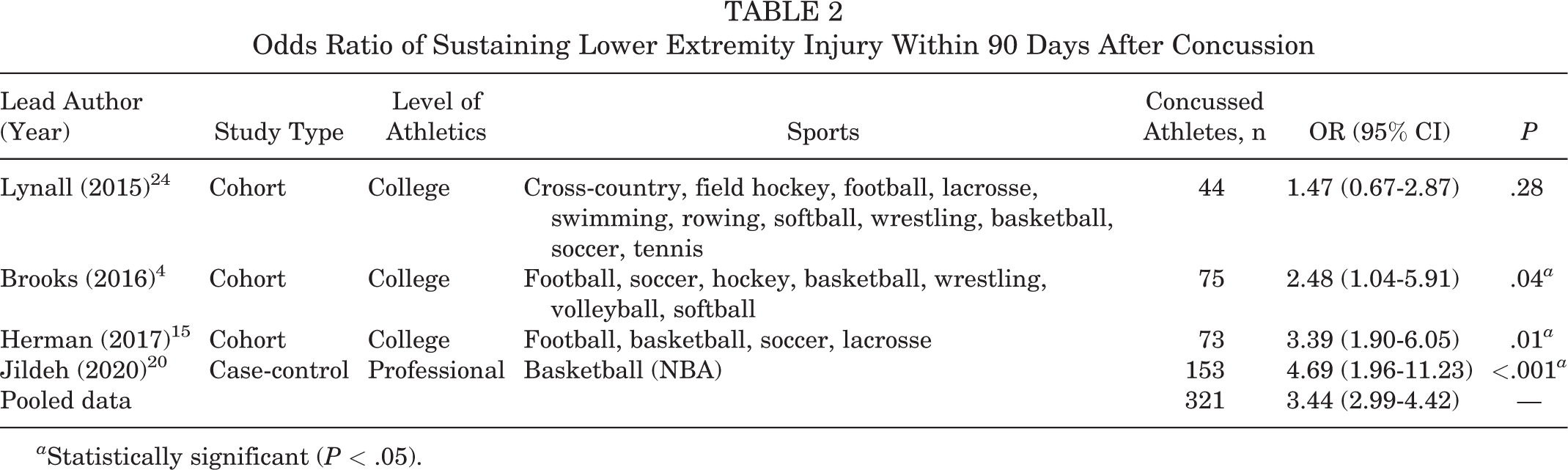
a Statistically significant (P < .05).
Relative Risk of LE Injury Within 1 Year of Concussion
Six studies 5,11,16,21,24,29 examined the odds of college athletes sustaining an LE injury 1 year after concussion compared with controls. The findings are summarized in Table 3. Collectively, athletes experienced a 1.85-fold increase (95% CI, 1.73-2.84) in LE injury within 1 year of a diagnosed concussion.
Odds Ratio of Sustaining Lower Extremity Injury Within 1 Year After Concussion a

a Retrosp, retrospective.
b Statistically significant (P < .05).
Risk of LE Injury After Concussion Stratified by Sex
While 9 studies collected data on male and female athletes, ¶ only 2 studies 15,16 performed an analysis comparing the associated risk between male and female athletes (Table 4). Pooled data for men resulted in an OR of 2.81 (95% CI, 2.12-3.79), while the data for women yielded an OR of 2.32 (95% CI, 1.81-3.31). Both sexes had an elevated risk of LE injury in 1 of the 2 studies. There were no discernable differences between male and female athletes regarding risk of LE injury after a concussion.
Odds Ratio Comparing Sex to Impact of Concussion on Lower Extremity Injury a

a CON, concussion.
b Statistically significant (P < .05).
Level of Competition, Concussions, and LE Injuries
There was a significant heterogeneity in the age and level of competition among studies reporting on LE injury after concussion. The high school study did not demonstrate an increased risk of LE injury after return to sports (RTS) after a concussion; however, this was the only article to make a distinction between time-loss injuries and non–time-loss injuries. The authors defined a time-loss injury as any injury evaluated or treated by an athletic trainer or physician that resulted in restriction from participation beyond the day of injury. 25 When accounting for the severity of LE injury, the authors reported a significantly increased incidence of time-loss LE injuries after a concussion in high school athletes compared with nonconcussed controls (OR, 1.34; 95% CI, 1.13-1.60; Wald test χ2 = 0.58). Pooled data from studies on both collegiate- and professional-level athletes demonstrated an increased risk of LE injury after returning from a concussion. A comparison of pooled data stratified by level of competition is displayed in Table 5.
Comparing Lower Extremity Injury Risk After Concussion by Level of Competition

Multiple Concussions and LE Injuries
Several studies explored the effect of multiple concussions on LE injuries. Pietrosimone et al 34 examined the relationship of the number of concussions sustained in the National Football League (NFL) and subsequent LE injuries throughout the player’s NFL career. Of the players who filled out the survey, 60.8% (1477/2429) players sustained at least 1 concussion. The authors reported that among NFL athletes who sustained 1 concussion in their career, there was a 1.59-fold increased risk of LE injury as compared with nonconcussed controls (OR, 1.59; 95% CI, 1.30-1.94). A stepwise increase in risk of sustaining an LE injury was observed with ≥2 (OR, 2.29; 95% CI, 1.85-2.83) and ≥3 (OR, 2.86; 95% CI, 2.36-3.48) career concussions.
Additionally, Harda et al 14 investigated the relationship of multiple concussions and LE injury in a cohort of 144 male collegiate athletes. Among participants who experienced multiple concussions, a significantly higher risk of LE injury was observed compared with a nonconcussed group (n = 48; OR, 1.66; 95% CI, 1.07-2.56; P = .02) and with those with a single concussion (n = 48; OR, 3.00; 95% CI, 1.26-7.12; P = .01). However, the authors found no significant risk of LE injury between 1 concussion and no concussions (n = 48; OR, 0.92; 95% CI, 0.41-2.05; P = .84).
Discussion
The present study demonstrates that athletes returning to play from a concussion harbor an elevated risk of LE injuries within 90 days and 1 year of concussion. As the level of competition increased, there was a concurrent increase in the likelihood of sustaining an LE injury. Additionally, when evaluating the impact of multiple concussions, a greater number of concussions were found to correlate with an increasing risk of LE injury. Finally, both men and women were shown to be vulnerable to LE injury. However, minimal data exist comparing men and women. Overall, despite the implementation of return-to-play protocols after concussion, the current literature reports an increased risk of LE injuries for collegiate and professional athletes in both the short- and long-term periods.
Traditionally, return-to-play protocols after concussion focused on neuroprotective measures. 13 In more recent years, research has revealed a more global impact of brain injury, including effects on LE and proprioceptive factors, resulting in greater focus on kinematic metrics. 7,22 In the present systematic review, we found an increased risk of subsequent LE injury at both 90 days (OR, 3.44; 95% CI, 2.99-4.42) and 1 year (OR, 1.85; 95% CI, 1.73-2.84) after the initial diagnosis of a concussion. Dubose et al 7 studied 39 Division I collegiate football players using motion-capture systems and force plates to compare joint stiffness before and after the season. Thirteen of the 39 players sustained a concussion during the season at an average of 49.9 days before the postseason testing. Comparing post- to preseason testing, the concussed group demonstrated increased hip stiffness, decreased knee and leg stiffness, and no change in ankle stiffness, suggesting altered joint properties after concussion. Lapointe et al 22 kinematically evaluated jump cuts between 10 previously concussed athletes and 10 matched nonconcussed controls. The concussed group exhibited significant alterations in the vertical center of mass during the act of jump cutting: decreased knee external rotation and flexion for both left and right cutting movements. Collectively, these studies suggest that joint kinematics may be altered after sustaining a concussion, which may explain the increased incidence of LE injury observed in our study. The included studies in our analysis, however, did not examine these kinematic properties. Further studies are warranted to clinically correlate and identify which kinematic alterations create the highest risk for LE injury. Ultimately, return-to-play protocols that incorporate joint kinematic analysis may be developed to identify athletes who may require additional rehabilitation before safely returning to competition.
Recent studies 6,10,20,30,31 have demonstrated that both age and competition level affect time to RTS, as younger athletes require more time to recover from a concussion compared with older, higher-level athletes. The delayed RTS in high school athletes is likely multifactorial. The developing brain may require more time to recover; thus, RTS protocols tend to be more conservative to protect adolescents. However, as the level of competition increases to the professional level, additional internal and external pressures to return to play exist with financial incentives, team roster management, and postseason pursuits. A study examining 127 American collegiate athletes who sustained a concussion reported an RTS of 12.9 days (interquartile range, 9.7-20.7 days), 33 while 124 European professional soccer players revealed an even faster average RTS of 10.9 days (95% CI, 2-28 days). 37 These timelines are less than half the 30.4 ± 23.2 days reported for RTS by Jildeh et al 20 in their evaluation of 357 concussed high school athletes. The decreased time to RTS from a concussion in college and professional athletes may not be enough time to adequately rehabilitate and return safely, as demonstrated by the increasing rates of LE injury in these groups; additionally, even the increased time in RTS for high school athletes may not fully protect the athletes from a subsequent LE injury. Furthermore, there are more physical demands at the collegiate and professional levels, which may portend a higher risk of LE injury, as demonstrated in the present study.
The current literature demonstrates mixed results regarding the effect of sex on LE injury risk after concussion. In a systematic review evaluating factors that predict recovery from a concussion, Iverson et al 19 identified 17 studies reporting that female sex predicted a longer recovery time compared with male sex, but also described 27 studies suggesting that sex played no significant predictive value in recovery time. The present systematic review showed conflicting results from the 2 studies examining sex and concussions. Herman et al 15 demonstrated that men had a higher risk of LE injury after concussion compared with women (OR, 3.72; 95% CI, 1.84-7.54 vs OR, 2.75; 95% CI, 0.98-7.69, respectively). Conversely, Houston et al 16 described men who sustained a concussion as having a lower rate of subsequent ankle (OR, 1.41; 95% CI, 0.68-2.91 vs OR, 2.54; 95% CI, 1.88-7.54) and knee (OR, 1.59; 95% CI, 0.74-3.41 vs OR, 1.88; 95% CI, 1.10-3.19) injuries compared with women. In an effort to evaluate the relationship between sex and concussions, Tanveer et al 43 prospectively compared 695 men and 362 women who sustained a concussion. They found differences in cognitive and symptom scores between men and women older than 13 years. However, when they only compared patients younger than 13 years, there were no sex-based differences in concussion symptoms or cognitive scores. The authors suggest that systemic hormonal changes during and after puberty may affect recovery from concussions. Only 11.9% of the athletes in our systematic review were female, which suggests that women were understudied and that the majority of studies focused on male-dominated sports, such as football and basketball. With the current body of literature demonstrating conflicting results, future investigations examining female athletes are required to elucidate the role of sex in recovery from concussions.
Limitations
There are several limitations to this study. First, the reporting was not standardized across studies, and many relied on self-reporting, which may introduce selection and recall biases. Many of these studies included a wide variety of sports. This heterogeneity introduces significant variability in diagnostic protocols and symptom reporting across sports, so certain populations may be underrepresented from underreporting. While collegiate and professional sports mandate the reporting of concussions by teams, high school sports have significant variability in these requirements. Similarly, there is a lack of information regarding the process of medical clearance and which return-to-play protocols were utilized, thus limiting the generalizability of these results. Finally, one important consideration is that the majority of studies report significant results demonstrating increased LE injuries. While this suggests a correlation, it is possible that publication bias exists and may skew these results. There is also limited reporting in these studies of types of LE injuries sustained. Further longitudinal studies with larger sample sizes, more standardized diagnosis, and return-to-play protocols are required to identify those at risk for LE injury, which injury types are more likely in each sport, and the optimal timing to RTS.
Conclusion
An increased incidence of LE injuries was observed at 90 days and 1 year after the diagnosis of a concussion. Higher levels of competition, such as at the collegiate and professional levels, resulted in an increased risk of sustaining a subsequent LE injury after a diagnosed concussion. These results suggest an at-risk population who may benefit from injury prevention methods after a concussion. Future studies should focus on identifying which injuries are most common, during what time period athletes are most vulnerable, and methods to prevent injury after RTS.
Footnotes
Final revision submitted August 16, 2021; accepted August 25, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: T.R.J. has received education payments from Medical Device Business Services and Pinnacle and hospitality payments from Exactech and Zimmer Biomet. P.J.B. has received grant support from Arthrex and education payments from SeaPearl and Smith & Nephew. K.R.O. has received grant support from Arthrex; education payments from Arthrex, Medwest, and Smith & Nephew; consulting fees from Endo Pharmaceuticals and Smith & Nephew; nonconsulting fees from Arthrex; and hospitality payments from Stryker, Wright Medical, and Zimmer Biomet. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.