
Abstract
Background:
Chronic tendon retraction subsequent to distal biceps tendon rupture significantly increases repair difficulty and potential for tendon grafting. Biceps tendons that appear short or absent with magnetic resonance imaging (MRI) or that cannot be readily identified at surgery may erroneously be classified as irreparable. These apparent “absent” biceps tendons may actually be retracted and curled up inside the muscle, visually resembling the head-neck of a turtle retracted inside its shell (the “turtle neck sign”). When located, these tendons could be unfolded and repaired primarily. This type of tendon retraction seems to be associated with high-degree ruptures and larcertus fibrosus tears.
Purpose:
To test the hypothesis that tendon retractions with a turtle neck sign on MRI are more associated with high-degree ruptures and larcertus fibrosus tears versus tendon tears with simple linear retraction.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
Retracted distal biceps tendon ruptures on sagittal MRI were categorized as linear retraction or curled-up (turtle neck) retraction. Retraction length, injury severity, and lacertus fibrosus tears were analyzed.
Results:
The authors retrospectively analyzed the patient records of 85 consecutive traumatic distal biceps tendon ruptures from 2003 to 2019; the final study cohort was 37 patients. Injury-to-surgery timing was as follows: <3 weeks, 43% (16 cases); 3 weeks to 3 months, 32% (12 cases); and >3 months, 24% (9 cases). Overall, 19 patients had linear retraction <7 cm (mean, 3.3 ± 1.9 cm) and 18 patients had a turtle neck retraction ≥7 cm (mean, 9.1 ± 1.6 cm). The injury-to-surgery time (median [± interquartile range]) was 27 days (±90 days) in the linear retraction group and 23 days (±65 days) in the turtle neck retraction group. The turtle neck retraction group had a significantly higher occurrence of abnormal hook test findings, complete distal biceps tendon rupture, and lacertus fibrosus tears compared with the linear retraction group (100% vs 58%, 100% vs 68%, and 100% vs 37%, respectively; P ≤ .02). However, significant repairability differences were not found.
Conclusion:
Highly retracted distal biceps turtle neck sign tendon ruptures occur frequently in association with high-degree ruptures and lacertus fibrosus tears. The presence of a turtle neck retraction did not affect reparability. Surgeons should be aware of this curled-up retraction to avoid mistaking it for an absent tendon or a muscle-tendon disruption.
Keywords
Distal biceps tendon ruptures are uncommon injuries with an incidence rate of 1.2 to 2.6 per 100,000 patients. 16,27 Unfortunately, diagnosis of a distal biceps tendon rupture is sometimes unclear and in many cases delayed. 1,3 Furthermore, many studies 14,18,25 have shown an increasing risk of surgical complications as a result of delay in diagnosis. Magnetic resonance imaging (MRI) findings can be confusing, even though MRI is the gold standard for imaging complete or partial tears. 8,17 Detailed information of the biceps tendon injury status would help surgeons with their preoperative treatment plan, including repair or reconstruction of the tendon.
Reconstruction of chronic distal tendon ruptures is technically difficult. 7 Where the tendons appear to be “resorbed,” surgeons may choose reconstruction or augmentation rather than the release of adhesion and direct repair because of the impression that the latter option is not possible. Retraction of the muscle-tendon junction proximally makes the repair demanding because of the gap between the tendon and bone attachment, which in many cases needs some type of augmentation. 28,30,31 Other risk factors making this surgery even more challenging include fibrosis and/or atrophy of the muscle, and a ruptured bicipital aponeurosis.
The senior authors (S.W.O. and J.S.) noticed when using ultrasonography that some avulsed biceps tendons appeared to be folded on themselves inside the muscle, similar to a turtle's neck when it retracts its head into its shell. As such, this has come to be known in our practice as the “turtle neck sign.” Based on these sonographic findings, the senior authors have also been able to observe similar findings on the MRI scans of several patients with retracted biceps tendons (Figure 1). Surgical exploration has confirmed that the curled-up tendon can be freed from the surrounded scar tissue by careful dissection then repaired primarily.
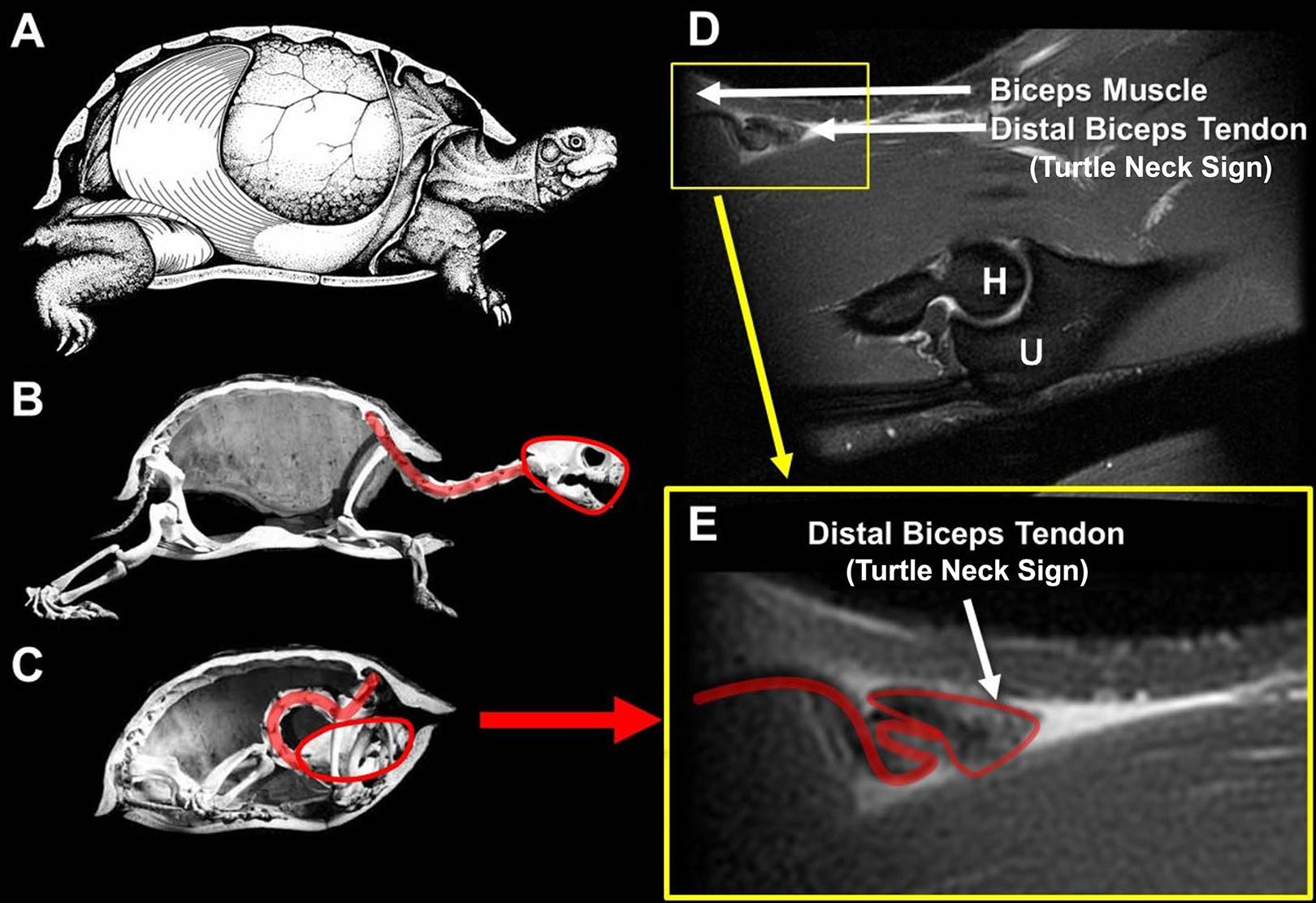
(A) Lateral view of the Terrapene carolina (common box turtle); half the shell has been removed to reveal the internal morphological relationships between the lungs, abdominal muscles, and skeletal elements. (B) The skeleton with the neck fully extended, similar to an intact distal biceps tendon. (C) The turtle head is retracted fully into the shell and the neck is curled up. (D) A sagittal T2-weighted fat-suppressed magnetic resonance imaging scan shows a ruptured distal biceps tendon curled up on itself and mimicking a retracted turtle neck, which we call a “turtle neck sign.” (E) Close-up view of the turtle neck sign. H, humerus; U, ulna. (Sources: Images A-C adapted with permission from Landberg T, Mailhot JD, Brainerd EL. Lung ventilation during treadmill locomotion in a terrestrial turtle, Terrapene carolina. Journal of Experimental Biology. 2003;206:3391-3404. Images D and E from Mayo Foundation for Education and Research, reproduced with permission. All rights reserved.)
Based on our interoperative observations, we hypothesized that the curled-up tendons on MRI scans were more associated with high-degree ruptures and larcertus fibrosus tears as compared with tendon tears with simple linear retraction. The purpose of this study was to test this hypothesis.
Methods
Inclusion and Exclusion Criteria
After receiving institutional review board approval, we performed a retrospective medical-record and imaging review on all patients who had undergone distal biceps repair or reconstruction by one of the senior authors (S.W.O.) between August 2003 and January 2019. To be included, each patient had to meet the following criteria: (1) preoperative data were available, including the timing of injuries and hook test 23 –25 results; (2) preoperative sagittal views of the MRI scans were available with the elbow extended in the anatomic position; and (3) intraoperative information regarding the distal biceps tendon and lacertus fibrosus status was available. Of the 85 patients (90 cases) of distal biceps tendon repair performed during that period, 23 patients (27 cases) were excluded owing to insufficient clinical documentation. Twenty-one patients (22 cases) were excluded because of an unavailable or inadequate MRI (eg, number of slices were limited in the area of interest, slice thickness, resolution, metal artifact, interference). Four patients (4 cases) were excluded because of the lack of detailed intraoperative information, including whether the ruptures were related to infection or tumors (Figure 2).

Flow diagram showing the process for patient inclusion and analysis in the study. MRI, magnetic resonance imaging.
Basic MRI Parameters
MRI was performed at a single institution using 1.5-T machines with proton-density, T1, and T2 sequences in 3 planes (axial, coronal, and sagittal). The position in the sagittal image must have been in an anatomic position for the patient to be included in the study.
Evaluation of Ruptured Distal Biceps Tendon
An independent reviewer (M.H.) who was not involved in the patients’ care reviewed the records and operative notes for documentation of causes of injuries, the timing of injuries, the hook test results, lacertus fibrosus status, intraoperative observations, and type of surgical procedure. As there is no definite agreement on what defines the acuity of an injury (estimates range from 3 weeks to 3 months), 6 we defined acute, subacute, and chronic rupture as injury-to-surgery times of <3 weeks, 3 weeks to 3 months, and >3 months, respectively.
Retraction of the distal biceps tendon on the MRI was measured by 2 orthopaedic surgeons (A.B. and T.R.). For radiographic evaluation, scrolling of the sagittal fluid-sensitive sequence, proton-density sequence, or T2 sequence was performed to identify the most distal portion of the stump and the most posterior cortex of the radial tuberosity. The distance of retraction was measured from the most distal portion of the stump to the center of the most posterior cortex at the radial tuberosity on the sagittal view. If these 2 structures were not on the same image, the cursor had to be held at the most distal stump, and the observer would scroll to the image with radial tuberosity to measure the distance. Retraction was measured twice by each orthopaedic surgeon, 8 weeks apart, to evaluate intraobserver reliability. Retraction on the sagittal MRI view was categorized into 2 groups based on the configuration of the retracted tendon: (1) linear retraction group (Figure 3) or (2) curled-up (turtle neck) retraction group (Figures 1 and 4; also see Video Supplement). To better show the anatomic relationship of the retracted distal biceps tendon to surrounding structures, a schematic illustration was derived using 3-dimensional manual contour segmentation on a representative sagittal T2-weighted fat-suppressed MRI scan on RIL-Contour and ITK-SNAP software 32 (Figure 5).
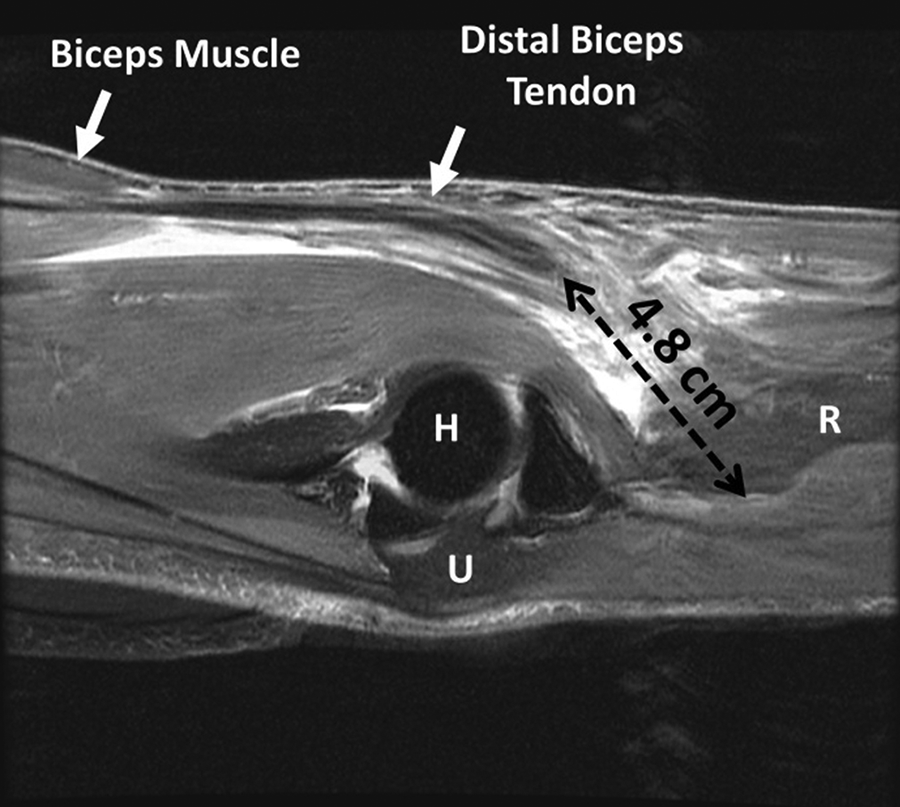
An overlay image of a sagittal T2-weighted fat-suppressed magnetic resonance imaging scan shows linear retraction of the ruptured distal biceps tendon. H, humerus; R, radius; U, ulna.
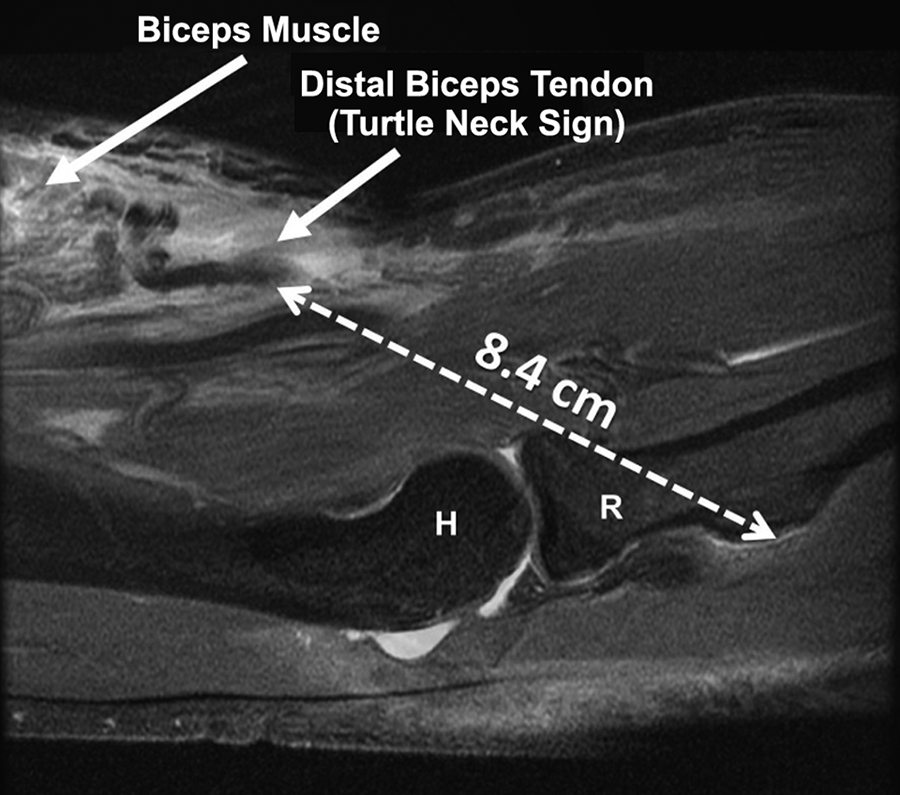
Overlay image of a sagittal T2-weighted fat-suppressed magnetic resonance imaging scan shows the curled-up, ruptured distal biceps tendon with the turtle neck sign. H, humerus; R, radius.
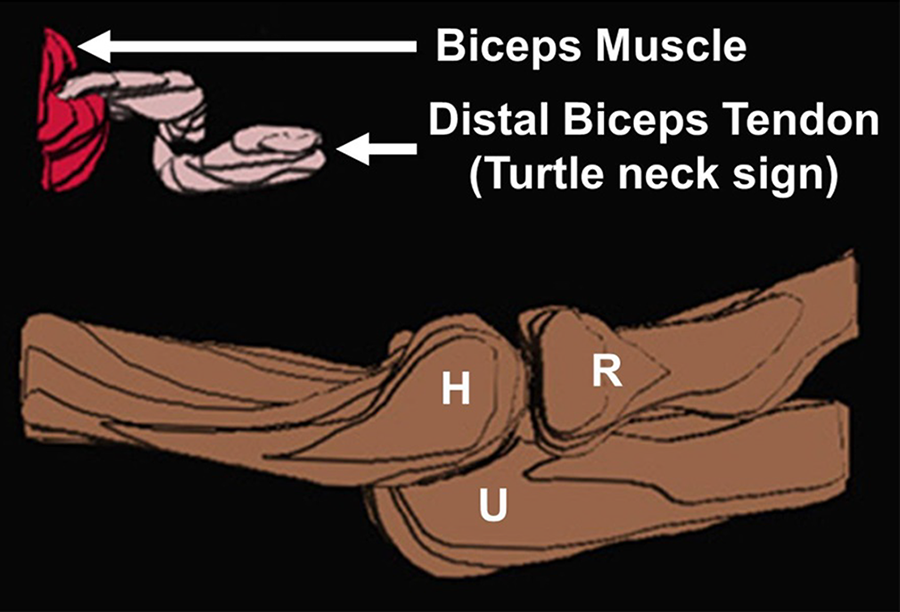
Schematic illustration demonstrating turtle neck retraction of the distal biceps tendon. Illustration was derived using 3-dimensional manual contour segmentation on each slice from a representative sagittal T2-weighted fat-suppressed magnetic resonance imaging scan (the same series from which panels D and E in Figure 1 were obtained) on RIL-Contour and ITK-SNAP software. 32 Selective segmentation of the distal biceps tendon, biceps muscle, distal humerus, and proximal radioulnar joint was performed to show the relative anatomic position of the retracted distal biceps tendon. H, humerus; R, radius; U, ulna.
Statistical Analysis
Statistical analyses were performed using statistical software JMP Pro version 10.0.0 (SAS Institute). Nonparametric data were reported as median ± interquartile range (IQR). Data were modeled using analysis of variance. The number of patients in each group was tabulated and analyzed with the Fisher exact test. A P value <.05 was considered to be statistically significant. Intraclass correlation coefficients (ICCs) were used for the analysis of measurement reliability. The ICC estimates and their 95% confidence intervals were based on a mean-rating (k = 2), consistency, or 2-way random-effects model. 11,12,29 An ICC >0.85 was considered to represent excellent reliability. 9 Intra- and interobserver reliability was determined based on the observers’ measuring of retraction of the distal biceps tendon.
Results
A total of 37 cases in 37 patients (36 male and 1 female patients) were included in the study. The average patient age was 51 ± 11 years. Injury acuity before surgery was as follows: acute rupture, 43% (16 cases); subacute rupture, 32% (12 cases); and chronic rupture 24% (9 cases). Nineteen patients had linear retraction in the sagittal view of the MRI, and all of these patients had retraction <7 cm. Eighteen patients had a turtle neck sign, and all patients had retraction >7 cm. The mean retraction in the turtle neck retraction group was significantly higher than that in the linear retraction group (9.1 ± 1.6 vs 3.3 ± 1.9 cm, respectively; P < .00001).
Preoperatively, the hook test 24,25 revealed an absent biceps tendon in 18 of 18 (100%) of the patients in the turtle neck retraction group versus 11 of 19 (58%) in the linear retraction group (P < .01). All of the patients in the turtle neck retraction group had a complete tear of the distal biceps tendon and a ruptured lacertus fibrosus, which was significantly greater in number than those observed in the linear retraction group (P = .02 and P < .00001, respectively) (Table 1).
Comparison of Preoperative and Intraoperative Characteristics Between Groups a
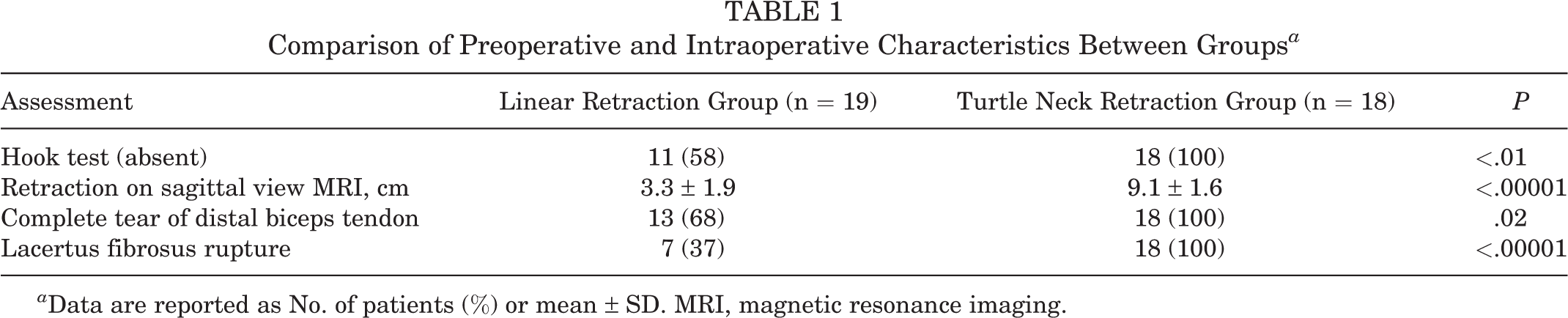
a Data are reported as No. of patients (%) or mean ± SD. MRI, magnetic resonance imaging.
Of the 18 patients in the turtle neck retraction group, 15 had repair of distal biceps tendon and 3 had reconstructions with Achilles allografts. One reconstruction was performed before we realized this pattern of folding of the tendon on itself within the muscle, and therefore it is not possible to know for certain whether it may indeed have been repairable or not. Two of these allograft reconstructions were revisions of failed prior repairs. Of the 19 patients in the linear retraction group, 2 had reconstruction and 17 had repair of the distal biceps tendon. Of the 2 patients who had reconstructions, one patient had surgery using Achilles tendon graft and the other patient had augmentation with the lacertus fibrosus. There was no significant difference between the 2 groups regarding those cases requiring reconstruction versus repair (P = .66).
Time from injury to surgery in the linear retraction group was not significantly higher than in the turtle neck retraction group (median ± IQR, 27 ± 90 vs 23 ± 65 days, respectively; P = .3). The intra- and interobserver reliability of measurement of retraction in the sagittal view demonstrated excellent reliability and is shown in Table 2.
Intra- and Interobserver Reliability for Retraction Measurements a
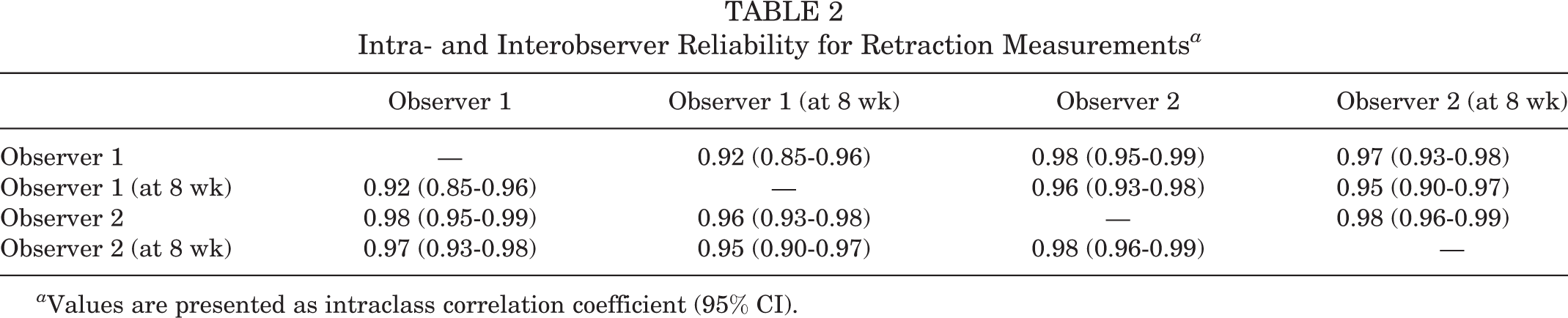
a Values are presented as intraclass correlation coefficient (95% CI).
Discussion
The present study showed that curled-up retraction of the tendon on MRI scans had a significantly higher association with high-degree rupture and larcertus fibrosus tear as compared with tendon tears with simple linear retraction. This study also showed that a highly retracted distal biceps tendon could be reliably assessed on an MRI, particularly in the sagittal view. We propose the term “turtle neck sign” to indicate such severely retracted tendons. When assessed on MRI, the turtle neck sign looks like a turtle head and neck that have been retracted into the shell. When a severely retracted tendon elicits the turtle neck sign, the tendon is curled up and surrounded by scar tissue, which after dissection can be freely pulled out of the wound and regain most, if not all, of its primary length. This can be seen in the supplemental intraoperative video and in Figure 1. On clinical examination, all patients with the turtle neck sign also had an absent hook sign. These observations have led us to believe that some of the injury patterns that were previously considered as an indication for reconstruction of distal biceps may be eligible for routine repair. 7,15
This finding is novel because understanding of the turtle neck sign has the potential to change preoperative planning, intraoperative findings, and postoperative outcomes. Distal biceps tendon ruptures lead to substantial functional deficits. 20 Some studies 10,22 have shown that an untreated distal biceps tendon tear leads to an average loss of 40% of supination and reduced muscle strength. An early diagnosis followed by prompt surgical treatment has been reported in many studies to lead to the best postoperative outcomes. 1,2,5,14,18,25 Additionally, delayed primary repair carries a higher risk of complications. 4,14,30
Many distal biceps tendon reconstructions previously considered to require graft augmentation might actually be repairable if the tendon can be uncurled and brought out to length. Hamer and Caputo 13 showed that when tendon retraction is prevented by an intact lacertus fibrosus, a late direct repair is possible. In a study of 10 patients with distal biceps tendon tears, Le Huec et al 17 showed that proximal tendon retraction <8 cm was associated with an intact lacertus fibrosus, whereas a retraction >8 cm indicated a torn lacertus fibrosus. Similarly to the work of Miller and Adler, 19 our study differed from that of La Huec et al 17 because 2 of our patients had a retraction <8 cm on sonography and MRI but had a torn lacertus fibrosus confirmed intraoperatively. This finding suggests that retraction <8 cm does not rule out possible rupture of lacertus fibrosus. Clinicians should pay attention to clinical examination of lacertus fibrosus because, in our experience, there have been cases of ruptured lacertus fibrosus with retraction <1 cm.
Morrey et al 21 showed that primary distal biceps tendon repairs can have excellent outcomes with a low rate of complications when performed in 60° to 90° of flexion. They also showed that reconstruction surgery should be considered based on the tendon quality rather than the amount of biceps retraction. The decision to reconstruct with a graft is often dependent on the elapsed time since the injury, clinical examination assessing the amount of retraction, and additional imaging. Robertson et al 26 showed that harvesting an autograft may cause donor site morbidity, extend surgery time to harvest, and require an additional surgical approach that includes the lower extremity. On the other hand, the use of an allograft increases procedural cost and carries a risk, albeit low, of disease transmission.
The turtle neck sign presents both orthopaedic surgeons and radiologists with an easily understandable mental image of a previously unreported finding on MRI. The main insight came when the distal biceps tendon was noted on ultrasonography imaging to be folded on itself in a manner similar to how a turtle’s neck curls up when it retracts its head into its shell. However, the surgeon must be aware of this possibility before surgical exploration of the tendon, which may appear to have been replaced by, rather than encased in, scar tissue. We believe that this finding will help orthopaedic surgeons to better understand the pathology of distal biceps tendon ruptures and to be able to repair what were previously thought to be unrepairable cases. In our study, we also found excellent intra- and interobserver reliability among distal biceps tendon retraction measurements. This finding suggests that the turtle neck sign can be reliably measured in MRI, particularly in the sagittal view.
Sometimes the biceps tendon appears deficient (short or absent) on MRI studies or cannot be readily identified at surgery. In such cases, it may be erroneously interpreted to have been disrupted at the muscle-tendon junction or resorbed and not able to be repaired. In our clinical practice, however, we have found that these apparent myotendinous disruptions and “absent” biceps tendons have turned out to have retracted and curled up inside the muscle. Furthermore, we have found that with meticulous surgical release and repair, tendon grafting reconstructions can be avoided.
This study has several limitations. Because of the retrospective nature of the study, we were limited only to existing MRI scans and clinical information already in the medical records. Additionally, the distal biceps procedures and clinical examination were done by a single surgeon.
Conclusion
The presence of a turtle neck sign on MRI of a severely retracted distal biceps tendon (usually in the sagittal view), indicates that the tendon is simply folded upon itself and encased in, rather than replaced by, scar tissue. The tendon is therefore likely to be able to be unfolded and repaired primarily, rather than having to be grafted. Surgeons treating this condition should be aware of this finding. This finding also permits radiologists to distinguish a distal avulsion from a muscle-tendon rupture.
Footnotes
Acknowledgment
A Video Supplement for this article is available at http://journals.sagepub.com/doi/suppl/10.1177/23259671211065030.
Final revision submitted August 11, 2021; accepted September 20, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: S.W.O. and the Mayo Clinic receive royalties from Acumed, Wright Medical, and DonJoy, and S.W.O. has received speaking fees from SIGN Fracture Care International. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Mayo Clinic (ref. IRB# 11-002988).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.