
Abstract
Background
Acute distal biceps tendon ruptures result in weakness and deformity. While in other jurisdictions the rate of surgical repair has outpaced rises in incidence, UK practice for distal biceps tendon ruptures is unknown. The aim of this survey was to characterise current UK clinical practice.
Methods
An online survey was sent to the surgeon members of the British Elbow and Shoulder Society. Questions covered respondent demographics, clinical decision making, surgical experience and willingness to be involved in future research.
Results
A total of 242 surgeons responded; 99% undertook acute distal biceps tendon repairs with 83% repairing at least half of all distal biceps tendon ruptures, and 84% of surgeons would have their own, hypothetical, acute distal biceps tendon rupture repaired in their dominant arm and 67% for their non-dominant arm. Patient age, occupation and restoration of strength were the commonest factors underpinning a recommendation of surgical fixation. Most surgeons (87%) supported a national trial to study operative and non-operative treatments.
Conclusions
UK upper limb surgeons currently advise surgical repair of acute distal biceps tendon ruptures for the majority of their patients. This is despite a paucity of evidence to support improved outcomes following surgical, rather than non-operative, management. There is a clear need for robust clinical evaluation in this area.
Background
Acute distal biceps tendon (DBT) ruptures can be a debilitating injury causing pain, weakness and an altered biceps contour. 1 Historically, they have been considered to be a relatively uncommon injury occurring in the dominant arm of otherwise healthy middle-aged men. 2 However, with increasing sporting participation and more active elderly populations, the incidence and age at presentation are expected to rise. Indeed, between 2001 and 2016, the incidence of DBT ruptures rose 6-fold among Swedish men. 3 Despite a lack of clinical consensus on the role of operative treatment, rates of surgical repair rose 28-fold in the same cohort. 3 Support for surgical repair has largely been driven by biomechanical studies that report a reduction in supination and elbow flexion strength, as well as impaired endurance in injuries managed non-operatively.4,5 Currently available studies investigating patient reported outcomes are noted to be at risk of selection bias and potentially conflicted. 6 Proponents of non-operative treatment cite concerns over serious operative complications, including nerve injury, radial neck fracture and heterotopic ossification (HO), and question the functional deficit conveyed by the biomechanical weakness identified on testing. 7
In the UK, it is unclear what the current practice is regarding acute distal biceps ruptures. The aim of this survey was to identify current UK clinical practice, gather information on the factors that influence surgeon treatment choice and to ascertain the degree of support amongst shoulder and elbow surgeons for future research into the treatment of acute DBT ruptures.
Methods
Administration of survey
Surgical members of the British Elbow and Shoulder Society (BESS) were invited via email to participate in an online survey prepared using the Bristol Online Survey system. Information about the aims of the survey and a hyperlink to the survey was provided. The survey was designed to take approximately 10 min to complete. There was no minimum number of responses required, as the study was opportunistic in terms of sample size and not driven by statistical testing. The response rate was defined as the number of responding participants divided by the number of eligible people invited. The statistical analysis was descriptive only. Responses were summarised quantitatively or narratively, as appropriate (using Microsoft Excel (Version 16.12) and Prism (Version 7.0)). No attempt was made to validate individual responses.
The email invitation was sent out on 17 June 2020, a further reminder email sent on 19 August 2020 and the survey closed on 31 October 2020. This was a voluntary survey of health care professionals and therefore formal ethical review was not sought. However, the survey was approved by the BESS Research Committee. A formal consenting process was not undertaken, rather completion of the survey was taken as implied consent. All responses were anonymous.
Survey contents
To assess respondent demographics, we asked about participant grade, place of work and age. To determine the degree of exposure to acute DBT repairs, we asked respondents to provide the total number of repairs performed annually and to estimate the percentage of acute DBT tears they typically repaired. For surgeons who did not perform repairs, the factors underlying this were explored.
The next section sought to investigate the pre-operative work-up of patients with acute DBT tears. Respondents were asked about investigations routinely used in diagnosis, decision making with regard to musculotendinous tears and whether decision making patient information leaflets were available. Surgeons were then asked about preferred surgical technique for repairs – the type of incision used and the type of bone–tendon fixation method.
To address the controversies surrounding patient selection for acute DBT repair, we asked respondents to rank the three most important factors leading to a recommendation for surgery or non-surgical treatment. In a hypothetical scenario, we asked if the responding surgeon would have their own acute DBT rupture surgically repaired in their dominant and non-dominant arm.
To investigate differences in post-operative rehabilitation, we asked whether chemical prophylaxis to prevent HO was routinely prescribed, whether a cast/splint/brace was utilised and for what duration, and if arm strength was routinely measured after rehabilitation.
Finally, respondents were then asked to consider the utility of future research into the treatment of acute DBT ruptures, including whether a national trial investigating operative vs. non-operative treatments would be useful, what their preferred study design would be and whether a nationally produced patient information resource would be valuable.
Within our collaborative, we piloted our survey on four members of the shoulder and elbow surgical community who perform acute DBT repairs.
A copy of the survey can be found in the online supplementary information (supplementary file 1).
Results
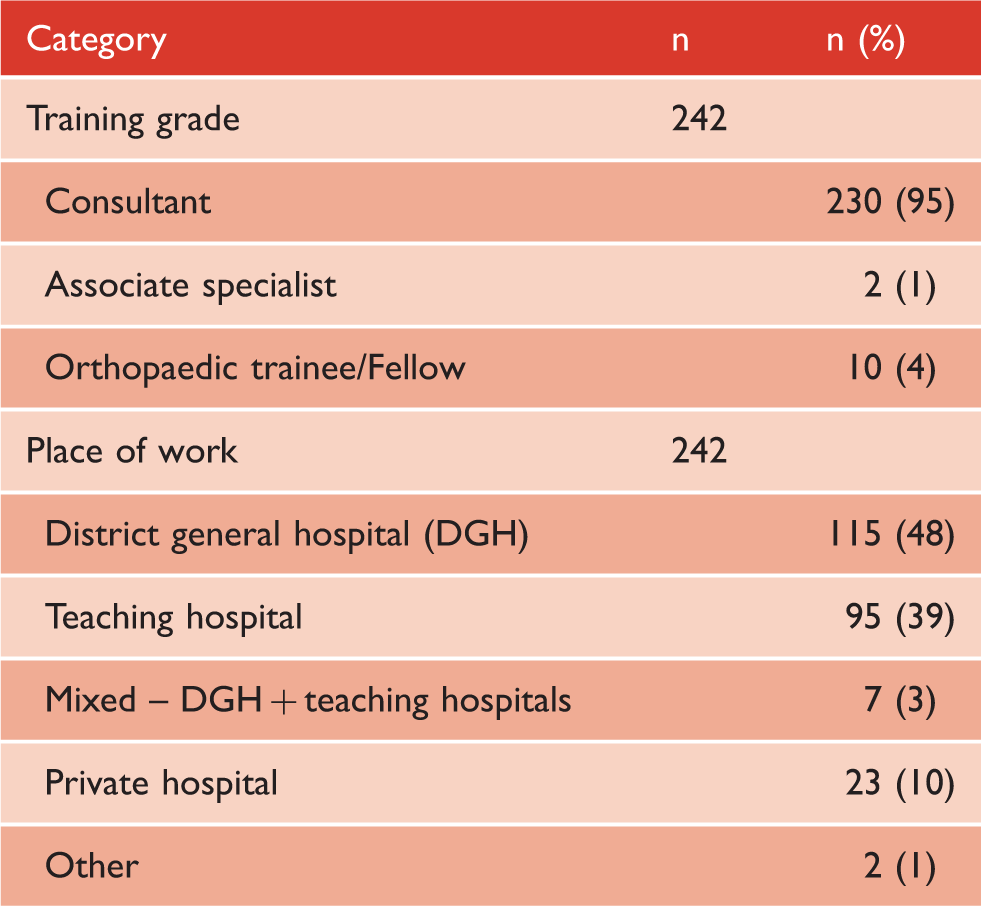
Characteristics of the respondents
Training grade and place of work of respondents.
Surgical experience with distal biceps tendon repairs
Surgeon-reported practice for DBT ruptures.
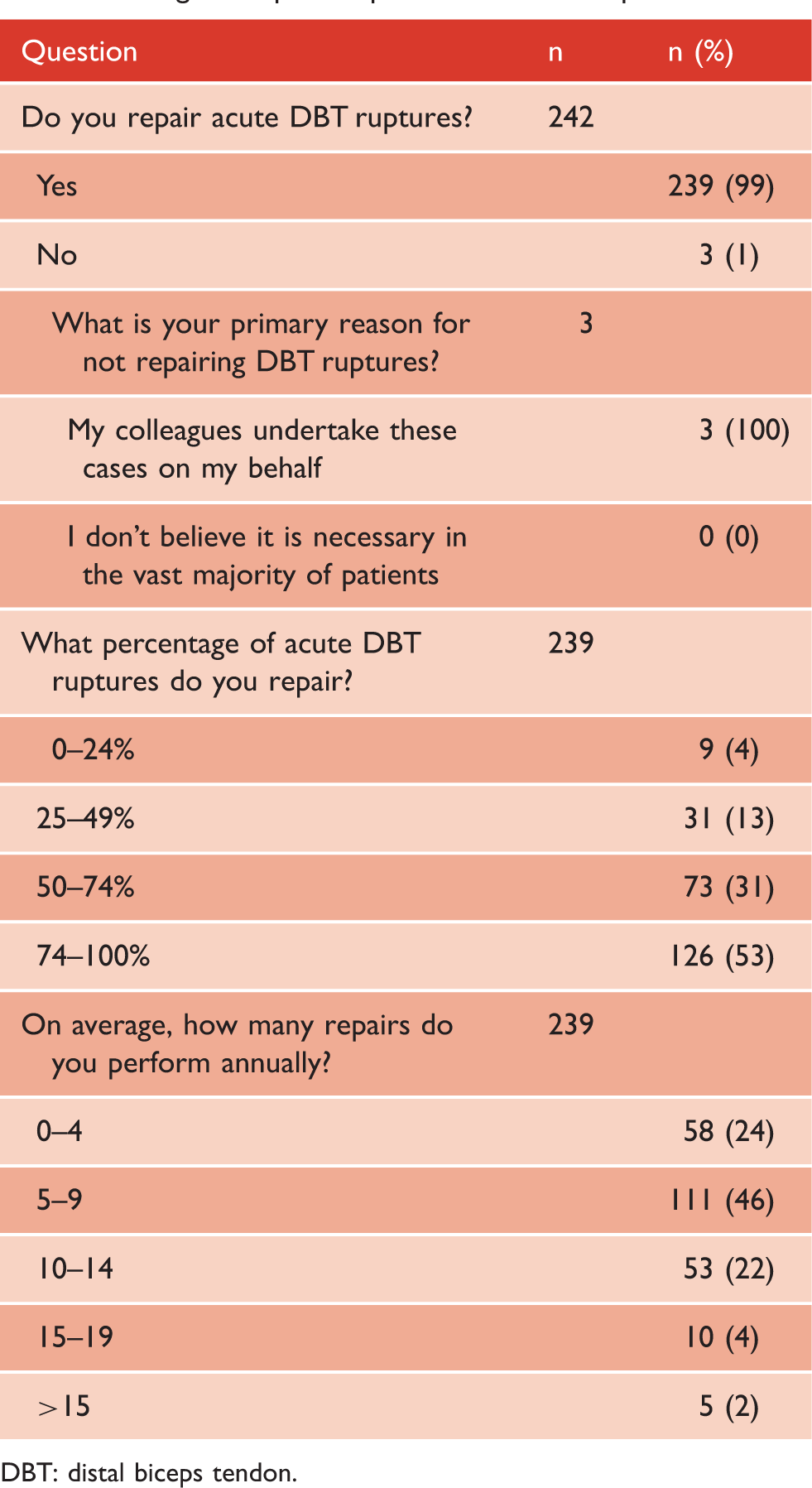
DBT: distal biceps tendon.
Clinical decision making
Clinical decision making for acute DBT ruptures.
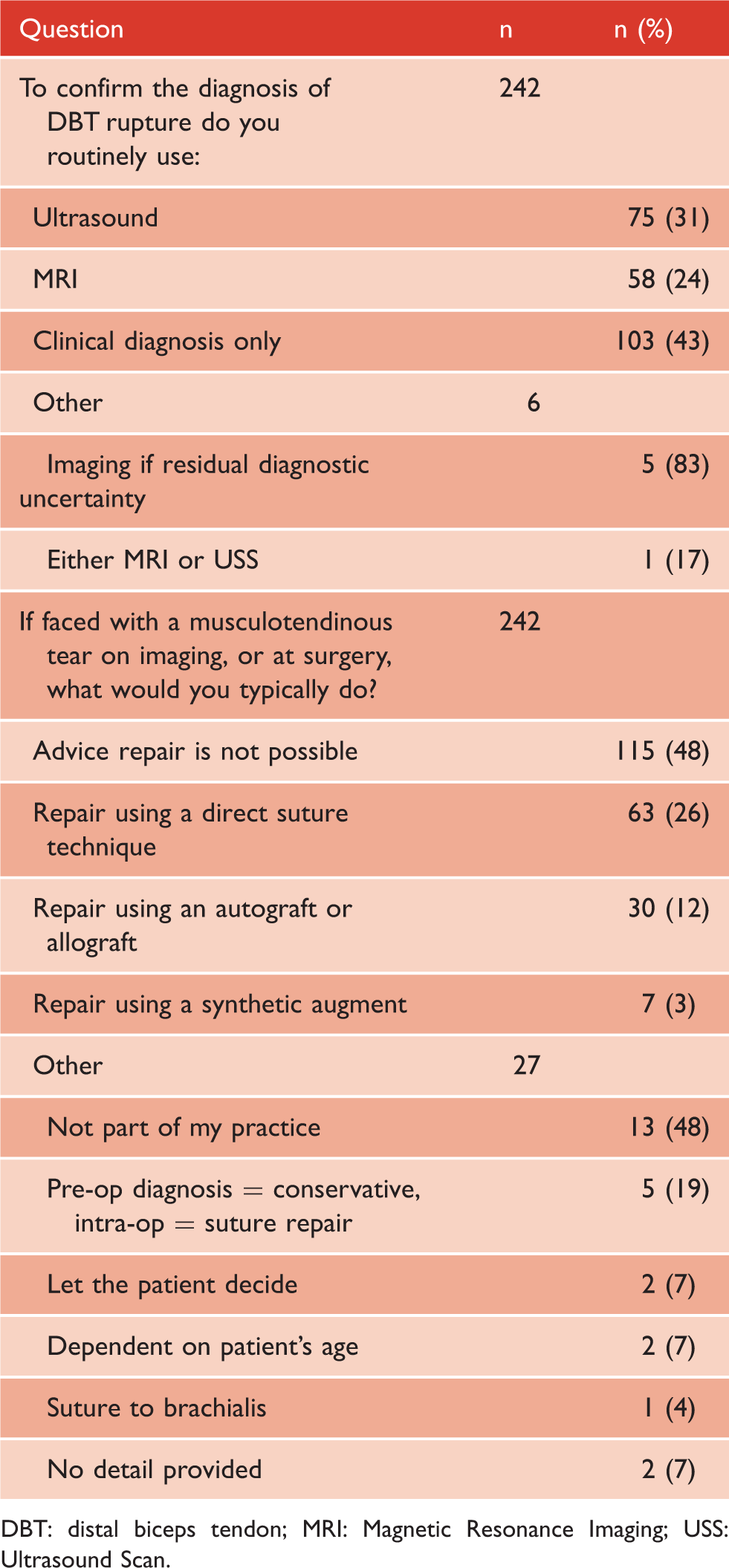
DBT: distal biceps tendon; MRI: Magnetic Resonance Imaging; USS: Ultrasound Scan.
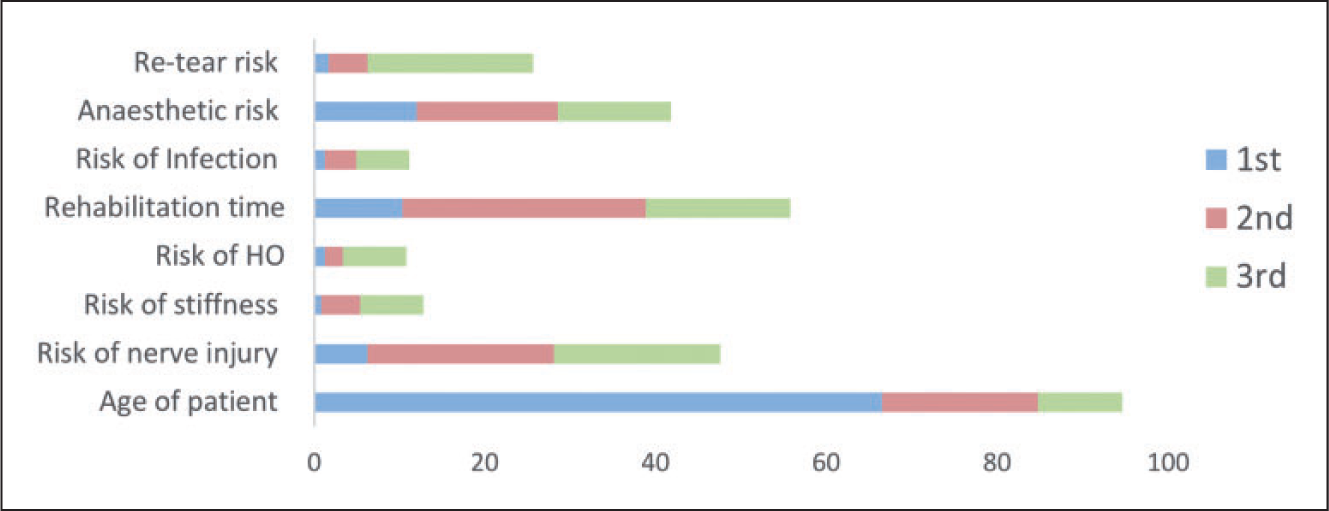
The majority (84%) of surgeons would have a repair of an acute distal biceps tear in their dominant arm and 67% for their non-dominant arm. When asked to provide the top three factors influencing a recommendation to undertake surgical fixation, the patient’s occupation (91%), age (86%) and restoration of strength (71%) were the most commonly reported factors (Figure 1). Conversely, consideration of hand dominance (26%), avoidance of cramps (18%) and cosmesis (8%) were of less importance to surgeons during clinical decision making. When recommending the non-surgical management of acute distal biceps ruptures, 95% of surgeons reported that the age of the patient was an important feature (Figure 2). Concerns over neurological injury (48%), rehabilitation duration (56%), anaesthetic risk (42%) and re-tear risk (26%) also emerged as important factors influencing the non-operative decision-making process. Only 11% of respondents reported access to a patient-directed information sheet to aid joint decision making.
Ranking of the three most important features influencing a recommendation for surgery. Ranking of the three most important features influencing a recommendation for non-operative management.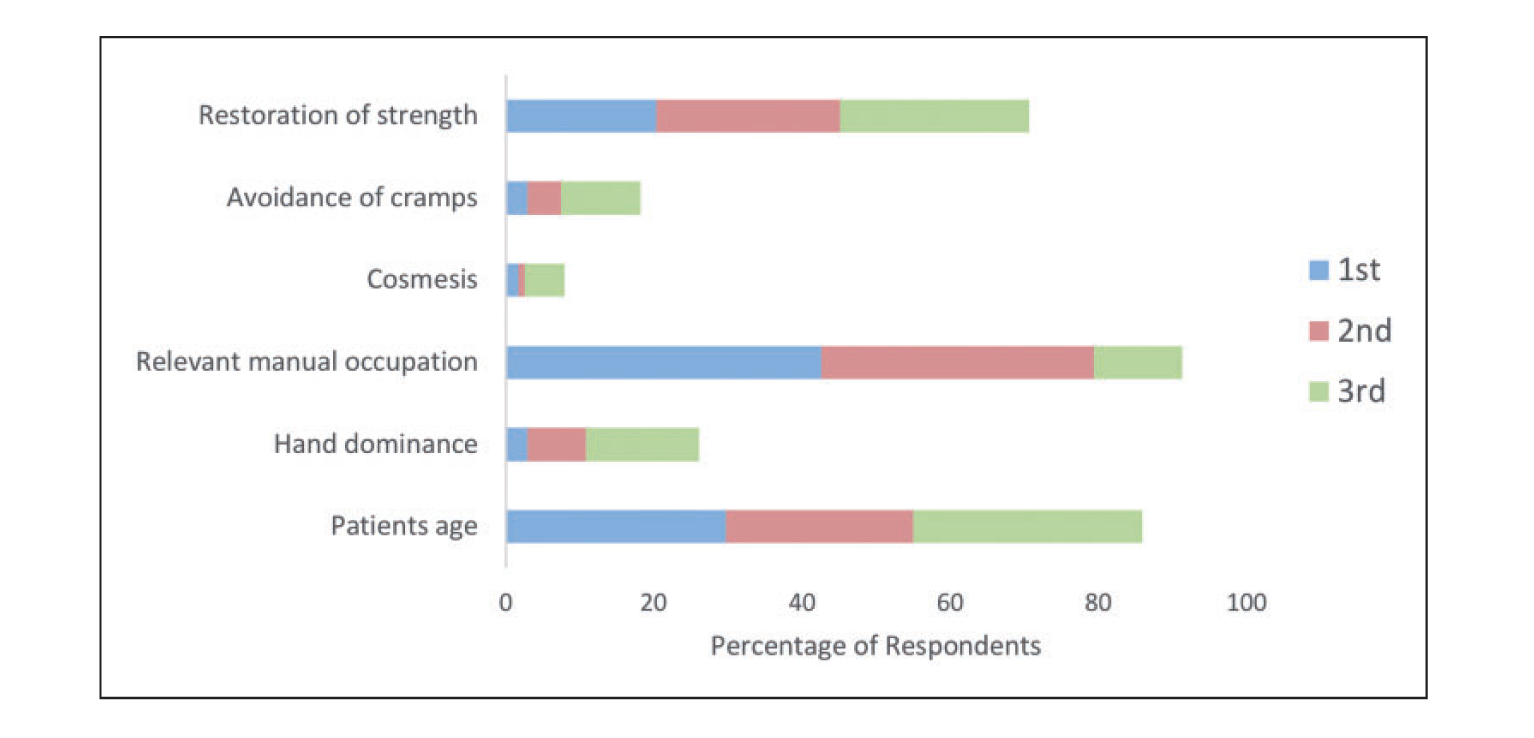
Surgical technique and post-operative protocols
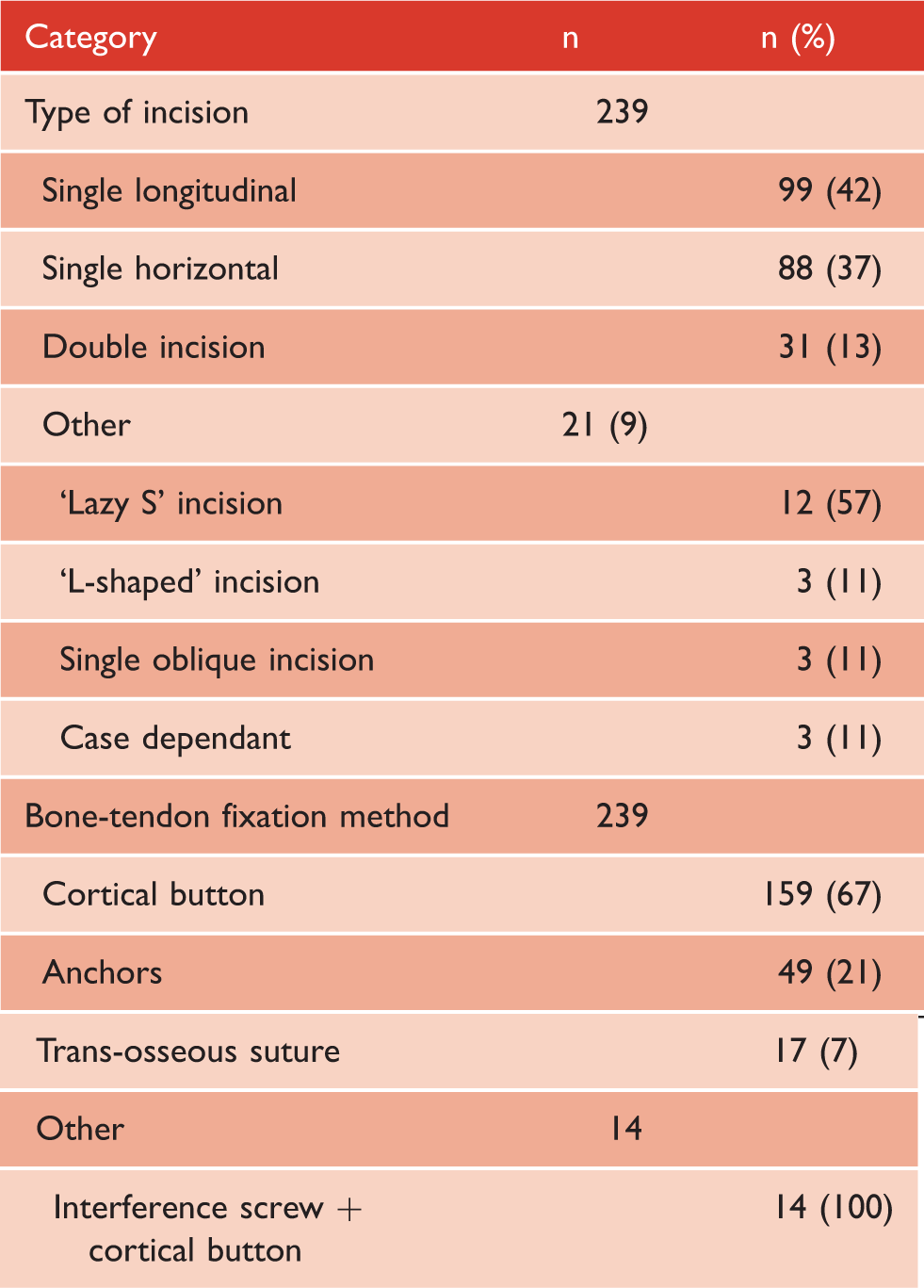
Surgical technique for distal biceps repair.
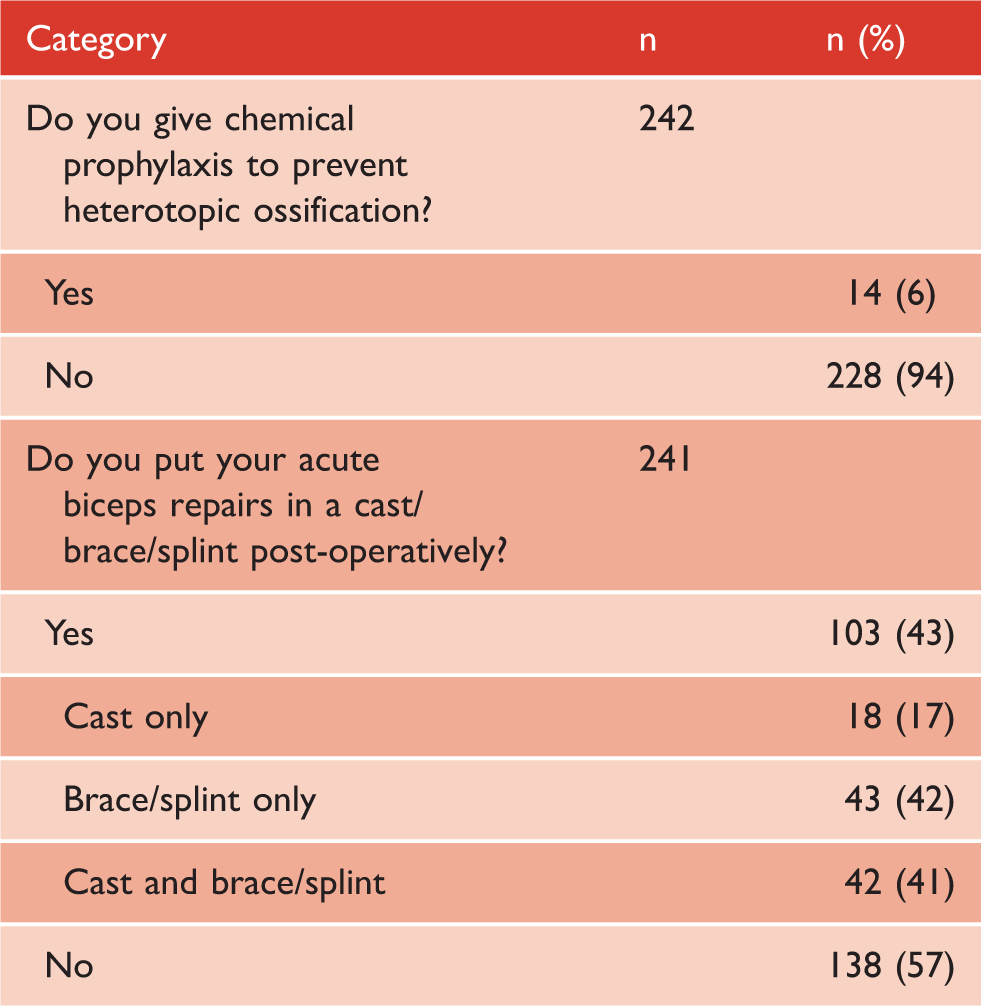
Only 6% of surgeons prescribed chemical prophylaxis with the aim of preventing HO. (Table 5) All of those prescribing chemical prophylaxis reported prescribing a non-steroidal anti-inflammatory drug. A minority of respondents (43%) prescribed a cast or brace/splint in the post-operative period. Of those who routinely recommend post-operative immobilisation, 17% prescribe a cast only for on average of two weeks (range 1–6 weeks), 42% a brace only for six weeks (range 2–12 weeks) and 41% a cast/brace combination for on average of two weeks (range 1–6 weeks) in cast and a further four weeks (range 2–8 weeks) in brace.
Future research
Post-operative protocol for distal biceps repair.
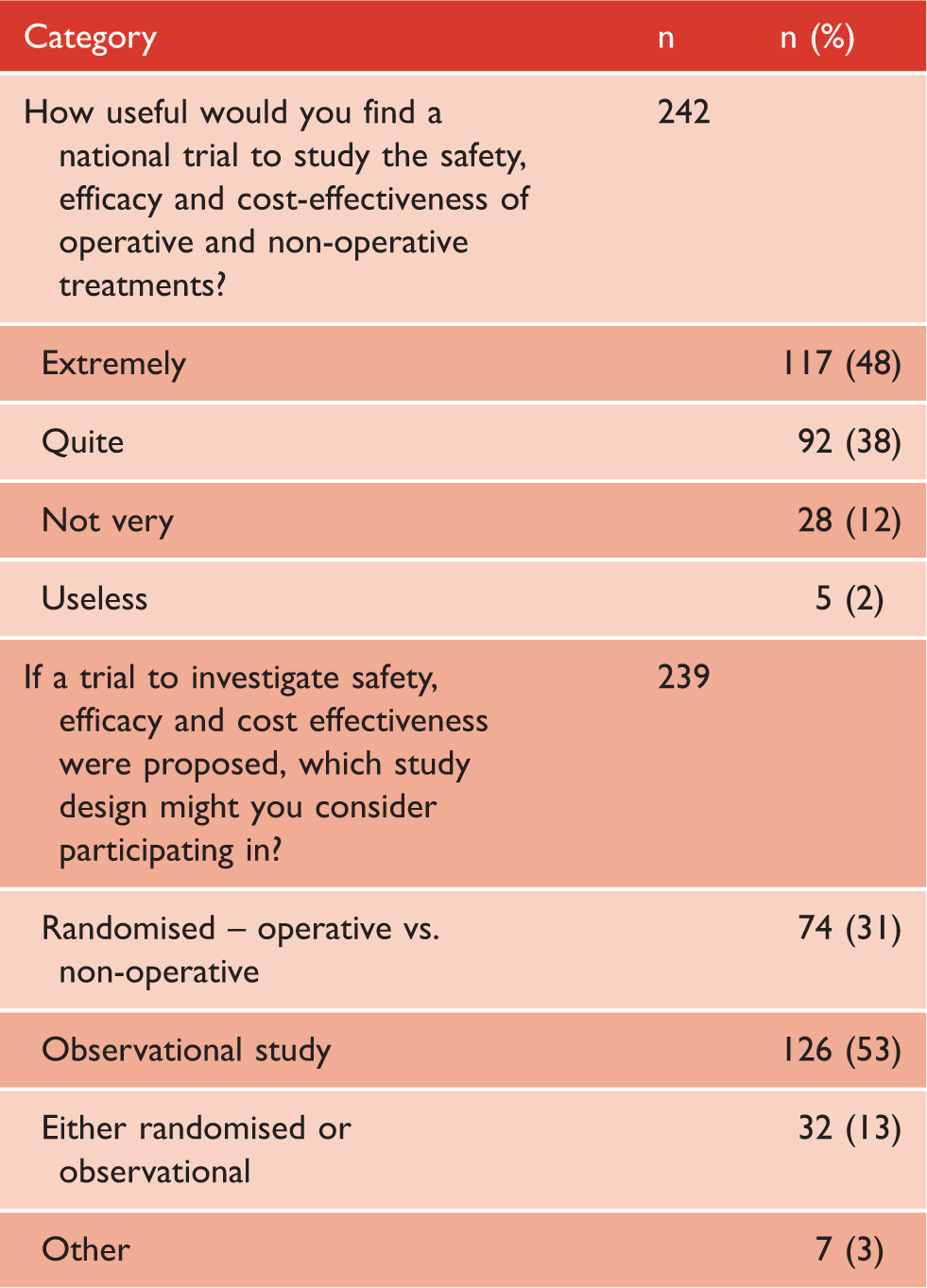
Role of research in acute distal biceps repairs.
Discussion
The incidence of acute distal biceps ruptures and the popularity of surgical repair both appear to be increasing.3,8 We carried out a survey of surgical society membership to assess current diagnostic, surgical and post-operative practice for acute distal biceps repairs.
The majority of UK respondents undertake the surgical repair of acute distal biceps ruptures and do so in the majority of patients, mirroring the rising trend towards operative intervention observed in other countries. 3 A large proportion of surgeons would also have their own, hypothetical, DBT repaired in their dominant arm. Interestingly, a smaller proportion would have their non-dominant distal biceps repaired, yet handedness did not rank among the top three clinical variables influencing a recommendation of surgery to patients. Similarly, a previous study among orthopaedic surgeons found differences between personal treatment preferences and those recommended to patients. 9 In part, this can be explained by a better appreciation of their own occupational, sporting and social factors and highlights the importance of shared decision making when discussing treatment options.
Overall, the majority of surgeons relied on Ultrasound (US) or MRI to confirm a diagnosis of distal biceps rupture. Despite a reported sensitivity of 83–100% for the hook-test10,11 and 95% accuracy for the biceps squeeze test, 12 less than half would depend solely on clinical diagnosis.
Despite widespread support for surgical intervention, our survey has also highlighted that concern over serious complications, in particular nerve injury, influences a recommendation for non-operative management. This position was historically advocated by Robert Dobbie who was ‘thoroughly convinced that exposure of the tubercle was impractical and unwise’. 13 Recent meta-analyses have confirmed an overall high rate of complications (20–28%), with neuropraxia of the lateral antebrachial cutaneous nerve (9%) and HO (3%) particularly common, while permanent motor deficits of the radial, posterior interosseous and anterior interosseous nerves appear to be uncommon.7,14 In light of these risks, the surgical community has an ethical obligation to provide robust evidence that operative management outweighs the risk of harm. Unfortunately, the current research landscape is limited to a small number of retrospective case series 6 with the only prospective trial to date subsequently withdrawn from publication. 15
As with all survey-based data collection, there is potential for a response bias and the survey frame potentially also limits the generalisability of the findings of this survey – soft tissue elbow surgery also being undertaken by a proportion of hand surgeons or general trauma surgeons not represented in the BESS membership. The achieved response rate was low, although it was not that dissimilar from that achieved in similar surveys of the BESS surgical membership.16,17 BESS members, and in particular those who are more likely to respond to a survey, are not necessarily representative of the wider upper limb surgical community and may include more research-oriented surgeons.
Despite the aforementioned limitations, a strong theme from the respondents was the need for robust multi-centre clinical trials, with greatest support for an observational study investigating the safety, efficacy and cost effectiveness of operative and non-operative treatments for acute distal biceps ruptures. Clearly, in any future trial it is important that the study protocol does not discourage surgeons from recruiting. This survey has highlighted a diverse range of surgical incisions, fixation methods and post-operative protocols, offering support for a broad, pragmatic, methodological approach towards surgical technique and post-operative immobilisation.
Conclusions
Amongst UK upper limb surgeons who responded to this survey, the surgical repair of acute distal biceps ruptures is widely adopted, and while the majority of patients are offered operative repair. Patient age, occupation and restoration of strength were the most important factors driving a recommendation of operative management. There is currently a paucity of evidence to support the surgical repair of acute distal biceps ruptures with survey participants expressing support for a future observational or randomised control trial assessing the safety, efficacy and cost-effectiveness of operative treatment.
Supplemental Material
sj-pdf-1-sel-10.1177_17585732211032960 - Supplemental material for Treatment of acute distal biceps tendon ruptures – A survey of the British Elbow and Shoulder Society surgical membership
Supplemental material, sj-pdf-1-sel-10.1177_17585732211032960 for Treatment of acute distal biceps tendon ruptures – A survey of the British Elbow and Shoulder Society surgical membership by MJ Baldwin, AC Watts, CA Peach, J Phadnis, H Singh and SE Gwilym in Shoulder & Elbow
Footnotes
Acknowledgements
We would like to thank the BESS Research Committee and all the BESS members who kindly completed this survey.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Review and Patient consent
This was a voluntary survey of health care professionals and therefore formal ethical review was not sought. However, the survey was approved by the BESS committee.
Guarantor
Senior author – SEG.
Contributorship
All authors contributed equally to survey design and manuscript preparation. The authors MJB and SEG undertook data collection, extraction and analysis. All work was overseen by the author SEG.
Availability of data + material
The dataset used and/or analysed during the current study is available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.