
Abstract
Purpose
Distal biceps tendon (DBT) injuries are relatively uncommon. Controversies exist regarding the best approach, leading to variations in treatment. This study aims to understand the preferences and practices of orthopedic surgeons regarding management of DBT injuries, as well as assess the feasibility of a future pilot randomized controlled trial (RCT) to evaluate the impact of various surgical factors on patient outcomes.
Methods
A cross-sectional international survey was conducted amongst surgeons treating patients with DBT injuries. The survey included questions about treatment preferences, surgical techniques, case volumes, and interest in participating in a future RCT.
Results
Responses from 491 orthopedic surgeons from 26 countries/territories were obtained. Most surgeons had limited exposure to DBT ruptures. Variations were observed in the work-up process, with some relying solely on clinical examinations while others used diagnostic imaging. A single incision approach was the most common surgical technique, and tendon fixation with suspensory cortical buttons was frequently preferred. Most surgeons did not explore or repair the bicipital aponeurosis. Interest in participating in a future RCT varied for different surgical controversies.
Conclusion
This survey provides valuable insights into surgeons’ preferences and practices for DBT injury management. The study highlights the need for standardization in the work-up process and the use of evidence-based guidelines. Current practices may be influenced by factors such as training, implant availability, and costs. The survey also identified surgeons and centers interested in collaboration for future multicenter trials, allowing for equitable access to surgical collaboration opportunities and addressing the lack of evidence in DBT rupture treatment.
Level of Evidence
Level V, expert-opinion.
Introduction
Distal biceps tendon (DBT) injuries are relatively uncommon, with an incidence of 1.2–2.6 per 100,000 inhabitants per year.1,2 These injuries constitute approximately 3% of all tendinous injuries and are more prevalent in the dominant arm of males in their 5th and 6th decade of life. 3 The most common mechanism of DBT injury is active elbow flexion during an eccentrically applied load.2,4,5 Manual labor, weight training, regular tobacco and anabolic steroid usage have been reported as risk factors.1,6–8
Overview of survey respondents’ demographic information.
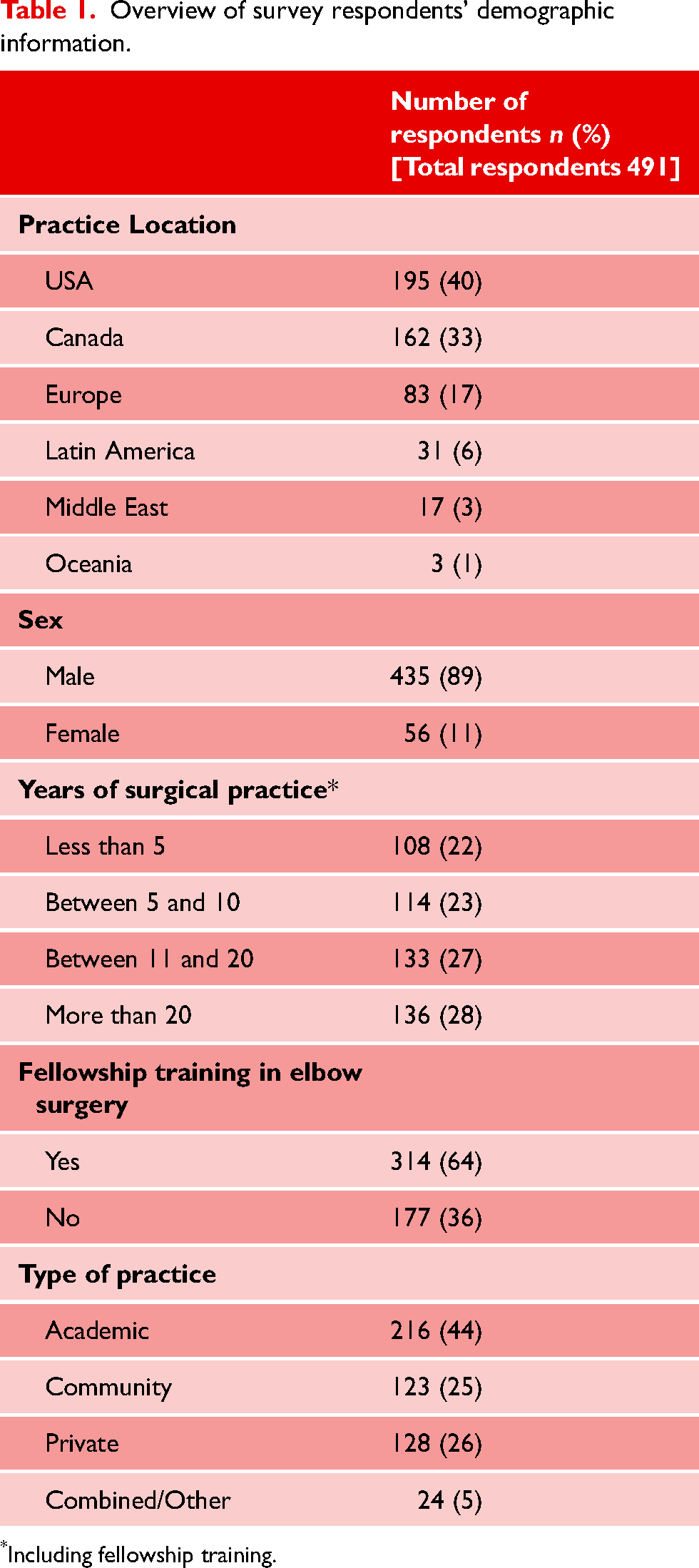
Including fellowship training.
Treatment options include both nonoperative and operative management. 9 Nonoperative approaches are often preferred for elderly and/or low demand patients who can tolerate the cosmetic deformity and strength loss associated with the injury. On the other hand, operative management is typically recommended for active patients who strive to regain their pre-injury range of motion and endurance. Several biomechanical and clinical studies have supported good functional outcomes with surgical management.4,10,11 Despite the numerous studies published in the last decade, many controversies persist regarding the best approach in DBT injuries treatment, leading to significant variation in management amongst surgeons.9,12–15
As most evidence in this topic comes from case-series and non-randomized studies, current evidence is inconclusive and, therefore, higher quality evidence is needed to guide the surgical community when treating these patients. An important first step in investigating these controversies involves an understanding of current surgeons’ preferences and practices as well as possible barriers in implementation of a pilot trial where the authors plan to assess how the number of incisions, type of DBT repair (single vs double bundle) and repair augmentation with bicipital aponeurosis (BA) impact patient outcomes when surgically treated.
The primary objective of this international survey is to ascertain the treatment preferences of orthopedic surgeons regarding surgical management of DBT injuries. We aim to investigate the overall variations in surgical approach, including the number of surgical incisions utilized, the type of surgical fixation and implants employed, and other surgical techniques and modifications (e.g., concomitant bicipital aponeurosis repair). Additionally, a secondary objective is to determine surgeons’ DBT repair volumes and assess the feasibility of involving the surveyed participants in a future pilot randomized controlled trial (RCT). This trial will evaluate the potential impact of three factors on surgical outcomes: 1) the number of surgical incisions utilized, 2) concomitant bicipital aponeurosis repair augmentation, and 3) the type of repair technique employed (single vs double bundle).
Materials and methods
Ethics
This study was granted final ethics approval by the authors institution (project number #10550).
Study design
The study is a cross-sectional international survey consisting of a questionnaire to determine surgeons’ current practice and preferences when treating DBT injuries.
Eligibility criteria
Practicing surgeons in upper extremity, shoulder and elbow, or orthopaedic trauma, and current fellows who perform DBT repair surgeries were eligible to answer the survey. Surgeons affiliated with orthopaedic associations from either English or Spanish speaking countries were invited to participate and answer an online survey. In the survey instructions, surgeons who did not treat patients with DBT tears were asked not to answer the survey. The following Orthopaedics Societies/Associations were contacted and accepted to disseminate the survey amongst their members: 1) American Shoulder and Elbow Surgeons (ASES) Society; 2) Canadian Orthopaedic Association (COA); 3) Sociedad Española de Cirugía de Hombro y Codo (SECHC); 4) Sociedad Chilena de Traumatología y Ortopedia (SCHOT); and 5) Saudi Orthopaedic Association (SOA).
Survey development
The questionnaire was developed by four upper extremity surgeons who developed the survey based on different aspects of patient care with a suspected/diagnosed DBT injury and identified the current gaps of knowledge and controversies on this topic. The survey was tested and improved through administration of sample copies to other surgeons and residents at a local orthopaedic trauma residency program. Agreement on questions was reached through a Delphi method. 16 A copy of the questionnaire can be found in the appendix (S1 – DBT preferences survey).
Survey administration
The participants were contacted through e-mail by the participants Orthopaedic Surgery Associations. Most organizations sent the survey twice to their members. The survey was piloted and administered using SurveyMonkey® (Momentive Inc., CA, USA). As a quality control measure, the opening statement of the survey instructed the respondents not to answer the survey more than once to avoid duplication.
Sample size
As this survey is intended to provide information about surgeons’ current practice and preferences when treating DBT injuries, a specific sample size was not targeted. However, we did anticipate that with greater than 50 completed questionnaires, we would have enough data and information to develop a protocol for a pilot randomized controlled trial surrounding this topic.
Questionnaire domains
The survey was designed to identify the current level of variations in surgical treatment of DBT injuries amongst orthopaedic surgeons, such as number of incisions used, method of tendon fixation, timing of surgery, and whether to repair a ruptured bicipital aponeurosis (BA). In addition, the survey collected demographic data such as country of training and practice, years of practice, type of clinical practice, and training level among others.
The survey was also intended to assist in identifying possible centers for research collaboration in this area. We surveyed aspects such as surgeons’ DBT repair case volumes, perceived area of controversies regarding DBT repair and willingness to participate in future trials on this topic. The survey was conceived as a tool to help the research team gauge the level of the interest among surgeons in engaging in future research to help resolve these controversies.
Data analysis
Surveys were entered into a secure study-specific database. Descriptive analyses, including frequency, counts and percentages, were calculated for all gathered data. Continuous data is presented as means with 95% confidence intervals (95% CI).
Results
Demographic characteristics
Responses were collected from 491 orthopaedic surgeons from 26 countries/territories. Forty percent of the respondents were from the US, followed by 33% from Canada, 17% from Europe, 6% from Latin America, 3% from the Middle East, and 1% from Oceania (Table 1).
Most respondents had a formal fellowship training in elbow surgery (n = 314, 64%), and have been in practice for over 10 years (n = 269, 55%).
Most surgeons encountered either five or less cases (n = 160, 33%) or between six and ten cases yearly (n = 153, 31%) (Figure 1). The majority of respondents (n = 374, 76%) declared that they treated greater than 75% of cases surgically.
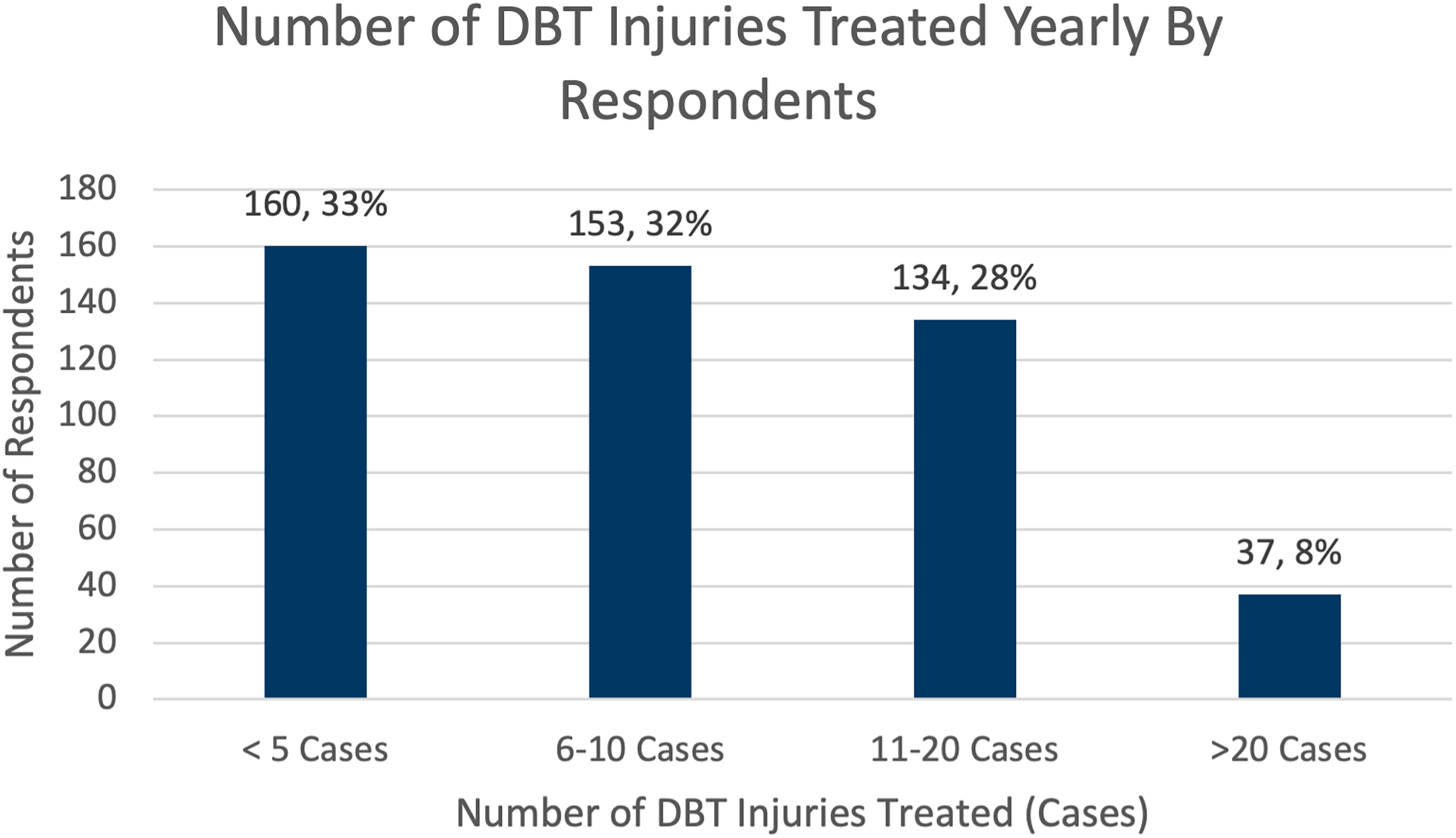
Overview of survey respondents’ DBT injury encounters over career.
DBT injuries treatment decision-making
When considering surgical versus conservative treatment of DBT injuries, most surgeons ranked age as the most important factor (n = 149, 33%). This was followed by the patients’ professional demand (n = 98, 22%), and level of physical activity (n = 96, 21%) (Figure 2). From the 144 surgeons (29%) who declared using an age cut-off for considering conservative treatment, the mean age cut-off was 64 years (95% CI 62.6–65.4).
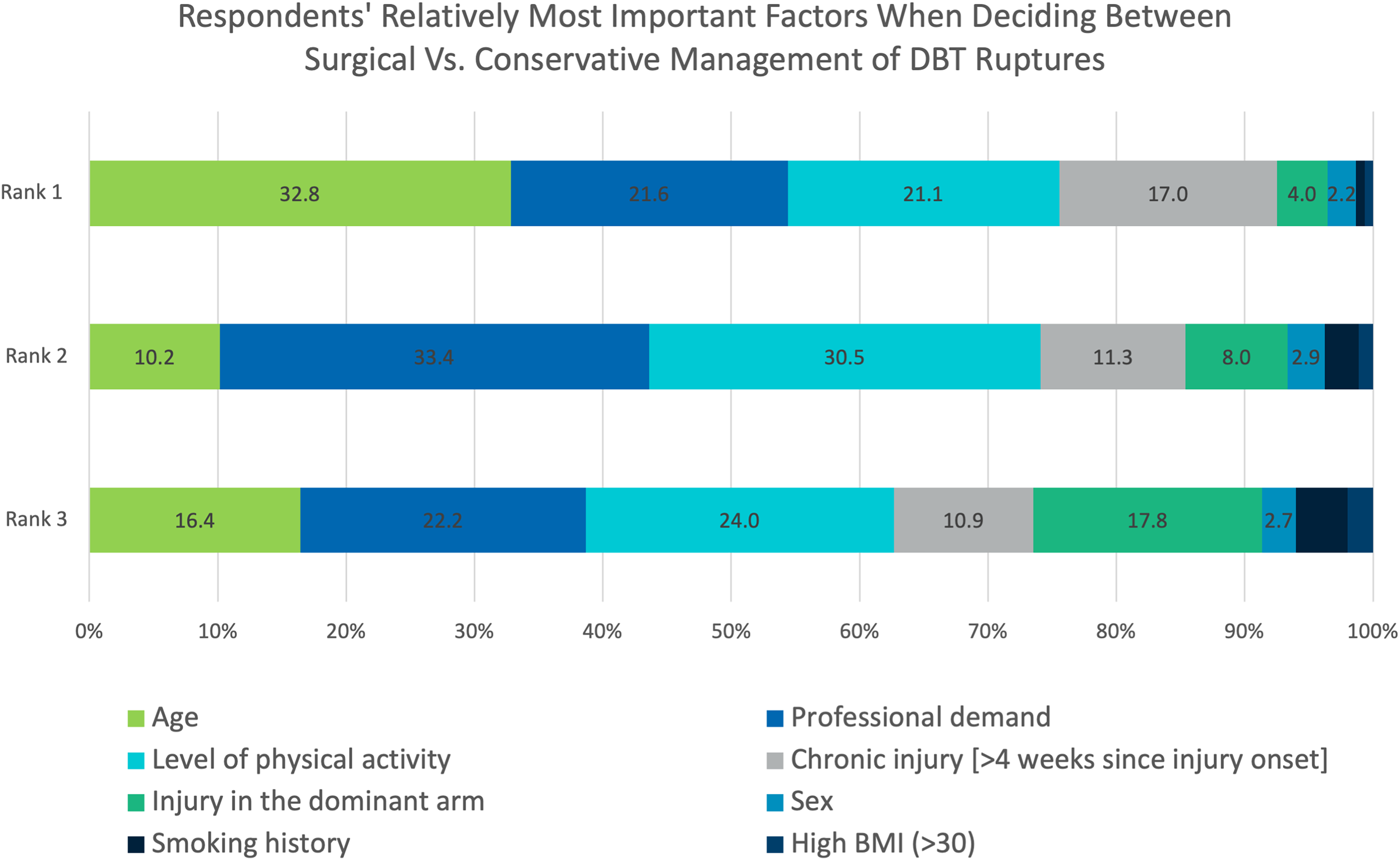
Factors ranked most important when deciding between conservative or surgical management of DBT injury.
DBT injuries work-up
The most frequent methods to diagnose DBT rupture mentioned by the respondents were the use of x-rays and magnetic resonance imaging (MRI) (n = 116, 24%), followed by only MRI (n = 100, 20%), and only clinical examination without additional imaging (n = 48, 10%). From analysis by geographic regions, interestingly surgeons from Canada were more likely not to order diagnostic imaging or perform only x-rays (39%) compared to surgeons in other countries (11%).
DBT surgical treatment preferences
An anterior single incision approach was the most frequent approach used (n = 340, 69%), followed by a two incision (one anterior and one posterior) technique (n = 73, 15%). Both acute and chronic injuries undergoing repair were found to be most preferably treated with suspensory cortical buttons (e.g., Endobutton) (acute: n = 211, 48%; chronic: n = 177, 45%). Other common methods included a combination of interference screws with suspensory cortical buttons (acute: n = 96, 22%; chronic: n = 95, 24%) and transosseous sutures/bone tunnels (acute: n = 65, 15%; chronic n = 61, 15%) (Figure 3).
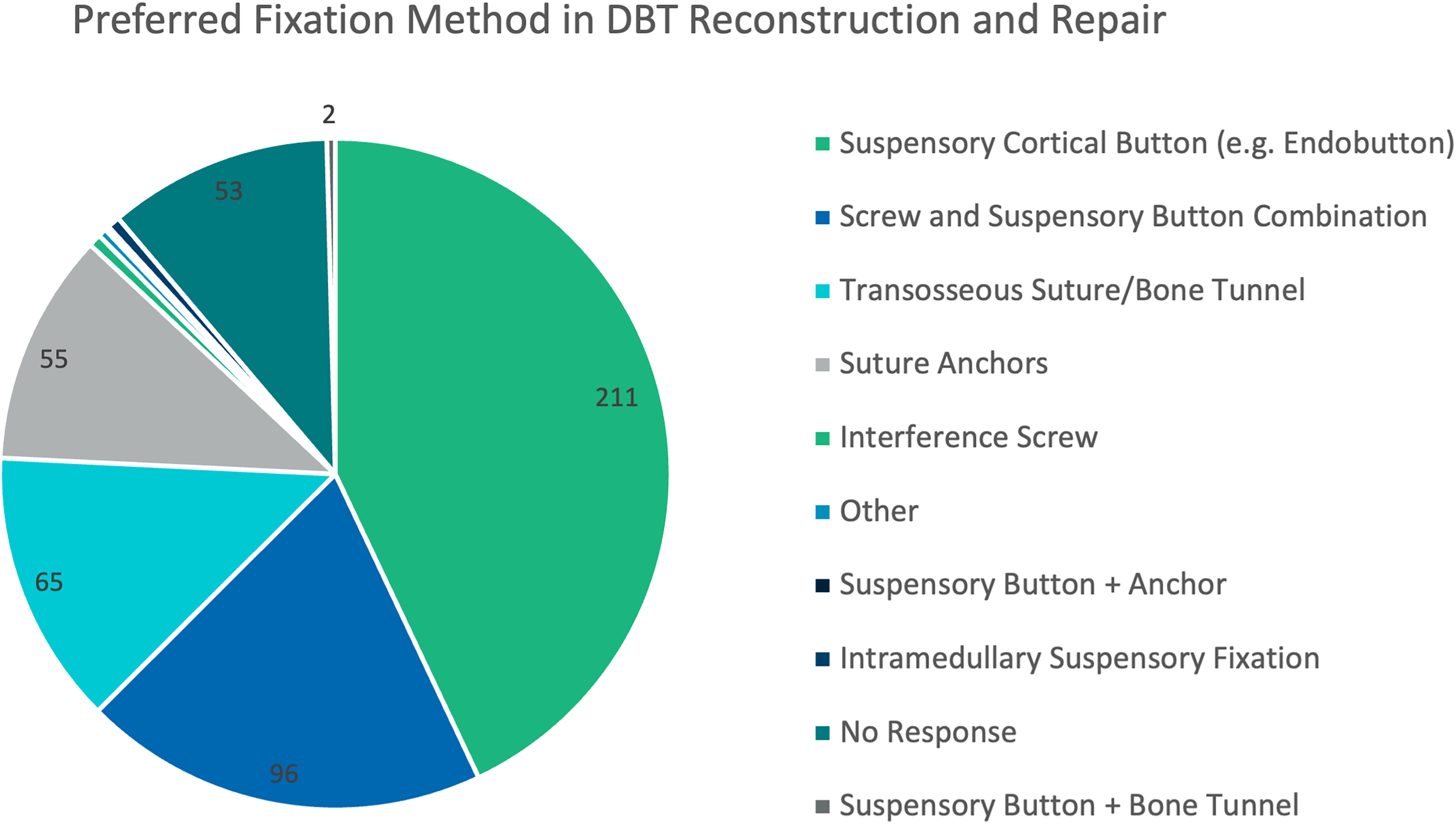
Fixation methods used in reconstruction for acute and chronic DBT injuries*.
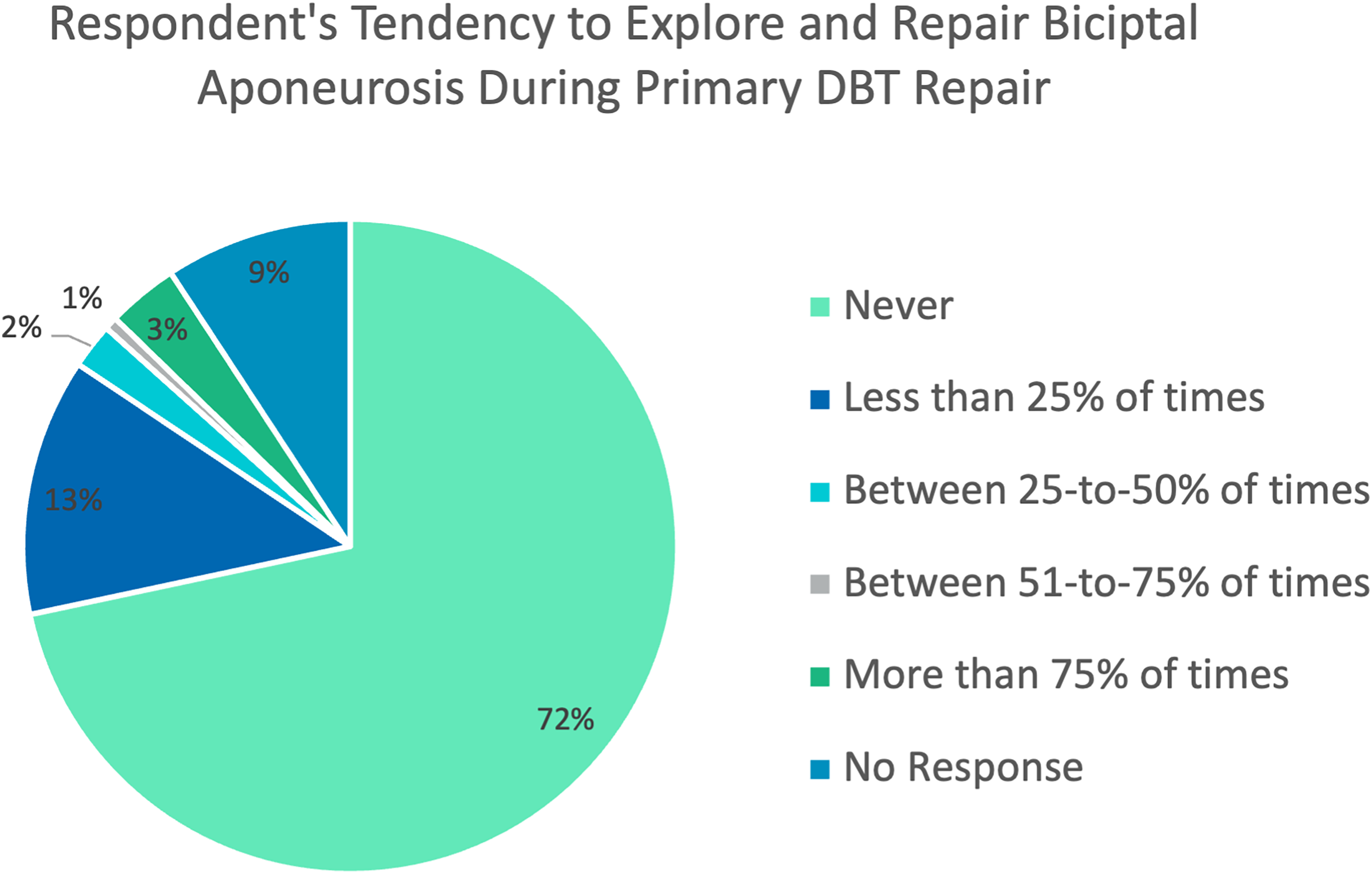
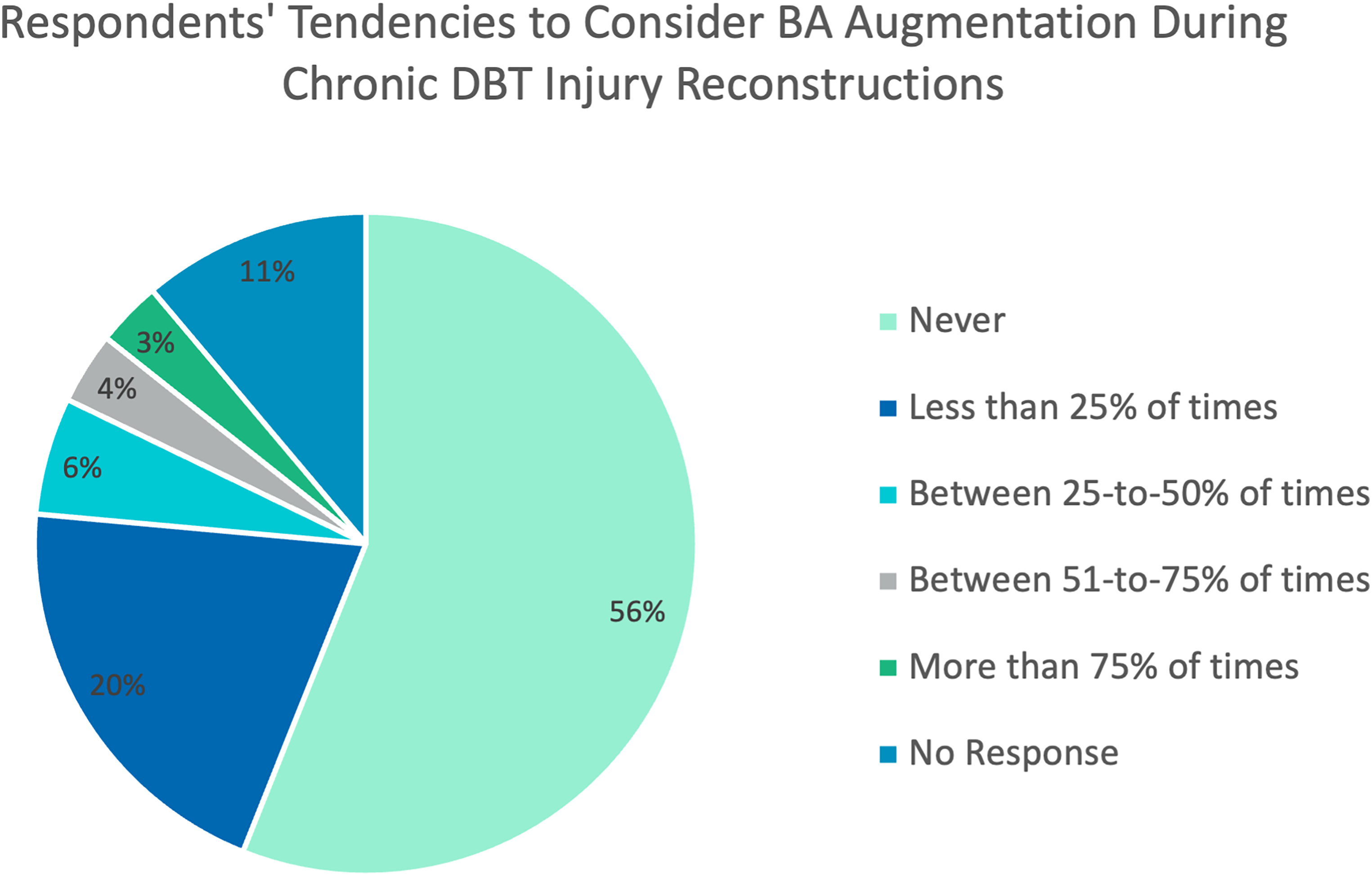
Most surgeons (n = 278, 64%) would not consider augmenting a chronic DBT rupture repair/reconstruction with concomitant BA repair. From those who would consider augmenting it (n = 154, 36%), only 7% (n = 32) would repair the BA to augment their repair/reconstruction in more than 50% of their cases (Figure 4). Moreover, 74% (n = 329) of surgeons do not explore nor repair a torn BA in the setting of acute injuries (Figure 5).
Bicipital aponeurosis utilization by respondents to augment chronic DBT reconstruction (%).
Performance of torn bicipital aponeurosis repair during DBT repair in respondents (%).
When facing chronic cases, 25% of surgeons declared they did not perform DBT reconstructions. From those performing reconstructions, most preferred the use of allograft (75%), with Achilles tendon allograft being the most utilized (44%). Additionally, most surgeons (62%) would not consider doing a biceps to brachialis tenodesis to treat patients in chronic cases.
Regarding postoperative immobilization and rehabilitation, the majority of surgeons immobilized their patients at 90° of flexion and neutral rotation. However, nearly one out of five surgeons (18%) immobilized their patients in supination. Surgeons authorized their patients to start active elbow extension and flexion around 4 weeks’ time (3.7 weeks for active extension and 4.4 weeks for active flexion). Strengthening exercises were reported to be allowed around 10 weeks after surgery (9.7 weeks).
Interest in surveyed surgical controversies and research collaboration
Most surveyed surgeons 69% (n = 293) considered that there was no need for a trial comparing single and double incision approaches. However, one third (n = 137, 32%) declared they would be interested in participating in a pilot trial comparing a single incision single bundle repair vs two incision double-bundle repair (separate repair of short and long heads tendon bundle) for DBT ruptures. Moreover, surgeons showed slightly less interest regarding repairs with vs without BA augmentation with 28% (n = 118) of surgeons declaring they saw a need for a trial comparing DBT injuries with concomitant BA repair vs no repair. In addition, 21% (n = 90) of surgeons were interested in participating in a clinical trial comparing DBT repair with and without BA repair.
Discussion
Our study on surgeons’ preferences when treating DBT injuries provides useful information on both current treatment choices and areas for future research in the management of distal biceps tendon (DBT) injuries. It also evaluates the potential for global collaborations in research initiatives to evaluate the management of these injuries. This international survey provides valuable insights from almost 500 surgeons providing treatment to patients with DBT injuries.
One of the interesting findings of our international survey was that it revealed that most surgeons have limited exposure to management of DBT ruptures (∼63% seeing 10 or less cases a year), and most cases seen do end up with surgical management. Therefore, considering the average surgeon expertise, it seems not only reasonable but prudent to concentrate DBT reconstructions cases, which are more challenging, in centers with higher volumes to achieve better surgical outcomes. Therefore, it was not surprising to observe that one out of four surgeons providing treatment for patients with DBT injuries did not perform reconstructions.
Our data showed that one of the main differences identified in surgeons’ practices was related to the work-up process of patients with DBT injuries. Interestingly, some surgeons relied purely on clinical examinations, while others order MRI, x-ray, ultrasound, or a combination of them to confirm the diagnosis and guide treatment. This is notable given that some authors advocate for the use of clinical examination alone for the diagnosis of this injury. For example, some argue that the hook test (alone or combined with the passive forearm pronation test, the biceps crease interval test, and the bicipital aponeurosis flex test) 17 surpasses the MRI with regards to sensitivity and specificity.18,19 With that however, others have also suggested that a negative hook test might not be enough to exclude a complete DBT rupture. 20 Special precaution is needed in chronic cases, as false negatives have mainly been reported in that population. This might be due in part to inadvertent hooking of the bicipital aponeurosis or scarred tissue in this group. 21 Cost-effectiveness studies and clinical guidelines are needed to standardize the diagnostic approach to these injuries to avoid missing valuable time during the work-up process that may delay the surgical treatment and compromise the ability to achieve a primary DBT repair.
Another interesting finding was the fact that despite the controversy regarding the use of a one or two incision approach in repairs of DBT ruptures, 15 there was a clear trend towards preferring to use a single incision approach (∼70%). This might change in the upcoming years due to newer techniques and fixation methods necessitating the use of a two-incision surgical approach. Surgical controversies regarding the number of surgical approaches,14,15 type of fixation used and the possible beneficial role that BA repair has in the surgical management of these injuries22,23 showed less dispersion than anticipated. As previously mentioned, most surgeons are still treating these patients using a single incision surgical approach and prefer to use suture-buttons to achieve tendon fixation. Also, the majority do not explore nor repair the BA neither consider using it to augment a DBT reconstruction. Despite some evidence suggesting potential benefits from BA repair augmentation due to its proprioceptive and biomechanical properties, few surgeons have incorporated this idea in their routine practice.10,13
Despite these being more common practices, there is a clear lack of evidence to guide surgeons in treating DBT rupture. Also, current practices may be influenced by surgeons training, industry-driven courses, implant availability, costs, and preferences.
This survey also helped to identify centers interested in collaborating on multicenter international trials that we are planning to conduct. Some controversies explored in our survey such as the use of BA repair did not receive much interest, though others such as investigating the use of a single vs. double bundle repair received positive feedback. Overall, our study supports the use of international surveys as a useful tool to identify surgical volumes, and gauge interest in collaboration prior to conducting either a pilot or a definitive multicenter trial. Ultimately, it allows for more equitable access to opportunities for surgical collaboration by recruiting teams that do not normally engage in such trials and may be underrepresented in the literature.
Limitations
Despite achieving a large sample size for a survey in orthopaedics, our study only surveys five surgical societies and associations. This impedes the study from drawing stronger conclusions and assumes the practice preferences found in this study to be representative of what is being done in other non-surveyed countries/territories. Another critical point of elaboration is the inability to calculate a true response rate as many of the societies involved (eg., Canadian Orthopedics Association, the Saudi Orthopedic Association, and the Chilean Society of Orthopedic Surgery) include members who do not perform upper extremity surgery so the number of potential eligible participants to participate in the study in those associations was impossible to be determined. It was also deemed impossible to accurately approximate these numbers given the number of societies involved and variation in proportions of members eligible to respond.
In addition, surveying surgeons imposes keeping the survey short enough to achieve high response rates to avoid fatigue and boredom while answering. This limitation in survey length hampered our ability to explore certain aspects with further detail. One key aspect of decision making, especially given the recent emphasis of shared-decision making, is patient preferences – the impact of which this survey was not able to explore.
Lastly, the substantial variation in practice and preferences observed among surgeons treating patients with DBT injuries emphasizes the necessity for high-quality studies that offer evidence-based guidance to the surgical community. These studies are vital for establishing the best practices in managing this specific patient population. International surveys can serve as valuable tools to identify centers and surgeons with significant case volumes, who may be willing to participate in collaborative research initiatives. This is particularly crucial in low-frequency conditions and pathologies where obtaining a large sample size poses a challenge for certain study designs. By leveraging the expertise and collaboration of such centers and surgeons, meaningful advancements in research and treatment outcomes can be achieved.
Conclusions
The survey results provide valuable insights into the current practices and preferences of orthopedic surgeons in treating DBT injuries. These findings can be used to guide future research and identify potential collaboration centers. The study highlights the importance of further research to address the ongoing debates on the best surgical approach in DBT repair and to provide evidence-based clinical guidelines.
Supplemental Material
sj-docx-1-sel-10.1177_17585732231215504 - Supplemental material for Distal biceps tendon injuries treatment: A survey of orthopaedic surgeons’ current practice and preferences
Supplemental material, sj-docx-1-sel-10.1177_17585732231215504 for Distal biceps tendon injuries treatment: A survey of orthopaedic surgeons’ current practice and preferences by Carlos Prada, Zhi Li, Praveen Sritharan, Moin Khan, Francesc Marcano-Fernández, Latifah Al Mana and Bashar Alolabi in Shoulder & Elbow
Footnotes
Acknowledgments
We would like to acknowledge the following surgical associations/societies: 1) American Shoulder and Elbow Surgeons (ASES) Society; 2) Canadian Orthopaedic Association (COA); 3) Sociedad Española de Cirugía de Hombro y Codo (SECHC); 4) Sociedad Chilena de Traumatología y Ortopedia (SCHOT); and 5) Saudi Orthopaedic Association (SOA).
In addition, we would like to acknowledge the Department of Surgery from McMaster University for the First Cut Award granted for this project.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the First Cut.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.