
Abstract
Background:
Foot and ankle injuries are a common but underestimated problem in taekwondo. Detailed data on injury incidence rates (IIRs), patterns, and injury mechanism are missing.
Purpose:
The primary aims were to evaluate the prevalence of foot and ankle injuries and the exposure-adjusted IIR of elite taekwondo athletes during matches while training (ie, sparring) and in competitions. The secondary aims were to evaluate injury site, type, sport-specific mechanism, and time loss.
Study Design:
Descriptive epidemiology study.
Methods:
Athletes from a single national Olympic taekwondo training center were assessed prospectively for foot and ankle injuries over 4 years (between January 1, 2016, and December 31, 2019). Data were collected regarding number and type of injuries, anatomic location, and total exposure time during training and competition for each athlete. Injury mechanism and dominant foot were assessed via personal interview. Time loss from sport was analyzed retrospectively. The injury prevalence and IIR were calculated. Correlation between mechanism and injury type, location, and dominant foot was evaluated. Time loss according to location and injury type was assessed. The chi-square test and Fisher exact test were used to test for differences in sex, age, and taekwondo experience and for comparison of injury location and type, injury mechanism, and side dominance, respectively. Training and competition IIRs and prevalence were calculated with 95% CIs (for Poisson rates).
Results:
From an initial 107 athletes, 79 (73.8%) were included in the final data set. Of these athletes, 38 were injured (n = 112 injuries) for a prevalence of 48.1% (95% CI, 43%-52%). The overall IIR of the ankle joint was 13.14 injuries per 1000 athletes (95% CI, 1.5-25.9) and was significantly higher during competition versus training (P < .001). Ankle joint injuries were most common (n = 71; 63%). Significantly more noncontact versus contact ankle ligament injuries (n = 46; 83%) occurred (P < .001). The forefoot (n = 18; 66%) was mainly affected by contact injuries (P < .001). Time loss was the highest for midfoot fractures (mean ± SD, 23.0 ± 0.6 days; range, 23-24 days).
Conclusion:
Noncontact ligamentous ankle injuries were most common, with a higher incidence during competition. Improvement of strength, endurance, and postural stability under strain is recommended for prevention.
Taekwondo is a traditional Korean martial art combining foot (tae) and hand (kwon) techniques. It is among the most popular martial arts worldwide and became an official Olympic discipline in 2012. 4 The Olympic taekwondo style is a dynamic full-contact sport characterized by head-height kicks, jumping spinning kicks, and fast kicking techniques. The goal is to score by hitting the opponent’s trunk and head or by knockout. There is a variety of forward and backward kicks, ranging from simple 1-leg kicks to dynamic jumping kicks with both feet in the air. Athletes usually hit their opponents with the calcaneus, the instep, or the dorsum of the foot. Therefore, protection gear for the feet and shin bones is mandatory in competition and sparring fights. One of the most common and spectacular kicks is called “the roundhouse kick,” which provides a powerful attack using a force up to 2000 N in elite athletes. 5 Independent of the fighting technique, athletes need the ability to adjust their body weight in different motions without losing balance in the process of releasing the force at the target. 12 This ability is important for taekwondo competitions and demands a high level of muscular strength, postural stability, and coordination in both legs in a highly competitive environment. Research interest for this sport has grown after evidence of high injury risk to the lower limbs in comparison with other Olympic sports. 9 Several studies 9,14,17 have identified the foot and ankle as the anatomic region with the highest risk for injury in taekwondo. A prospective 10-year observation by Park and Song 16 showed that injuries of elite taekwondo athletes during training mostly affected the lower extremities, with a significantly higher injury incidence rate (IIR) for the knee and ankle joint as compared with other locations. Unfortunately, the authors did not provide any information regarding the exact anatomic location or the mechanism of injury. While injury patterns and mechanisms for the hand and wrist have been recently investigated for taekwondo, detailed data on injuries of the foot and ankle are currently lacking.
The primary aims in the current study were to evaluate the injury prevalence rate, recurrence rate, and exposure-adjusted IIR for foot and ankle injuries incurred by elite taekwondo athletes during training and competition over a 4-year period. The secondary aims were to evaluate injury site, type, and mechanism, as well as related time loss. The authors hypothesized that because of their experience, specific athletic training, and mandatory foot protection gear, these athletes would have smaller foot and ankle IIRs and fewer noncontact injuries (vs contact) during competition (vs training).
Methods
Study Population
The protocol was approved by a university research ethics board, and participants gave their informed consent. All 107 athletes from a national Olympic taekwondo training center were investigated prospectively for training and competition injuries over 5 years (January 1, 2014–December 31, 2019). A substudy within this cohort was conducted between January 1, 2016, and December 31, 2019, and included data regarding all foot and ankle injuries in the population.
Part of the sample was included in another study with a different inclusion period and aims, 7,19 and the descriptive information for these participants has been published previously. 7 All athletes were performing at the black-belt level, took part in a regular institutional training schedule with a frequency of 5 to 6 times per week, and participated regularly in competition fights during the study period. As requested by the official rules of the World Taekwondo Federation, the use of protective gear, including foot protectors, was mandatory for all athletes during training fights (ie, sparring) and competition fights and supervised by the attending medical staff (Figure 1).

Standard foot protection gear used during competition and training fights (left sock; dorsal, lateral, and medial views).
Data Collection
Data about fight exposure and injuries were recorded prospectively. All athletes were evaluated for foot and ankle injuries by experienced medical staff (team physician or physical therapist) during training sessions or competition (M.G., J.R.). In case of an acute injury, the athletes were examined by experienced sport orthopaedic specialists from an Olympic training center within the first week (M.G.). The exact injury type and location were based on clinical examination as well as radiologic results from ultrasound, radiographic, and magnetic resonance imaging data. Injuries were defined via criteria recommended by Junge et al 10 as “all injuries receiving medical attention regardless of the consequences with respect to absence from competition or training.” Data of athletes who finished their career during the study period or presented with incomplete medical documentation were excluded from final evaluation.
The prevalence of injury during the 4-year study period was calculated as the number of injured athletes divided by the number of athletes studied. The prevalence of subsequent injury was also calculated (number of athletes with multiple injuries divided by number of injured athletes). As previously published, 7 IIR was defined as the number of injuries per 1000 hours of exposure; separate IIRs were calculated for fighting time during training (ie, sparring time) and competition. 21
For classification of injury type, the Orchard Sports Injury Classification System–10 was used. 18 Analysis of injury location was performed according to anatomic regions of the foot and ankle. Time loss attributed to injury was defined as time elapsed until return to full-contact taekwondo training and was analyzed retrospectively.
The mechanism of a foot or ankle injury was assessed by the medical staff attending the fights, from personal interviews on the same day of the injury (M.G., J.R.). The injury was classified as contact (impact of the foot or ankle with the opponent) or noncontact (occurring while standing or moving). The dominant foot was defined as the preferred foot for delivering kicks and was indicated by the athlete during a personal interview. This definition of the dominant limb has been described for martial arts athletes. 14
Statistical Analysis
Injury data were obtained prospectively but analyzed retrospectively. Radiographs were reviewed retrospectively. Statistical analysis was performed using SPSS Statistics for Windows (Version 24; IBM Corp).
The chi-square test was used to determine statistical differences in sex, age, and taekwondo experience. The Fisher exact test was used for comparison of injury location and type, injury mechanism, and side dominance. Training and competition IIRs were calculated with 95% CIs (for Poisson rates) using R statistical software (R Core Team, Version 3.5.1). For comparison of IIRs, the exact Poisson test was used. All reported P values are 2-tailed, with an alpha level <.05 considered significant. Descriptive data are reported as mean, SD, and range unless otherwise stated.
Results
From the original 107 athletes at the Olympic training center, 79 (73.8%) were included in the final data set with an exposure time of 8495 hours. The mean age of the athletes was 19.3 ± 3.2 years (range, 15-27 years), with 9.6 ± 3.3 years of taekwondo experience (range, 6-20 years). There was no significant difference between male and female athletes according to injuries or taekwondo experience. Most participants (91%) described the right foot as dominant (Table 1).
Characteristics of Participants and Injuries a

a Values are presented as No. (%) or mean ± SD (range) unless noted otherwise. IIR, injury incidence rate. Dashes indicate not applicable.
b Significant difference between training and competition (P < .001).
Over the study period, 112 injuries in 38 athletes were recorded, leading to a prevalence rate of 48.1% (95% CI, 43%-52%). Of the 112 recorded injuries, 73 (65.2%) were recurring; thus, the prevalence of subsequent injury was 68.4% (95% CI, 54%-81%). The highest IIR (per 1000 hours) was calculated for ankle joint injuries during competition (20.9; 95% CI, 15.4-26.5) versus training (2.9; 95% CI, 2.0-3.7). The IIR for foot injuries was lower: 6.8 (95% CI, 5.4-8.2) for competition and 2.7 (95% CI, 2.0-7.9) during training. A significantly higher IIR was seen during competition than with training regarding ankle as well as foot injuries (P < .001 for both) (Table 1).
The most common injury types were ligamentous (63%) mainly affecting the anterior talofibular ligament, followed by bruising (10%), fractures (10%), and joint dislocations (7%). The most common injury location was the ankle joint (63%) and the phalanges (24%). Ankle ligamentous injuries represented 49% of total injuries recorded. Significantly more ligament injuries occurred at the ankle joint as compared with all other locations (P = .001) (Table 2).
Injury Type According to Location

a Blank cells indicate counts of zero.
b Significant difference vs other locations (P < .001).
Noncontact injuries accounted for 63% of injuries, while 37% of injuries took place during contact with the opponent. Significantly more ankle ligament injuries were from a noncontact mechanism (P < .001) (Figure 2). In contrast, significantly more forefoot injuries had a contact mechanism (P < .001) (Table 3).

Foot and ankle injuries according to mechanism. ***P < .001.
Foot and Ankle Injury Locations and Injury Mechanism

a Bold P values indicate statistically significant difference between contact and noncontact injuries (P < .05).
b Not applicable for testing.
c Low or missing values.
The fractures in our cohort occurred almost exclusively during competition (91%). In the grouped analysis regarding the side dominance of athletes, there was a significant accumulation of ankle injuries and ligament injuries on the nondominant versus dominant side (P < .001 for both). The mean time loss for all foot and ankle injuries was 6.8 ± 5.1 days (range, 1-32 days). Fractures accounted for the longest time loss, with a mean of 12.0 ± 8.9 days (range, 4-24 days), equal to that for cartilage injuries with a mean of 12.0 ± 3.3 days (range, 1-32 days). According to location, the mean time loss for midfoot injuries was longest with 13.6 ± 9.7 days (range, 1-24 days) (Table 4).
Time Loss in Days According to Location and Injury Type
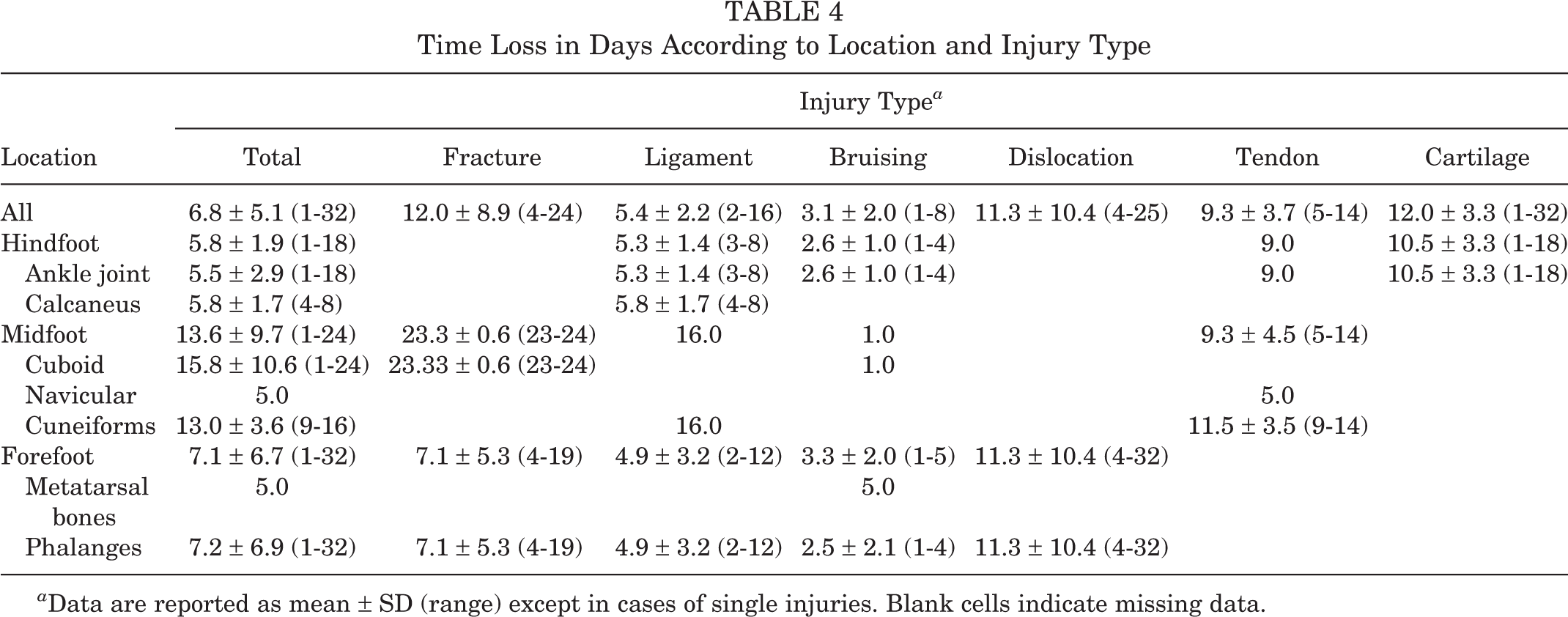
a Data are reported as mean ± SD (range) except in cases of single injuries. Blank cells indicate missing data.
Discussion
The most important finding of this study was a significantly higher IIR for acute foot and ankle injuries in elite taekwondo athletes during competition as compared with training. Injuries of the ankle joint were most common (63% of all injuries) and were most frequently ligament injuries of the anterior talofibular ligament (70%). There was a significant accumulation of ankle injuries and ligament injuries on the nondominant foot side (76%). Furthermore, significantly more noncontact injuries (75%) occurred at the level of the ankle joint, while contact injuries were usually related to the forefoot. Fractures, dislocations, and cartilage injuries resulted in a mean time loss of 12.0 days from sport, while ligament injuries accounted for only 5.4 days. The present study confirmed the findings of previous studies 9,15,17 regarding the high incidence of ankle injuries during competition.
As high-level taekwondo is extremely demanding physiologically and psychologically, the aggressive fighting style might lead to perceived exertion causing a lack of coordination. 1 Therefore, the number of ankle sprains and concomitant ligament injuries could rise when postural stability decreases owing to muscular imbalance, as demonstrated in previous studies for contact sports. 3,6 In addition, previous studies 6,13 in different sports have described limb dominance, body mass index, functional deficits in isokinetic strength, muscle reaction time, recurrent injuries, and lack of postural stability as intrinsic risk factors for lateral ankle sprains.
The role of the dominant foot for injuries in taekwondo has not been described in detail. In this study, significantly more ankle and ligament injuries (P < .001 for both) occurred on the nondominant side, which is referred to as the supporting leg in this sport. As most combat sports rely on kicks, athletes use the dominant foot for pinpoint kicking and usually shift their body mass slightly to the supporting back leg to generate stability, making the front foot easier to lift and increasing the speed of kicks at the same time. It is one of the most challenging tasks in high-level taekwondo to maintain balance while performing such complex maneuvers in a competitive environment. Furthermore, isokinetic strength and muscle reaction time might be diminished during competition as a result of rapid weight loss immediately before competitions. Regarding athletes achieving the required weight for their class, previous studies 2,11,22 have reported a magnitude of rapid weight loss before competition between 3% and 7% of body weight, resulting in reduced muscular strength and endurance.
Contact injuries in this study mainly affected the forefoot, as the feet are the main weapons and therefore prone to direct injury during attacks. During training, some athletes wear special shoes to protect their feet, but those shoes are not allowed during competition. Mandatory protection gear for competition consists of soft padding covering the dorsum of the foot. It is mainly to protect the midfoot and metatarsalia but leaves the toes widely unprotected. This design might explain the small number of injuries to the metatarsalia and the finding of significantly more contact injuries of the toes. Noncontact injuries of the phalanges might also be associated with the lack of toe protection, which can cause hyperflexion or hyperextension during rapid movements in combination with a high adherence of the phalanges to the mat due its rubber texture.
Hunt et al 8 conducted a study on foot and ankle injuries in elite collegiate athletes at a single institution. Among 37 contact and noncontact sports, the authors reported a mean time loss of 12.3 days and indicated that the prevalence of recurrence for the same injury accounted for 28% of affected athletes. Ankle sprains were reported among the most common recurrent injuries. The mean time loss of 6.8 days in taekwondo athletes indicates that foot and ankle injuries might be considered mild to moderate in this sport according to injury severity classification. 20 However, with a prevalence rate of 68.4% for subsequent injury, these injuries should not be underestimated. The observed mean time loss of 5.3 days for ankle ligament injuries suggests an underestimation of ankle injuries in combat sports. This finding emphasizes the need for specific criteria for return to competition and training based on strength, flexibility, endurance, and proprioception testing to prevent possible chronic ankle instability and loss of function over time.
Besides exact diagnosis and proper treatment, improvement of protective gear according to the described injury patterns might have the potential to reduce injury rates, especially since the dominant striking leg is more affected by contact injuries. Taping of the ankle joints in taekwondo during competition is widespread, but rules and regulations concerning application differ widely among tournaments. Therefore, integrating bracing of the ankle joint seems advantageous but is technically demanding because of the need for free range of motion in this sport. Reinforced padding of the forefoot and toes might also lead to more severe injuries of the opponent. Since a modification of protective gear requires an official process and has inherent problems, the training and teaching of correct kicking techniques seem most important. The observed toe fractures could be prevented by focusing on the midfoot for striking, as current protective gear provides the best padding for this part of the foot. Some athletes even tend to use unlicensed protection gear, such as shoes, during training, which conveys a false sense of protection. Consideration should be given to wearing licensed protective gear during training for better adoption to competition conditions.
Regardless of protection, the awareness of noncontact injuries to the foot and ankle region should be raised. The high IIR during competition fights suggests that the ankle on the nondominant side might be more vulnerable because of impairment of postural stability during competition as a result of fatigue. Specific training of proprioception and stability of the ankle with a focus on the nondominant foot should be an integral part of the training. Athletic training should focus on muscle strengthening of both legs and physical endurance to prevent fatigue. Neuromuscular control and coordination exercises should focus on an increased simulation of strain like that during competition. Possible preventive strategies for the nondominant leg could include the use of weight jackets during training of the single-leg stance and kicking, as well as trampoline training under strain and distraction.
Note, however, that all presented injury prevention recommendations in this study are based on a small sample size. To reduce the number of recurrent injuries, criteria-based return-to-sport decision making after lateral ankle ligament injury should be established. Continuing injury surveillance across multiple centers with staff education should be established to decrease injury rates. Besides that, results derived from prevention recommendations should continuously be evaluated with regard to reduction of time-loss injuries to demonstrate their effectiveness and improve acceptance among athletes, trainers, and officials.
Study Limitations
Despite the epidemiologic description of these injuries in our study, a selection bias may be assumed owing to the small number of athletes from 1 national training center, restricting generalization of results. No power analysis was conducted to determine which injuries are more common, given the naturally limited number of elite athletes. Furthermore, a selection bias might have occurred as attributed to athletes who did not complete the study. Different persons were participating in data collection, and some injuries might not have been assessed because of underestimation. Based on the nature of athletes participating in combat sports, this might have especially affected the inclusion of milder forms of injury types, such as bruising or joint ligament injuries. Athletes might not have reported an ankle sprain to medical staff if it did not affect their ability to continue fighting. It remains unclear in this study if injury risk skewed toward the remaining 79 athletes over time. The number of athletes included in the study was too small for calculation of IIR for each weight class. Time lost from participation attributed to injury might also have acted as a confounding factor. Finally, the evaluation of injury mechanism by interviewing certainly favors a recall bias, although it was done in a timely manner.
Conclusion
Noncontact ligamentous ankle injuries were most common, with a higher incidence during competition. Improvement of strength, endurance, and postural stability under strain is recommended for prevention. Multicenter or international studies can be performed to reinforce these findings. Sport-specific information about injury patterns and mechanism are needed for reduction of injury rates, improvement of protective gear, and prevention in full-contact combat sports.
Footnotes
Final revision submitted July 22, 2021; accepted August 24, 2021.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Paracelsus Medical University (2018-007).