
Abstract
Background:
Baseball is one of the most popular sports among high school– and college-aged men and carries significant injury risk; however, contemporary data comparing injury epidemiology between these competition levels are limited.
Purpose:
To compare the population-adjusted incidence, anatomic location, and diagnoses of baseball-related injuries presenting to US emergency departments (EDs) between high school and college-aged male athletes.
Study Design:
Descriptive epidemiological study.
Methods:
The National Electronic Injury Surveillance System (NEISS) was queried for baseball-related injuries from 2015 to 2024 in male patients aged 14 to 23 years. Patients aged 14 to 18 years were classified as high school–aged and those aged 19 to 23 years as college-aged. Incidence, anatomic location, diagnoses, and ED disposition were analyzed. Weighted national estimates were calculated using NEISS sample weights, and National Federation of State High School Associations and National Collegiate Athletic Association (NCAA) participation data were used to derive incidence rates (IRs) per 100 at-risk players and IR ratios (IRRs) with 95% CIs.
Results:
A total of 8335 baseball-related injuries were identified in the NEISS sample, corresponding to a weighted national estimate of 297,921 male athletes aged 14 to 23 years evaluated in US EDs for baseball-related injuries between 2015 and 2024. College-aged athletes had a higher injury incidence and were nearly 3 times as likely to be evaluated as their high school–aged counterparts (14.00 vs 5.23 per 100 at-risk players; IRR, 2.68; 95% CI, 2.65-2.70). Both groups exhibited a sharp decline in injury incidence in 2020, corresponding with the onset of the COVID-19 pandemic. The most frequently injured body parts in both groups included the face, head, ankle, and knee, and fractures were the most common diagnosis. IRRs for nearly all injuries were higher among college-aged athletes, particularly for shoulder injuries (IRR, 4.20; 95% CI, 3.44-5.14) and dislocations (IRR, 5.98; 95% CI, 4.62-7.74).
Conclusion:
This study showed that between 2015 and 2024, college-aged baseball players had significantly higher IRs of ED-treated injuries than their high school–aged peers across most body regions and diagnoses. College-aged athletes face elevated risks for more severe injuries requiring emergency care, including fractures, dislocations, and concussions, highlighting the need for preventive strategies tailored to the specific demands of higher competition levels.
Baseball is among the most widely played organized sports for adolescent and young adult male athletes in the United States, with >470,000 high school–aged and 36,000 college-aged participants annually.13,14 Participation confers health, developmental, and social benefits; however, the sport's repetitive and explosive demands with overhead throwing, sudden accelerations and decelerations while fielding and base running, and bat-to-ball impacts expose athletes to both acute trauma and overuse pathology.3,18,25 Prior exposure-based surveillance studies consistently identify upper-extremity injuries, particularly at the shoulder and elbow, as most common.3-5,18,19,25 Reported risk factors include older age, greater height, higher pitch velocity, and increasing sport specialization.1,15,16 Less is known about injuries treated in emergency departments (EDs), which may reflect more acute, traumatic, or severe presentations and injuries occurring outside formal athletic settings.
Limited comparative work suggests that, with increased intensity and volume of play, collegiate athletes may experience a greater burden of overuse and noncontact injuries. 25 Prior studies have indicated that upper-extremity overuse injuries occur more frequently at higher levels of competition, 14 while lower-extremity injuries (eg, ankle sprains) and facial injuries may be underreported in athletic training surveillance yet more prominent in ED data sets.1,26 Accordingly, ED-based data provide a complementary perspective on the acute care burden and full spectrum of baseball-related injuries.11,22
Few cross-level comparisons between high school and collegiate baseball athletes exist, and most relied on organized-sport surveillance systems that are now outdated. The most recent large-scale comparison reported data only through the 2004 to 2014 seasons and drew from dedicated high school and collegiate injury surveillance programs rather than from an ED-based, nationally representative data set. 25 Subsequent epidemiologic studies have narrowed their focus to specific anatomic regions or diagnoses rather than evaluating the full spectrum of baseball-related injuries across levels of play.1,2,4,5,12,15,19,22,25 An updated cross-level comparison is warranted, particularly across 2015 to 2024, a period that spanned the COVID-19 pandemic and potential shifts in sport participation and care seeking.
The purpose of this study was to provide an updated, comparative assessment of baseball-related injuries presenting to US EDs among high school– and college-aged male athletes. We aimed to compare population-adjusted incidence, anatomic location, and diagnosis patterns between cohorts. We hypothesized that college-aged athletes would demonstrate a higher overall incidence and greater injury severity than high school–aged athletes.
Methods
Database and Query
This cross-sectional epidemiologic study used data from the National Electronic Injury Surveillance System (NEISS) to evaluate baseball-related injuries treated in US EDs from 2015 through 2024. 24 NEISS samples approximately 100 hospitals using a stratified probability design to generate national estimates of consumer product–related injuries. Data are collected by trained hospital coders from ED medical records and, when necessary, follow-up telephone interviews. Because all patient data are deidentified and publicly available, institutional review board approval was not required.
Data Collection
Injuries were included if the patient was male, aged 14 to 23 years, and the incident was classified under NEISS baseball product codes. Patients aged 14 to 18 years were categorized as high school–aged, and those aged 19 to 23 years as college-aged. For each case, injury characteristics, anatomic location, diagnosis, and ED disposition were recorded.
Statistical Analysis
Weighted national estimates and 95% CIs were calculated using NEISS sample weights. Baseball participation data were obtained from the National Federation of State High School Associations and the National Collegiate Athletic Association (NCAA) to calculate at-risk populations.13,14 Incidence rates (IRs) were reported per 100 at-risk patients. IR ratios (IRRs) with corresponding 95% CIs were calculated to compare rates between high school– and college-aged athletes. IRRs were calculated using Poisson approximations, and confidence intervals were constructed using mid-P exact methods. Statistical analyses were performed using R (Version 4.4.1), and significance was set at α≤ .05.
Results
A total of 8335 baseball-related injuries were identified in the NEISS sample, corresponding to a weighted national estimate of 297,921 male athletes aged 14 to 23 years evaluated in US EDs for baseball-related injuries between 2015 and 2024. Male college-aged baseball players sustained significantly higher injury rates than high school–aged players, with an overall incidence of 14.00 versus 5.23 per 100 at-risk players. The corresponding IRR was 2.68 (95% CI, 2.65-2.70), indicating that college-aged athletes were more than twice as likely to present to the ED for baseball-related injuries than their high school–aged counterparts (Table 1).
Comparative Characteristics of Male Baseball Injuries by Age Group a

Data are presented as n (%) unless otherwise indicated. For the National Estimate columns, percentages are row percentages, calculated as the age-group national estimate divided by the combined national estimate for that row (High School + College)
Fatalities were too rare in college athletes to generate reliable estimates or IRRs.
Between 2015 and 2024, the IR of baseball-related injuries among high school athletes remained relatively stable, fluctuating by only 3.8 points. In contrast, college-aged athletes had higher injury rates than high school–aged athletes across the study period. From 2015 to 2020, the college-aged injury rate declined by 11.6 per 100 at-risk players. Both groups exhibited a sharp decline in injury incidence in 2020, corresponding with the onset of the COVID-19 pandemic (Figure 1).

Incidence rates among high school and collegiate athletes by year.
Injury Patterns
The most frequently injured body parts evaluated in the ED among both groups included the face, head, ankle, and knee, while fractures were the most commonly reported diagnosis (Figure 2). Weighted estimates showed that fractures accounted for 47% (n = 22,519) of facial injuries, 45% (n = 10,121) of finger injuries, and 43% (n = 1248) of upper arm injuries among athletes aged 14 to 23 years between 2015 and 2024.
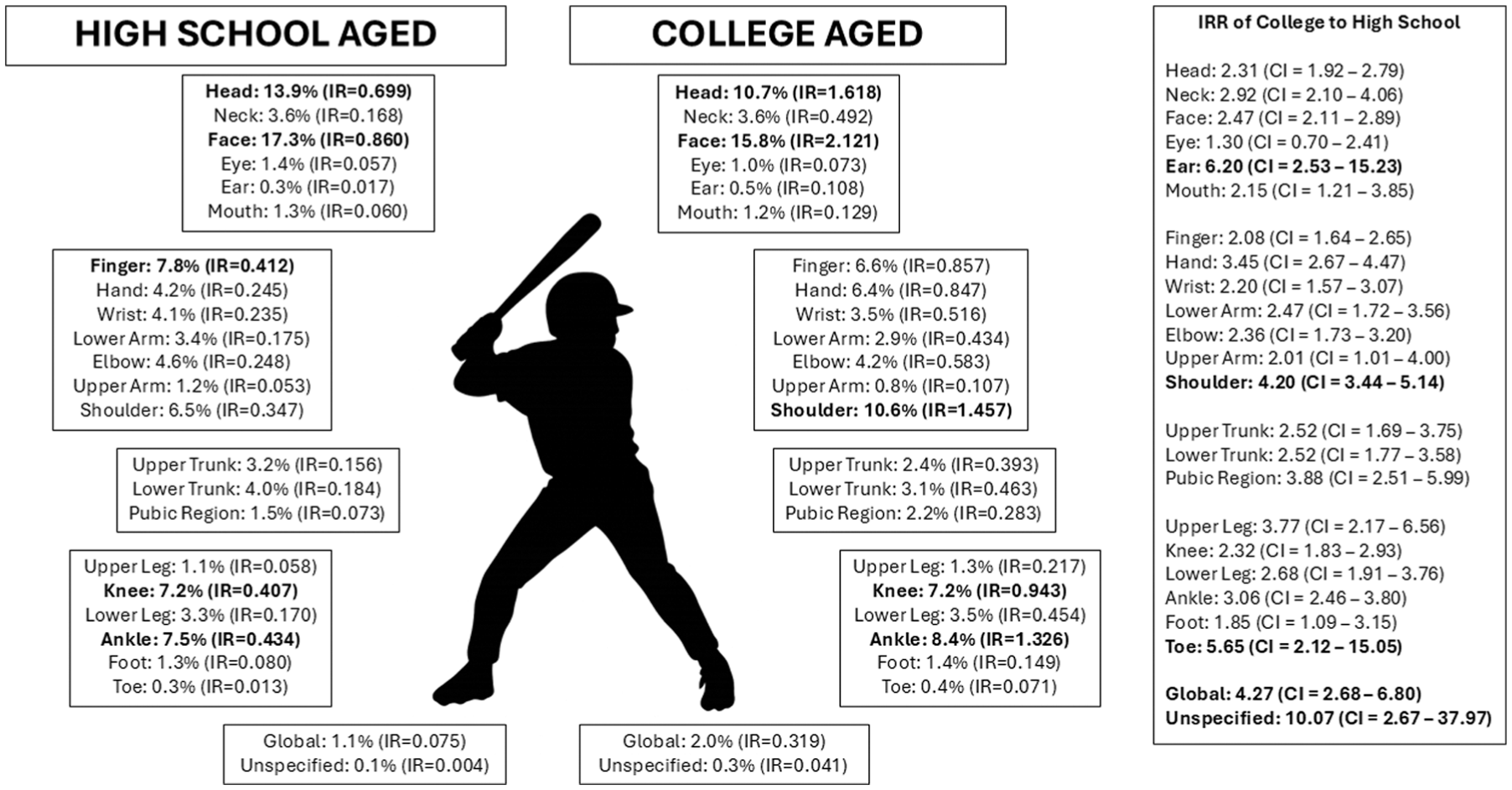
Incidence rates (IRs) among male baseball athletes evaluated in the emergency department, stratified by age group. For each anatomic site, values are presented as percentage of injuries within the cohort and incidence per 100 at-risk players. Bolded text indicates the top 5 injury sites by region. The right-side panel displays the IR ratio (IRR; college-aged vs high school–aged) for each anatomic site.
Although high school athletes represented 83% of ED visits for baseball-related injuries, IRs adjusted for at-risk population revealed consistently higher injury rates among college-aged athletes. Notably, college players had significantly elevated rates of injury to the face (IRR, 2.47; 95% CI, 2.11-2.89), shoulder (IRR, 4.20; 95% CI, 3.44-5.14), knee (IRR, 2.32; 95% CI, 1.83-2.93), ankle (IRR, 3.06; 95% CI, 2.46-3.80), and wrist (IRR, 2.20; 95% CI, 1.57-3.07) (Table 2). They also demonstrated higher rates of nearly all diagnoses, including lacerations (IRR, 3.55; 95% CI, 2.94-4.28), dislocations (IRR, 5.98; 95% CI, 4.62-7.74), and concussions (IRR, 2.30; 95% CI, 1.67-3.16).
Injury Characteristics and Population-Adjusted Incidence Rates by Age a

Percentages represent the proportion of all emergency department–treated injuries within each cohort (ie, category-specific national estimate divided by the total national estimate for that cohort: High School = 246,456; College = 51,465)
Disposition
Most baseball-related ED visits in both groups resulted in treatment and discharge. Within each cohort, 96.5% of high school–aged and 95.2% of college-aged athletes were treated and discharged (IR, 5.04 vs 13.33 per 100 at-risk players). High school–aged athletes experienced significantly lower rates of hospital admission (IRR, 0.29; 95% CI, 0.21-0.40) and leaving against medical advice (IRR, 0.22; 95% CI, 0.13-0.36). Overall, college-aged athletes were nearly 3 times more likely to be evaluated in the ED for a baseball-related injury than high school–aged athletes (IRR, 2.68; 95% CI, 2.65-2.70).
Discussion
The major findings in this national analysis of nearly 300,000 estimated baseball-related ED injuries from 2015 to 2024 demonstrated that college-aged players had almost a 3-fold higher incidence of ED-treated injuries than high school–aged players. College-aged male baseball athletes also exhibited elevated rates of injury across many body parts, particularly the face, shoulder, knee, ankle, and wrist, as well as higher rates of fracture, dislocation, laceration, and concussion. While most injuries were treated and discharged from the ED, college-aged players were >3 times more likely to require hospital admission or transfer than their high school peers.
These findings align with prior exposure-based surveillance data. A direct comparison utilizing both the High School Reporting Information Online system and the NCAA Injury Surveillance Program (ISP) by Wasserman et al 25 demonstrated higher injury rates in college-aged athletes than in high school–aged athletes (3.20 vs 0.98 per 1000 athlete-exposures). Other studies using these surveillance systems have similarly reported high rates of upper-extremity injury across competition levels.3,18 While our ED-based IRs (per 100 at-risk players) are not directly comparable with exposure-based metrics (per 1000 athlete-exposures), the magnitude and direction of the differences between age groups are consistent with the established pattern of higher injury rates at higher levels of competition. The injury patterns across body regions show that collegiate athletes experience higher rates of facial, shoulder, knee, ankle, and wrist injury. The elevated rates of these injuries in college athletes are likely driven by factors inherent to the collegiate environment, including faster pitches, more forceful base running and sliding, more frequent collisions, longer seasons, and greater cumulative exposure.3,5,19,25 Together, these factors may increase the likelihood of severe acute injuries that require ED care (such as fractures and dislocations), in contrast to the overuse injuries more commonly managed in athletic training rooms or outpatient clinics. Prior work directly comparing NEISS ED presentations with athletic trainer–based surveillance systems demonstrates systematic differences by care setting, with ED-treated injuries disproportionately including higher-acuity diagnoses (eg, fractures/dislocations) relative to athletic training settings, which capture a larger proportion of sprains/strains and injuries managed on-site. 6 Similar ED versus athletic trainer differences have been shown in sport-specific comparisons, including soccer and basketball, and in injury-specific comparisons, including ankle injuries.6,9,26 These findings suggest that collegiate programs may benefit from targeted preventive strategies, such as reinforcing safe sliding and base-running techniques and optimizing conditioning to reduce high-energy collisions.
Head and facial injuries were common in both age groups, but rates were significantly higher among college-aged athletes. Our findings are consistent with prior work. 12 Marar et al 12 reported that concussions in baseball frequently result from being hit by a pitch, a mechanism that also contributes to facial trauma. Lawson et al 10 similarly noted high proportions of facial injuries in youth baseball participants accounting for 33.5% of reported injuries. Given the high incidence and potential severity of facial and head injuries, particularly at the collegiate level, the use of enhanced facial protection, such as helmet face guards, warrants further consideration.
Regarding diagnosis patterns, fractures were the most prevalent injury overall, particularly involving the face, fingers, and upper arm. College-aged athletes also had higher rates of dislocation, concussion, and laceration. These findings are consistent with the expectation that ED-based samples disproportionately capture higher-acuity injuries compared with athletic trainer or clinic-based settings. Prior studies have shown that high-energy mechanisms, including collisions and ball contact, are common causes of severe injury in baseball. 2 Previous NEISS-based research has also demonstrated that ED-treated injuries such as ankle trauma are more likely to involve fractures, whereas sprains and strains are more frequently seen in other care settings. 26 The higher rate of concussions among college-aged athletes underscores the importance of robust concussion protocols that emphasize preseason education, early recognition, and diligent in-season monitoring, especially in collegiate programs where game speed and impact forces are greater.
With respect to disposition, college-aged baseball athletes had higher ED visit rates per at-risk population, but the proportion of patients treated and discharged was similar across age groups. Nonetheless, the higher incidence of admission and transfer among college-aged players suggests greater clinical severity and resource utilization in this cohort. Differences in care pathways may also contribute. Although organized collegiate programs commonly have athletic training coverage, the age-based cohort may include athletes outside NCAA settings, and thresholds for ED presentation may differ with decision-making autonomy and available on-site medical resources. Because NEISS does not capture prior athletic trainer evaluation or referral status, we could not evaluate how supervision or referral pathways influenced ED utilization or disposition. These patterns have implications for staffing, athletic training coverage, and emergency care planning at institutions with collegiate baseball programs, as well as for insurance and health policy considerations for young adult athletes.
The injury rates for both groups experienced declines in injury incidence in 2020, coinciding with the onset of the COVID-19 pandemic. Our results parallel prior reports documenting reductions in organized sports participation and sports-related ED visits during the lockdown period.11,17,23 As sporting activities resumed, injury rates returned toward prepandemic levels, highlighting the extent to which external factors influenced observed injury epidemiology.
Although many baseball injuries occur as acute events and may not be fully preventable, the observed injury distributions suggest opportunities for risk reduction and severity mitigation. The high frequency of head/face injuries in both cohorts supports continued emphasis on properly fitted protective equipment and consideration of additional facial protection where permitted, as well as rule enforcement and policies aimed at reducing dangerous contact. Consensus guidance also supports standardized concussion recognition and return-to-play pathways to reduce missed injuries and facilitate appropriate escalation of care. 7 The comparatively higher incidence of fractures and dislocations among college-aged athletes highlights the potential value of upper-extremity risk reduction efforts, such as shoulder-scapular strengthening and neuromuscular programs and evidence-informed throwing workload management, recognizing that optimal thresholds vary across settings.8,20 Finally, because this study captures ED-treated injuries, level-appropriate emergency action planning (eg, protocols for craniofacial trauma, fracture management, and expedited transfer when needed) may be particularly relevant for higher-acuity events that cannot be entirely prevented. 21
Limitations
This study is not without limitations. Only injuries that were evaluated in EDs were captured in NEISS. Injuries managed in athletic training rooms, urgent care centers, outpatient clinics, or not treated at all were not included, likely leading to underestimation of the true incidence of all baseball-related injuries, particularly minor and overuse conditions. NEISS uses a sample of approximately 100 US EDs to generate national estimates, so the data in this study were subject to sampling variability and potential over- or underrepresentation of specific injury types. The database contained limited contextual information, including mechanism of injury, player position, level of play, and whether the injury occurred during practice or competition, which restricted more granular risk factor analysis. Last, the age cutoffs used (14-18 vs 19-23 years) served as pragmatic proxies for high school versus collegiate participation because NEISS did not capture competition level. However, age did not perfectly map to level of play; for example, some 18-year-olds competed in college, and some 19-year-olds may still have been competing in high school (eg, delayed school entry or grade retention). In addition, injuries captured in these age ranges may reflect nonscholastic participation (eg, club, recreational, or professional play). This potential misclassification could dilute true between-level differences; therefore, findings should be interpreted as age-based comparisons and may be conservative with respect to differences attributable strictly to level of play.
Conclusion
Our study showed that between 2015 and 2024, college-aged baseball players had significantly higher IRs of ED-treated injuries than their high school–aged peers across most body regions and diagnoses. College-aged athletes faced elevated risks for more severe injuries requiring emergency care, including fractures, dislocations, and concussions, highlighting the need for preventive strategies tailored to the specific demands of higher competition levels.
Footnotes
Final revision submitted January 2, 2026; accepted January 26, 2026.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.