
Abstract
Background:
Few studies have reported the return-to-sports (RTS) rate in patients after augmentation of autologous anterior cruciate ligament reconstruction (ACLR) with the Ligament Augmentation and Reconstruction System (LARS).
Purpose/Hypothesis:
The purpose of this study was to compare postoperative outcomes in patients who underwent ACLR with single-bundle 4-strand hamstring autograft either without augmentation (HA-ACLR group) or with LARS augmentation (AUG-ACLR group). It was hypothesized that clinical outcomes and RTS rates would be better in the AUG-ACLR group at the 1-year follow-up, with similar outcomes in both cohorts by 2 years.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Patients who underwent ACLR between April 2014 and December 2017 were included in the current comparative study if they were skeletally mature and had 1- and 2-year follow-up outcomes; patients with concomitant meniscal surgery were also included. Included were 66 patients with AUG-ACLR (mean age, 26.8 years; 67% male) and 130 patients with HA-ACLR (mean age, 27.5 years; 61% male). Subjective outcome measures included the International Knee Documentation Committee Subjective Knee Evaluation Form, Knee injury and Osteoarthritis Outcome Score, Lysholm scale, Tegner activity scale, and the Noyes sports activity rating scale. Objective measures included knee laxity, maximal isokinetic knee flexion and extension strength, and the results of 4 functional hop tests.
Results:
There were no significant differences between the study groups in age, sex distribution, body mass index, time to surgery, or number of concurrent meniscal surgeries. At the 1-year follow-up, the AUG-ACLR group had a significantly higher Tegner score (P = .001) and rates of RTS (P = .029) and return to preinjury level of sport (P = .003) compared with the HA-ACLR group. At the 2-year follow-up, there were no differences in these measures between groups. There were no between-group differences in other subjective outcomes, knee laxity, or strength and hop test results at either postoperative time point. There were also no differences in rerupture rates or other complications between the groups.
Conclusion:
Patients with AUG-ACLR had higher 1-year postoperative Tegner scores and rates of RTS and preoperative sport level compared with the HA-ACLR group. The 2-year rerupture rate for the AUG-ACLR group was low, and no intra-articular inflammatory complications were noted.
Many patients desire a rapid return to activities and sports after anterior cruciate ligament (ACL) reconstruction (ACLR). This is now being utilized as a primary outcome measure in many studies. 4 However, less than two-thirds of patients return to their preinjury level of sports, and just over half return to competitive sports. 4,6 The inability to return to sports (RTS) is multifactorial, with outcomes influenced by both surgical and rehabilitation factors. 27
During the early graft-remodeling phase (5-9 weeks) after ACLR, there remain signs of inflammation within the knee, with the graft itself demonstrating hypocellular and hypovascular areas, reducing its strength and stiffness. 13,52 After 9 weeks, these hypocellular areas are no longer seen, and the graft is surrounded by a hypertrophic synovial layer. 52 Thus, the period between 5 and 9 weeks postoperatively represents a transitional stage and a time for potential graft stretching/failure. 58 For this reason primarily, patients are often informed to avoid impact and pivoting/cutting activities for at least 3 to 4 months after surgery. 43
Early aggressive rehabilitation after ACLR has demonstrated varied outcomes. Randomized controlled trials have shown no or only modest improvement with accelerated rehabilitation. 11,14,24 Others have suggested early aggressive rehabilitation to have a negative effect on final graft laxity. 21,34,41 The fear of the latter leads to surgeons, rehabilitators, and patients being guarded and cautious in their rehabilitation approach. Nevertheless, early accelerated rehabilitation may improve graft healing and neuromuscular control of the limb and accelerate the restoration of knee range of motion and muscle strength. 45,47 In combination, these may facilitate an earlier return of knee function and potentially participation in sports.
Augmentation of ACLR autografts with synthetic material is a recognized technique proposed to facilitate and accelerate rehabilitation. 18,19,20,32 Fears regarding noninfective synovitis with effusion were noted with earlier generations of intra-articular synthetic devices, but new generations, such as the Ligament Augmentation and Reconstruction System (LARS; Surgical Implants and Devices), have shown low rates of 0.2%. 35 This is in contrast to earlier devices that had high failure and synovitis rates and an increased risk of early-onset osteoarthritis. 10,33
The aim of the current study was to compare patient outcomes and the ability to RTS after a single-bundle 4-strand hamstring autograft ACLR either without augmentation (HA-ACLR group) or with LARS augmentation (AUG-ACLR group). We hypothesized that clinical outcomes and RTS rates would be better in the AUG-ACLR group at 1 year after surgery, with similar clinical outcomes in both groups by 2 years. We also hypothesized that there would be an absence of complications that may be more commonly reported with synthetic intra-articular augmentation and accelerated RTS (graft laxity/failure and synovitis).
Methods
Patients
A total of 212 patients who underwent ACLR (73 patients with AUG-ACLR, 139 patients with HA-ACLR) between April 2014 and December 2017 were recruited into a prospective research program. All patients with AUG-ACLR underwent surgery by the same surgeon (P.T.A.), with patients with HA-ACLR undergoing surgery by 1 of 3 different surgeons using the same technique. Inclusion criteria were ACL rupture in a skeletally mature patient. Patients were excluded if there was a concurrent posterior cruciate or collateral ligament injury requiring surgical intervention. Concurrent meniscal surgery cases were included. Ethical approval was obtained by the relevant hospital human research ethics committee, and all patients provided consent for participation.
In total, there were 73 patients with AUG-ACLR who underwent surgery during the study period. Five patients were lost to follow-up between the 1- and 2-year follow-ups (3 had a long traveling distance for face-to-face follow-up, 1 was unable to comply with strength/functional testing because of an unrelated health issue, and 1 experienced a patellar fracture at 23 months postoperatively due to an unrelated trauma). One patient had a rerupture at 18 months postoperatively, while 1 patient experienced a contralateral ACL rupture at 14 months postoperatively. Therefore, 66 patients with AUG-ACLR were included in the current study for data analysis.
In total, there were 139 patients with HA-ACLR during the study period. Nine patients were lost to follow-up between the 1- and 2-year follow-ups, including 3 patients who had ipsilateral reruptures (at 13, 13, and 17 months postoperatively) and 2 patients who had contralateral ACL ruptures (at 12 and 16 months postoperatively). Another 4 patients did not complete outcomes at 1 and/or 2 years and were excluded from the current analysis, leaving a total of 130 patients with HA-ACLR in the current data analysis.
All patients underwent ACLR using a single-bundle 4-strand hamstring reconstruction using both semitendinosus and gracilis tendon harvested from the ipsilateral limb. Fixation was achieved using a fixed-loop suspensory device for the femoral fixation and interference screw for the tibial fixation. Patients undergoing LARS augmentation had the addition of a LARS (product code 104.133; LARS ACL reinforcement) to the construct. The exact surgical technique for LARS-augmented ACLR has been previously published by Ebert and Annear. 19
Rehabilitation was performed by the patients’ preferred practitioner. All patients were advised to engage in a structured rehabilitation program with a graded return to activities and sports. A time-based approach was avoided, and a task-based approach was advised. RTS was permitted once the patient’s practitioner felt it was suitable. However, broadly speaking, patients should have no joint effusion, quadriceps and hamstring strength within 90% of the contralateral limb, and no subjective sensation of instability.
Clinical Assessment
Clinical subjective and objective assessments were conducted by a research senior physical therapist (J.R.E.) who was not involved in any patient’s rehabilitation.
A number of patient-reported outcome measures (PROMs) were completed at 1 and 2 years postoperatively. These included the International Knee Documentation Committee (IKDC) Subjective Knee Evaluation Form, 26 Knee injury and Osteoarthritis Outcome Score (KOOS), 46 Lysholm scale, 31 Tegner activity scale, 48 and Noyes sports activity rating scale. 38 Furthermore, a global rating of change scale was employed to evaluate the patient’s perceived status compared with that before surgery, with scores ranging from –5 (very much worse) to 0 (about the same) to 5 (completely recovered).
Objective outcome measures included anterior tibial translation as measured using a KT-1000 arthrometer (MEDmetric) during a maximal manual test; the difference between the operated and nonoperated knees was obtained. 42 Patients also underwent a previously validated battery of 4 hop tests in the following order: (1) single hop for distance, (2) 6-m timed hop, (3) triple hop for distance, and (4) triple crossover hop for distance. 44 Finally, peak concentric knee extension (quadriceps) and flexion (hamstring) strength were measured at a single isokinetic angular velocity of 90 deg/s using an isokinetic dynamometer (Isosport). To avoid fatigue, patients were given as much time as they wanted between hop and strength trials; this time was not standardized but was based on the individual patient’s readiness to proceed.
Statistical Analysis
The mean ± standard deviation (range) of all measures (operated and nonoperated limbs) was calculated at 1 and 2 years postoperatively. Analysis of variance was employed to investigate differences in pertinent patient and surgical characteristics between the 2 surgical groups, as well as clinical differences over time (1 and 2 years) between groups. Other categorical data were analyzed using the chi-square test. Limb symmetry indices (LSIs) were calculated for all hop and strength tests, further categorized by the number and percentage of patients with LSIs <90% and ≥90%. Normality of data was tested using the Shapiro-Wilk test. The t test was employed for parametric data, and the chi-square test was used for nonparametric data.
The KT-1000 arthrometer laxity measurements were categorized based on the side-to-side difference as normal (<3 mm), nearly normal (3-5 mm), abnormal (6-10 mm), and severely abnormal (>10 mm). 36 The Noyes activity rating scale was employed to present the number and percentage of patients participating in level 1 (4-7 d/wk) or level 2 (1-3 d/wk) activities, including jumping, hard pivoting, cutting, running, twisting, and/or turning sports. Finally, the number and type of surgical complications, postoperative adverse events, reoperations, and reruptures (ipsilateral and/or contralateral ACL ruptures) were evaluated between groups. Statistical analysis was performed using SPSS software (Version 23.0; IBM Corp). Statistical significance was determined at P < .05.
Results
Patients
No significant differences were observed between the AUG-ACLR and HA-ACLR groups in age, sex distribution, body mass index, time to surgery from injury, surgery on the dominant leg, prior contralateral ACLR, and the rate of concomitant meniscal surgery (Table 1).
Comparison of Patient Characteristics Between the AUG-ACLR and HA-ACLR Groups a

a Data are reported as mean ± SD or No. of patients (% within group). ACLR, anterior cruciate ligament reconstruction; AUG, augmented; BMI, body mass index; HA, hamstrings alone; MACI, matrix-induced autologous chondrocyte implantation.
Subjective Assessment
At the 1-year follow-up, there was a significantly better Tegner score in the AUG-ACLR group compared with the HA-ACLR group (P = .001) (Table 2). At the 2-year follow-up, a significantly better KOOS–Activities of Daily Living score was reported in the HA-ACLR group (P = .007) (Table 2).
Comparison of Patient-Reported Outcome Measures at 1- and 2-Year Follow-ups a

a Data are reported as mean ± SD (95% CI). Bolded P values indicate a statistically significant difference between groups (P < .05). ACLR, anterior cruciate ligament reconstruction; ADL, Activities of Daily Living; AUG, augmented; GRC, global rating of change; HA, hamstrings alone; IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; QOL, Quality of Life; Sport/Rec, Sport and Recreation.
Objective Assessment
There were no significant between-group differences observed in KT-1000 side-to-side laxity and no differences in the percentage of patients with normal laxity (Table 3). There were also no significant differences between the AUG-ACLR and HA-ACLR groups in strength or hop test LSIs at either 1 or 2 years postoperatively (Table 4).
Comparison of KT-1000 Arthrometer Laxity at 1- and 2-Year Follow-ups a

a Data are reported as mean ± SD (95% CI) or No. of patients (% within group). ACLR, anterior cruciate ligament reconstruction; AUG, augmented; HA, hamstrings alone; SSD, side-to-side difference.
Comparison of Functional Hop Tests and Peak Isokinetic Quadriceps and Hamstring Strength at 1- and 2-Year Follow-ups a
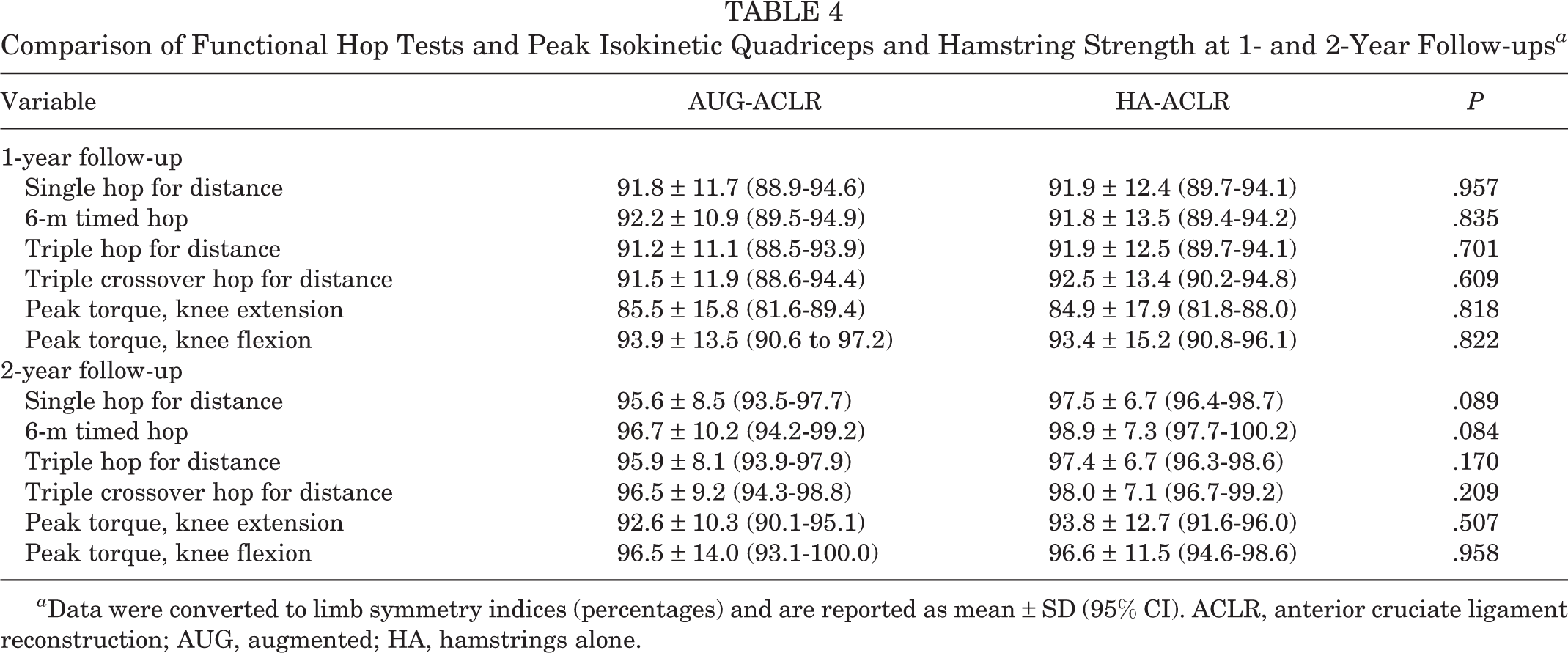
a Data were converted to limb symmetry indices (percentages) and are reported as mean ± SD (95% CI). ACLR, anterior cruciate ligament reconstruction; AUG, augmented; HA, hamstrings alone.
Return to Sports
A significantly greater proportion of patients with AUG-ACLR achieved a return to Noyes level 1 or 2 sports (81.8%) at 1 year compared with the HA-ACLR group (66.2%; P = .029) (Table 5). No between-group differences were observed by 2 years (Table 5).
Comparison of Sport Participation Preoperatively and at 1- and 2-Year Follow-ups a

a Data are reported as No. of patients (% within group). Bolded P value indicates a statistically significant difference between groups (P < .05). ACLR, anterior cruciate ligament reconstruction; AUG, augmented; HA, hamstrings alone.
b Defined as participating in Noyes level 1 or 2 sports.
The return to preinjury level of sports was 51.5% in the AUG-ACLR group and 28.5% in the HA-ACLR group at 1 year (P = .003). At 2 years, this difference was no longer observed (60.6% vs 49.2%; P = .173). There was no statistical change in the percentage of patients who had returned to their preinjury level of sports between 1 and 2 years for the AUG-ACLR group (P = .079), although this had significantly improved for the HA-ACLR group (P = .001).
Complications, Reoperations, and Failures
For the 66 patients who underwent AUG-ACLR, there was 1 early wound infection (treated with antibiotics) and 3 patients who required secondary arthroscopy (1 partial meniscectomy, 1 meniscal repair, 1 excision of cyclops lesion). For the HA-ACLR group, a similar complication rate was observed, with 1 superficial wound infection (treated with antibiotics) and 6 patients requiring secondary arthroscopy (2 partial meniscectomies, 1 meniscal repair, 3 excisions of cyclops lesions).
Patients who experienced an ipsilateral rerupture or contralateral ACL tear between 1 and 2 years were omitted from the current analysis, given they could not be appropriately assessed at 2 years after their primary ACLR. Overall, in the AUG-ACLR group, 1 patient sustained an ipsilateral rerupture at 18 months postoperatively, while 1 patient had a contralateral ACL rupture at 14 months postoperatively (overall ipsilateral/contralateral tear rate, 3.0%). In the HA-ACLR group, 3 patients had ipsilateral reruptures at 13, 13, and 17 months postoperatively, while 2 patients had contralateral ACL ruptures at 12 and 16 months postoperatively (overall ipsilateral/contralateral tear rate, 3.8%).
Discussion
The most important findings from the current study were that the AUG-ACLR group demonstrated significantly better Tegner score and RTS rates by the 1-year follow-up, without any apparent complications, including excessive side-to-side graft laxity or reinjuries (ipsilateral retears or contralateral tears). Despite these findings, no other differences between the groups in PROMs (except KOOS-ADL) or objective LSI scores (strength and functional hop capacity) were observed at 1 or 2 years postoperatively.
ACLR augmentation has been utilized for some time with reproducible results. 53 In vivo studies have shown that LARS may permit tissue ingrowth, and this property can be utilized when it is used as an augmentation to biological ACLR, albeit unlikely as an ACL replacement on its own. 49,54,55 The LARS is made from polyethylene terephthalate, which is also a main component of the EndoButton (Smith & Nephew) device. Ligament augmentation with a synthetic graft has been used with good effect for medial collateral or posteromedial corner injuries of the knee, 22,30 lateral ligaments of the ankle, 15,51 and the ulnar collateral ligament of the thumb. 40
In vitro studies have shown that suture tape augmentation of a biological ACL graft leads to significantly reduced elongation at higher loads and increased ultimate strength. 37 It has also been found that at lower loads, the suture tape does not shield the graft from tension, as a certain amount of graft elongation is required before suture tape sharing loads. 7,17 We believe that if stress shielding of the biological graft by the synthetic augmentation were an issue, we would have seen a much higher early failure rate. The reported failure (retear) rate of 2.0% in the current study is comparable with the rates in other similar studies. 2,12,20 First-generation synthetic augmentations used intra-articularly did cause concerns regarding noninfective synovitis, persistent effusion, early failure, and potentially early degeneration of chondral surfaces. 10,33 We found none of these issues within the study population. Key points made during surgery included using a narrow LARS and placing it posteriorly in the graft construct. We believe that by using these simple maneuvers, we were able to allow the synthetic material to synovialize and prevent intra-articular issues seen in previous generations of synthetic ligaments.
RTS after ACLR is multifactorial, and studies have used a variety of markers to ascertain when a patient is ready to RTS. These include muscle strength or thigh circumference; knee examination findings; PROMs; and more recently, single-leg hop tests. 9 Many of these factors have been refuted. 39,56 The current study demonstrated that the AUG-ACLR group had improved Tegner scores, return to preinjury level of sports, and return to Noyes level 1 or 2 sports at the 1-year follow-up compared with the HA-ACLR cohort. Patients with ACLR who do not RTS at 1 year only have a 41% chance of returning to their preinjury sporting level by 2 years. 5 The 2-year return to preinjury sports rate of 61% in the AUG-ACLR cohort in the current study is at the higher end of comparative study results in modern literature, which has revealed a return to preinjury level of sports rate of 42% to 68%. 1,6,8,16,23,28
The current study did not find a substantial increase in this rate between 1 and 2 years, suggesting that these patients’ sporting recovery returned earlier, with earlier RTS, and fewer patients needed more than a year to RTS. This is reinforced by the fact that the HA-ACLR group did statistically improve in their return to preinjury level of sports between the 1-year and 2-year follow-ups, showing there was still improvement needed after the first year. Psychological factors and the perceived readiness to RTS play an important role. 3,29,50,57 The patients who underwent AUG-ACLR were generally counseled and aware that the synthetic component of the graft may permit faster rehabilitation. This counseling could allow for a greater amount of faith in the surgical construct, which could transfer to increased motivation in rehabilitation and a subsequent increased preparedness for RTS. However, all patients underwent supervised physical therapy and were deemed ready to RTS in conjunction with their individual physical therapist.
Falconer et al 20 established that double-bundle hamstring ACLR using autologous hamstrings and LARS augmentation allowed accelerated rehabilitation without compromising graft laxity up to 2 years after surgery. The benefits included a faster return to activities of daily living and low-level sporting activities. The overall result led to only 7% of patients having a side-to-side difference >3 mm at 2 years. 20 Bodendorfer et al 12 conducted a similar comparative cohort study to the current study, assessing the differences between single-bundle 4-strand hamstring ACLR with or without suture augmentation using the InternalBrace (Arthrex). They reported outcomes in 30 augmented ACLRs and a matched cohort of 30 hamstring-only ACLRs at 2 years and demonstrated that having a suture-augmented construct predicted a greater improvement in IKDC scores and KOOS Sport and Recreation and Quality of Life subscores, among other outcomes. Furthermore, a faster return to preinjury level of sport and a higher percentage of patients achieving preinjury levels of sport were reported, 12 similar to the results of the current study. Furthermore, Hamido et al 25 augmented undersized single-bundle 4-strand hamstring grafts with LARS in an effort to bulk up the diameter of their reconstruction. When compared with a hamstring-only ACLR, they had a reduced side-to-side laxity difference that was significant at 2 years, with improved functional scores at 5 years. 25
We accept there are limitations to the current study. First, it was nonrandomized, and while the groups were similar in characteristics, surgical history, and preinjury sporting capacity, it was a comparison of a single surgeon’s patients with AUG-ACLR to a group of patients undergoing HA-ACLR undertaken by 3 different surgeons. We accept there could be minor technical differences that could lead to variation in outcome. However, it is acknowledged that it is likely that by 1 year many of these objective scores would have improved, and it is possible that if these objectives measures were undertaken earlier (such as 6 months), then differences may have been observed.
A second limitation is that there were no baseline PROMs from which to assess our cohort. Baseline data would allow us to more robustly assess selection bias and add more meaning to the comparative results. Third, there may be an unknown psychological benefit for patients that an augmented LARS procedure may have. That is, many patients and their rehabilitation practitioners may foresee this as an avenue for accelerated rehabilitation, which may enhance physical capacity and confidence toward returning to activities and improving psychological readiness to RTS. This factor cannot be assessed fully unless the patient, therapist, and follow-up assessor are blinded to the surgical procedure in a more structured randomized controlled trial. Finally, we accept that rehabilitation may be an important factor contributing toward objective scores and RTS; this was not standardized across patients, and no standardized RTS testing battery was administered across patients. Rather, this was at the discretion of the patient’s individual rehabilitation practitioner, and patients were rehabilitated via a modern task-based approach. We also accept the inevitable cost attached to the addition of augmentation to an autograft construct. In order to make this standard practice, it should be cost-effective, and we have not performed this analysis in this study.
Conclusion
This study has shown that the AUG-ACLR procedure permitted a significantly better Tegner score and RTS rate by the 1-year follow-up compared with an HA-ACLR procedure. These outcomes were observed without increased complication, reoperation, and/or reinjury rates and without increased side-to-side laxity at the 1- and 2-year follow-ups. An autologous augmented graft construct may utilize the best of both graft types with early strength, to limit stretching/failure, with a longer-term biologically stable construct. A more robust randomized study with early postoperative assessment time points could ascertain the true benefits of such an augmented procedure.
Footnotes
Final revision submitted May 2, 2021; accepted June 8, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: This research was supported by independent funding grants provided to J.R.E. by Corin and the Hollywood Private Hospital Research Foundation (RF070). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Hollywood Private Hospital Human Research Ethics Committee (HPH382).