
Abstract
Background:
Anterior cruciate ligament (ACL) reconstruction has been the gold standard for primary ACL rupture since the 1990s. In the past decade, ACL repair has received renewed attention and increased research.
Purpose:
To compare the clinical outcomes of modern augmented ACL repair versus autograft reconstruction for ACL ruptures.
Study Design:
Systematic review; Level of evidence, 3.
Methods:
A search of the PubMed, EMBASE, Scopus, Web of Science, and the Cochrane Library databases was conducted for prospective or retrospective comparative studies published between January 1, 2010, and January 3, 2023, with a minimum 2-year follow-up. Two independent reviewers performed data extraction and methodological quality assessment. Sensitivity analysis was performed to maintain the stability of results.
Results:
Nine studies were included (minimum follow-up period, 24-60 months). The total sample size was 833 patients (augmented repair group: 358 patients; autograft ACL reconstruction group: 475 patients). There were 4 randomized controlled trials (level 1), 1 prospective comparative study (level 2), 2 retrospective comparative studies (level 3), and 2 case-control studies (level 3). The augmented ACL repair group attained significantly higher Lysholm score (weighted mean difference [WMD] = 1.57; 95% confidence interval [CI], 0.14-3.01; P = .03) and hamstring strength (WMD = 36.69; 95% CI, 29.07-44.31; P < .01) but had higher rates of hardware removal (odds ratio [OR] = 6.30; 95% CI, 2.44-16.23; P = .0001), reoperation (OR = 1.87; 95% CI, 1.33-2.62; P = .0003), and failure (OR = 1.58; 95% CI, 1.03-2.43; P = .0003) compared with the autograft ACL reconstruction group. No significant differences were observed between the repair and reconstruction groups regarding postoperative International Knee Documentation Committee scores, Tegner scores, knee laxity, satisfaction, ACL revisions, complications, and reoperation rather than revision.
Conclusion:
Augmented ACL repair was associated with higher rates of reoperation, hardware removal, and failure compared with autograft ACL reconstruction in studies with minimum 2-year follow-up data. However, augmented ACL repair had higher Lysholm scores and hamstring strength versus autograft ACL reconstruction.
Keywords
Anterior cruciate ligament (ACL) injury is a potentially disabling knee injury, affecting approximately 85 per 10,000 people aged between 16 and 39 years. 11 Primary open ACL repair was the standard surgical technique for ACL ruptures in the 1970s and 1980s. Although early results were encouraging,16,32 poor results emerged at long-term follow-up, 24 including persistent laxity, pain, stiffness, 16 and high failure rate.14,15,25 In contrast, ACL reconstruction in the same period had more reliable mid- and long-term clinical results than ACL repair.18,52 As a result, open ACL repair was gradually replaced by ACL reconstruction in the early 1990s, and ACL reconstruction became the gold standard for primary ACL rupture. 24
Although ACL reconstruction has shown more reliable long-term efficacy, limitations of the procedure, such as harvest complications and poor clinical outcomes after revision surgery, have also been reported.7,30 In the past decade, new techniques in ACL repair and augmentation have been described, with advantages such as less invasiveness compared with ACL reconstruction, lack of harvest site morbidity, and earlier restoration of function,9,47 thus bringing this surgical method back into the public view. 24 At short- to midterm follow-up, modern ACL repair has been found to have clinical outcomes that are comparative to or better than those of ACL reconstruction.1,12,35,36,42,47 However, whether the clinical success of primary ACL repair can be sustained at longer follow-up is still controversial.33,38
A variety of arthroscopic ACL repair techniques have emerged. 19 Some techniques that have gained attention are suture anchor repair (SAR), 1 suture augmentation repair, repair with dynamic intraligamentary stabilization (DIS), 13 bridge-enhanced ACL repair (BEAR), 36 and internal brace ligament augmentation (IBLA). 45 Each technique requires specific patient selection and indication such as tear type, age, and tissue quality. 24 Previous systematic evaluations have demonstrated improved clinical outcomes with ACL enhanced repair. In 2019, Ahmad et al 2 conducted an analysis of 23 articles on DIS and concluded that ACL repair could be an effective treatment for acute proximal ACL tears. Similarly, van der List et al 49 conducted a systematic evaluation involving 1101 patients and found that various ACL augmentation repair techniques were safe, with failure rates ranging from 7% to 11%, and yielded favorable knee functional outcome scores.
Recent studies have reported varying findings regarding the outcomes of arthroscopic ACL repair compared with ACL reconstruction, with some studies indicating similar outcomes and others suggesting better or worse results in terms of mixed objective and patient-reported outcomes.1,21,27,29,39,50,53 It is widely acknowledged in the academic community that this variability in outcomes may be attributed to the insufficient duration of follow-up.24,39,46,49 In recent meta-analyses, most of the included studies had ≤2 years of follow-up, and almost no study reached 5 years of follow-up. Short-term results may affect the accuracy of the overall effect of the meta-analysis, for adverse events may not appear until long-term follow-up. Several recent randomized controlled trails have renewed their outcomes to 5-year follow-up findings.17,22
The purpose of this systematic review and meta-analysis was to compare the clinical outcomes between modern augmented ACL repair and autograft ACL reconstruction. To avoid being affected by short-term (<2-year postoperative) results, we included only studies with at least 2-years of follow-up.
Methods
Literature Search
This study was conducted and reported according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement, 43 and the study protocol was registered on the PROSPERO database (CRD42022320640). Two independent researchers (Y.R. and C.Z.) searched for relevant English-language studies published between January 1, 2010, and January 3, 2023, in the following databases: PubMed, the Cochrane Library, Scopus, EMBASE, and Web of Science. Investigators used combinations of Medical Subject Headings and search terms such as “anterior cruciate ligament,”“ACL repair,”“anterior cruciate ligament reconstruction,”“ACL reconstruction,”“augmentation,”“reinforcement,”“suture,”“tape,”“internal brace,”“dynamic intraligamentary stabilization,” and “bridge enhanced.” The detailed search strategy is available separately as supplemental material.
Inclusion and Exclusion Criteria
Articles were included if they met the following inclusion criteria: (1) written in English, (2) study patients had a confirmed diagnosis of ACL rupture, (3) clinical studies comparing primary augmented ACL repair with ACL reconstruction with tendon autograft, and (4) studies had at least 2 years of follow-up data. When there were multiple publications on the same study population or if the overlapping of a patient cohort was found, studies based on the most complete outcomes and the longest follow-up were included. Also, because ACL repair with suture augmentation was first described in 2015, 4 we included studies published only after the year 2010. The exclusion criteria were studies with (1) inadequate or unavailable data, (2) presence of multiple ligament injuries or knee dislocations, (3) presence of concomitant lesions that affected rehabilitation, (4) presence of previous knee injuries on either the injured or contralateral knee, (5) presence of ACL repair without augmentation or ACL reconstruction with artificial ligament, (6) long-term follow-up of historical studies or case series (level 4 evidence), and (7) studies published before 2010.
Data Extraction
Data from the included studies were abstracted by 2 authors (J.J. and C.Z.) independently. Discrepancies were resolved by consensus, referring back to the original article, in consultation with a third reviewer (Q.M.). Data extracted from each study included the following: (1) study characteristics (primary author, year, country, study design, level of evidence, sample size); (2) patient characteristics (age, sex, time from injury to surgery, follow-up period, rupture location, autograft type); (3) primary outcomes (patient-reported outcomes including the International Knee Documentation Committee [IKDC] score, 37 Lysholm score, 31 Tegner score, 8 and patient satisfaction; clinical knee stability measures including anteroposterior knee laxity defined as mean difference in anterior tibial translation [ΔATT] between the injured and contralateral knees and positive Lachman test [grades 2 and 3]); and (4) secondary outcomes (adverse events including failure [a combination of subjective instability, findings at physical examination, and/or graft rupture], reoperation [all ipsilateral surgeries during follow-up, including revision ACL surgeries], reoperation other than revision [additional surgical interventions for ipsilateral knee disorders other than ACL retears], hardware removal [removal of the internal fixation devices], revision ACL surgery [repeated ACL reconstructions or conversion to ACL reconstruction due to rerupture or adverse events] and complications), and functional outcomes including muscle strength and hop tests.
Quality Assessment
The risk of bias of the included studies was assessed by 2 authors (Y.R. and J.W.) independently. The Cochrane Collaboration tool was used to assess the risk of bias of enrolled randomized controlled trials (RCTs), 20 and the risk of bias of the included cohort and case-control studies was evaluated with the Methodological Index for Non-Randomized Studies (MINORS) criteria. 44 A third evaluator (Q.M.) made the final decision in case of any disagreements.
Statistical Analysis
All statistical analyses were performed with Review Manager Version 5.4.1 (The Cochrane Collaboration, Software Update). Weighted mean difference (WMD) and pooled odds ratios (ORs) with 95% confidence intervals (CIs) were calculated to analyze the outcomes. A P value <.05 was considered to be statistically significant. Heterogeneity was measured by the Cochran chi square-based Q test and I2 statistic for all eligible studies. When P was >.10 and I2 was <50%, a fixed-effect model was applied; otherwise, a random-effects model was used. If there was significant heterogeneity, subgroup analysis and sensitivity analysis was conducted to explore the sources of high heterogeneity. Sensitivity analysis was performed to maintain the stability of results. The Egger test was applied to assess publication bias.
Results
Results of Literature Search
A total of 11,173 articles were initially retrieved from the database searches. After 5250 duplicates were removed, the titles and abstracts of 5923 remaining articles were screened, and 5893 articles were removed according to the inclusion and exclusion criteria. The remaining full texts of 30 articles were screened, and, ultimately, 9 articles were included in the meta-analysis ¶ : 4 RCTs,17,22,28,35 1 prospective cohort study, 36 2 retrospective cohort studies,23,26 and 2 case-control studies.1,6 The literature search process is shown in Figure 1.

PRISMA flowchart of literature retrieval and inclusion. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Baseline Data
Detailed baseline information for the 9 articles is summarized in Table 1. ¶ There were 833 patients including 358 who underwent ACL repair and 475 who underwent ACL reconstruction. The mean age of patients ranged from 17 to 35 years, and the percentage of male patients ranged from 30% to 81%. The mean time from injury to surgery ranged from 13 to 336 days, and the minimum follow-up period ranged from 24 to 60 months.
Characteristics of Included Studies a

Dashes indicate data not reported. ACL, anterior cruciate ligament; BPTB, bone-patellar tendon-bone; C-C, case-control; F, female; HT, hamstring tendon; LOE, level of evidence; M, male; PCS, prospective cohort study; PT, patellar tendon; QT, quadriceps tendon; RCS, retrospective cohort study; RCT, randomized controlled trial; R Comp, retrospective comparative study; Recon, reconstruction; SG, semitendinosus-gracilis tendon; ST, semitendinosus tendon.
Data are shown as mean ± SD and/or (range).
Data are shown as mean ± SD, (range), and/or minimum.
Measured as percentage length of tibial remnant.
The ACL rupture locations included proximal, central, and distal. Semitendinosus-gracilis tendon, hamstring tendon, patellar tendon, and quadriceps tendon were used as autograft for ACL reconstruction. The ACL repair techniques included primary SAR, primary ACL suture repair with DIS, and BEAR. The primary SAR was performed using 1 suture anchor to reattach the ACL remnant back to the femoral footprint. The DIS was performed by introducing an intraligamentary braid with cortical button fixation on the femoral side and an additional elastic link (a spring-in-screw mechanism) on the tibial side after the remaining threads in the ACL stump were tensioned and the tibial stump was repositioned to the femoral footprint. The BEAR procedure was performed by combining a BEAR scaffold saturated with 5 to 10 mL of autologous blood with suture repair of the ligament to bridge the gap between the ends of the torn ligament.
Quality Assessment
The quality of the included RCTs as assessed using Cochrane risk-of-bias tool are summarized and visualized in Figure 2, 20 and the quality of the included cohort and case-control studies as evaluated by MINORS criteria is shown in Table 2. 44 All included studies were of high quality.

Results of Cochrane risk-of-bias assessment for the included RCTs. (A) Graph of overall risk of bias. (B) Risk-of-bias summary by study. RCTs, randomized controlled trials.
Quality Assessment of the Non-RCT Studies Using MINORS Criteria a

C-C, case-control; LOE, level of evidence; MINORS, Methodological Index for Non-Randomized Studies; PCS, prospective cohort study; RCS, retrospective cohort study; RCT, randomized controlled trial.
Only the part of the MINORS criteria for noncomparative studies (ie, the first 8 questions) was used. Items: 1, a clearly stated aim; 2, inclusion of consecutive patients; 3, prospective collection of data; 4, end points appropriate to the aim of the study; 5, unbiased assessment of the study end point; 6, follow-up period appropriate to the aim of the study; 7, loss to follow-up <5%; and 8, prospective calculation of the study size.
Item scoring: 0, not reported; 1, reported but inadequate; and 2, reported and adequate. Maximum score is 16.
Meta-Analysis of Primary Outcomes: Patient-Reported Outcomes and Knee Laxity
A total of 5 included studies compared postoperative IKDC subjective score between ACL repair and reconstruction.17,22,26,35,36 The group difference in IKDC subjective score was not statistically significant, with low heterogeneity (WMD = 1.44; 95% CI, -0.20 to 3.09; I2 = 30%; P = .09) (Figure 3A). Two of the studies compared the postoperative Lysholm score and found a statistically significantly higher score in the repair group versus the reconstruction group, with no heterogeneity (WMD = 1.57; 95% CI, 0.14-3.01; I2 = 0%; P = .03) (Figure 3B).17,26
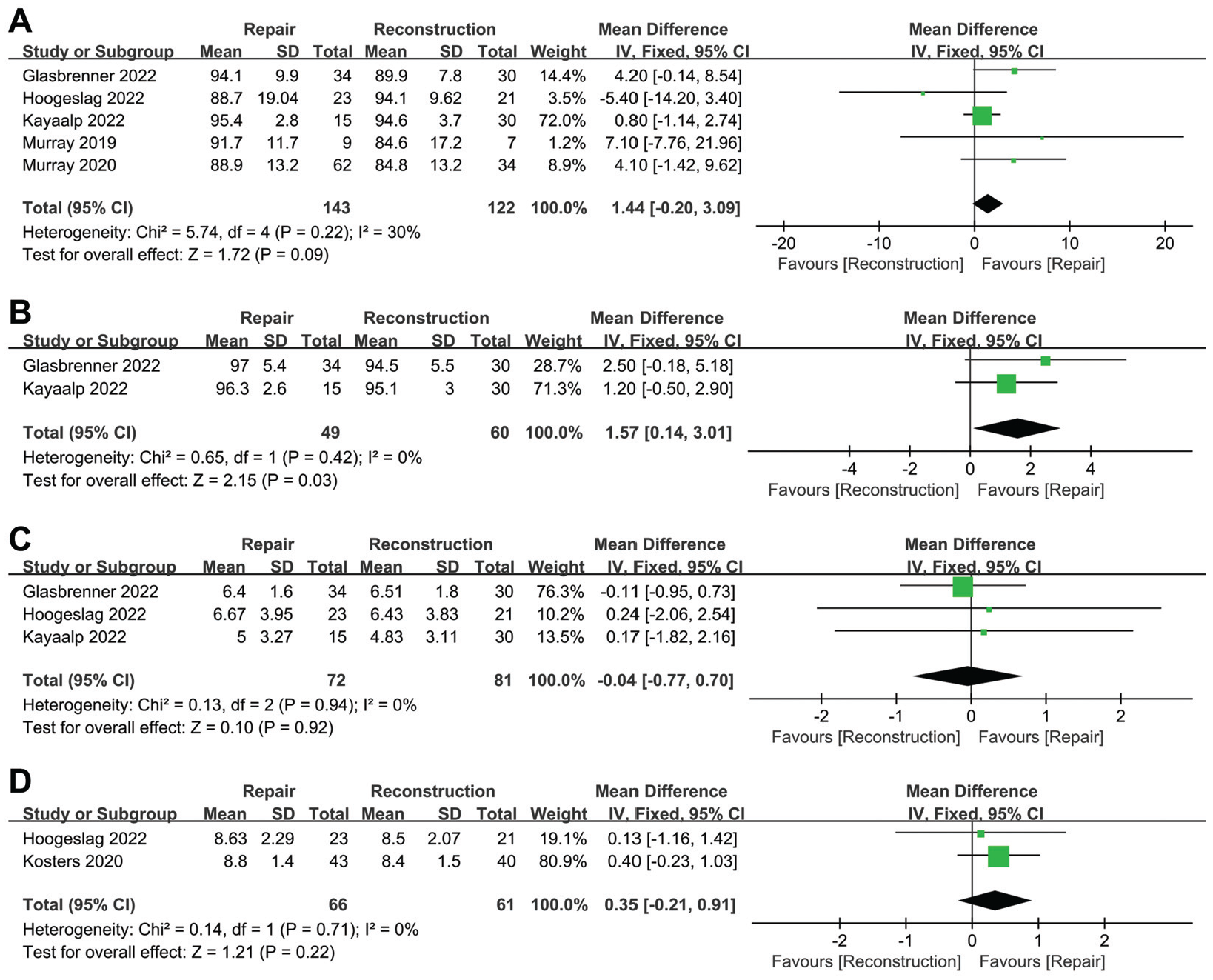
Results of meta-analysis of patient-reported outcomes. (A) IKDC score, (B) Lysholm score, (C) Tegner score, and (D) satisfaction. CI, confidence interval; df, degrees of freedom; IKDC, International Knee Documentation Committee; IV, inverse variance.
There were 3 studies comparing postoperative Tegner score between the repair and reconstruction groups,17,22,26 with no significant difference between the 2 groups (WMD = -0.04; 95% CI, -0.77 to 0.70; I2 = 0%; P = .92) (Figure 3C). Two studies reported patient satisfaction (range, 0-10; 0 representing unsatisfied and 10 representing very satisfied),22,28 with no significant difference between the repair and reconstruction groups (WMD = 0.35; 95% CI, -0.21 to 0.91; I2 = 0%; P = .22) (Figure 3D).
Results of anteroposterior knee laxity when stress was exerted on the knees were reported in 5 studies.1,17,26,35,36 The difference in postoperative ΔATT between ACL repair and reconstruction was not statistically significant, with no heterogeneity (WMD = 0.35; 95% CI, -0.09 to 0.79; I2 = 0%; P = .12) (Figure 4A). Three studies compared postoperative Lachman test results and found no significant differences between the 2 groups (OR = 1.59; 95% CI, 0.42-5.95; I2 = 42%; P = .49).1,26,35 We performed subgroup analysis by follow-up time and found that the I2 value decreased dramatically to 0% in intermediate-term follow-up (OR = 4.93; 95% CI, 0.70-34.55; I2 = 0%; P = .11) (Figure 4B). As there was only 1 study in the short-term follow-up subgroup, we assume that the heterogeneity came from the study by Murray et al. 35

Results of meta-analyses. (A) Difference in laxity between injured and contralateral knees and (B) positive Lachman test (grades 2 and 3). CI, confidence interval; df, degrees of freedom; IV, inverse variance; M-H, Mantel-Haenszel.
Meta-analysis of Secondary Outcomes: Adverse Events and Knee Functional Outcomes
Reoperation was defined as ipsilateral surgery during follow-up, including revision ACL surgery, meniscal fixation or resection, cleaning of postoperative adhesion and infection, cyclops lesion removal, and implant removal. There were 8 studies comparing reoperation rates between the ACL repair and reconstruction groups.1,6,17,22,23,26,35,36 The group differences were statistically significant, with more repeated surgeries in the repair group than in the reconstruction group (OR = 1.87; 95% CI, 1.33-2.62; I2 = 29%; P = .0003) (Figure 5A).

Results of meta-analysis of (A) reoperation, (B) hardware removal, and (C) failure rates. CI, confidence interval; df, degrees of freedom; M-H, Mantel-Haenszel.
In the 6 studies that compared hardware removal rates between ACL repair and reconstruction, more hardware removal was found to have occurred in the ACL repair group than in the ACL reconstruction group (OR = 6.30; 95% CI, 2.44-16.23; I2 = 0%; P = .0001) (Figure 5B).6,17,22,26,35,36
Failure was defined as a combination of subjective instability, findings at physical examination, and/or graft rupture. There were 8 studies1,6,17,22,23,26,35,36 comparing failure rates between the 2 groups. The differences between the 2 groups were statistically significant, with more failures in the ACL repair group than in the ACL reconstruction group (OR = 1.58; 95% CI, 1.03-2.43; I2 = 0%; P = .03) (Figure 5C).
A total of 6 studies reported postoperative complications, including superficial or deep infection, deep venous thrombosis, and pain at the tibial screw without the need for removal.1,6,17,22,26,36 There was no significant difference in complications between the 2 groups (OR = 1.43; 95% CI, 0.64-3.18; I2 = 0%; P = .38) (Figure 6A).

Results of meta-analysis of (A) complications, (B) reoperation rather than revision, and (C) revision ACL surgery rates. ACL, anterior cruciate ligament; CI, confidence interval; df, degrees of freedom; M-H, Mantel-Haenszel.
Reoperation (rather than revision) was defined as an additional surgical intervention for ipsilateral knee issues other than ACL retears, such as meniscal lesions, synovitis, and arthrofibrosis. Reoperations were reported in 8 studies, with no significant difference in reoperation rates between the 2 groups (OR = 1.29; 95% CI, 0.81-2.06; I2 = 0%; P = .29) (Figure 6B).1,6,17,22,23,26,35,36
Revision surgery was defined as repeat ACL reconstruction or conversion to ACL reconstruction due to rerupture or adverse events (recurrent instability). ACL revision rates were reported in 6 studies.6,17,22,23,26,35 There was no significant difference in ACL revision rates between the 2 groups (OR = 1.53; 95% CI, 0.99-2.36; I2 = 0%; P = .05) (Figure 6C).
Changes in postoperative strength in the muscles surrounding the knee joint were assessed by 2 studies.35,36 The difference in isometric hamstring strength between the 2 groups was statistically significant, with higher hamstring strength in the ACL repair group than in the reconstruction group (WMD = 36.69; 95% CI, 29.07-44.31; I2 = 0%; P < .01) (Figure 7A). There was no statistically significant difference in the comparison of isometric quadriceps strength between the 2 groups, with no heterogeneity (WMD = -1.89; 95% CI, -6.82 to 3.04; I2 = 0%; P = .45) (Figure 7B).

Results of meta-analysis of (A) isometric hamstring strength and (B) isometric quadriceps strength. CI, confidence interval; df, degrees of freedom; IV, inverse variance.
A total of 3 studies reported the results of hop tests, including 6-m timed hop, single hop, triple hop, and crossover hop.22,35,36 There was no statistically significant difference in the comparison of hop tests between the 2 groups, except for longer times in the ACL repair group in the 6-m timed hop test (WMD = 6.26; 95% CI, 2.12-10.39; I2 = 0%; P = .003) (Figure 8 A-D).
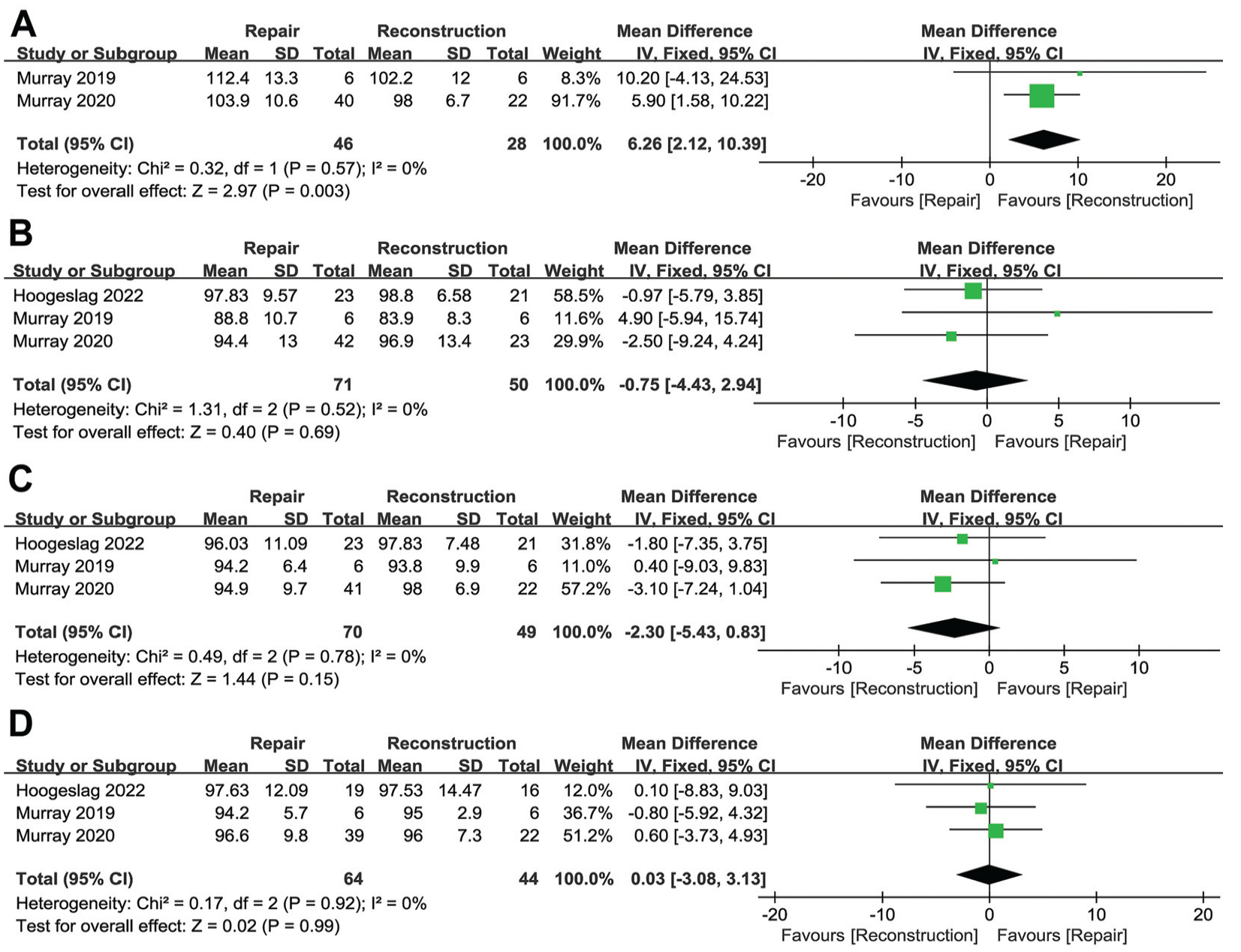
Results of meta-analysis of (A) 6-m timed hop test, (B) single-hop test, (C) triple-hop test, and (D) crossover hop test outcomes. CI, confidence interval; df, degrees of freedom; IV, inverse variance.
Discussion
In this meta-analysis, we found that with a minimum follow-up period of 2 years, arthroscopic ACL repair was associated with higher rates of failure, reoperation, and hardware removal compared with ACL reconstruction. On the other hand, ACL repair was associated with better postoperative outcomes in terms of Lysholm scores and better hamstring strength. In addition, ACL repair yielded functional knee outcomes comparable with those of ACL reconstruction.
The majority of results of our meta-analysis are consistent with those of previous meta-analyses; however, our meta-analysis revealed several differences. In the meta-analysis by Pang et al, 39 with a mean follow-up of 12 to 28 months, the difference between ACL repair and ACL reconstruction in anteroposterior knee laxity was not statistically significant, but the heterogeneity was high (I2 = 80%). After removing the study by Szwedowski et al, 45 which had a mean follow-up shorter than 15 months, the I2 decreased dramatically and ACL repair showed significantly larger ΔATT than ACL reconstruction. In our meta-analysis, with a minimum follow-up of 2 years, no statistically significant difference was found between the repair and reconstruction groups in ΔATT, and the heterogeneity was low (I2 = 0%). In terms of the positive postoperative Lachman tests, the heterogeneity of the overall pooled outcome was relatively high (I2 = 42%) but decreased to zero in the intermediate-term subgroup. We suspected that the heterogeneity was from the different manifestations of the Lachman test result in the 3 included studies.1,26,35
With a minimum follow-up of 24 to 60 months, the ACL repair group had similar IKDC subjective score and higher Lysholm score when compared with the ACL reconstruction group. In the previous meta-analysis, with a mean follow-up period of 12 to 28 months, the difference in Lysholm score between the 2 groups was not statistically significant and the ACL repair group showed a significantly higher IKDC subjective score. 39 However, the number of included studies (n = 2) was too small to confirm the superiority of ACL repair regarding postoperative Lysholm score.
It seems that, compared with ACL reconstruction, ACL repair has a better return to activity, knee function, and quality of life during early follow-up, but, when regarding the longer follow-up time, no significant difference was found. A randomized clinical trial by Barnett et al 5 with a maximum follow-up time of 2 years showed that patients undergoing the BEAR procedure had a higher IKDC score and Knee injury and Osteoarthritis Outcome Score (KOOS) as well as better hamstring muscle strength than patients undergoing ACL reconstruction at early timepoints postoperatively. However, the gap between BEAR and ACL reconstruction in IKDC score and KOOS narrowed over time, whereas significant differences in hamstring strength persisted until the 2-year follow-up. 5 Other studies, using BEAR or other ACL repair techniques, found similar superior outcomes after ACL repair compared with ACL reconstruction in the early months postoperatively.41,47 The advantages of ACL repair, such as the lack of donor site morbidity from graft harvest and the avoidance of bone tunnel drilling, are believed to contribute to a quicker resolution of knee symptoms, earlier return of patient satisfaction, and fewer postoperative complications.5,24 It is noteworthy that these advantages of ACL repair happen primarily in the early stage after surgery.
In our meta-analysis, with a minimum follow-up period of 24 to 60 months, failure rate, reoperation rate, and hardware removal were statistically higher in the ACL repair group than in the ACL reconstruction group. In the previous meta-analysis, with a mean follow-up period of 12 to 28 months, no significant difference in failure rates was observed between the 2 groups. 39 It is believed that the different histological response of ACL to healing contributes to the high failure rate after ACL repair. When ACL rupture happens, the fibrin-platelet scaffold does not form across the defect as extra-articular ligaments do. This special healing process and the lack of vascularity hinder the healing of the injured ACL. 34 Although augmented devices, such as the DIS technique, help create a stable healing environment for ACL and the outcomes are significantly better than the disappointing outcomes after historical open ACL repair, the reported failure rates at midterm follow-up are higher than those at short-term follow-up, especially after ACL repair with dynamic augmentation.3,10 Interestingly, the revision rate was not statistically different between the 2 groups. Eight studies reported failure rates and only 6 studies reported ACL revision rates. Studies that reported ACL revisions had also reported failure rates, but 2 of the studies only reported failure rates.1,36 The 2 studies did not explain whether ACL revisions were performed after failure, although it is generally believed that failure will require revision. ACL repair showed a significantly higher hardware removal rate, which was consistent with the previous meta-analysis. This is probably because most of our included studies used a DIS augmentation technique, in which the monobloc spring-screw is much bulkier than that used in ACL reconstruction, leading to a frequent removal of hardware. 27 Review of the studies indicated that most reoperations were caused by hardware removal, scar tissue, range of motion deficits, and arthrofibrosis, which might be caused by the additional spring device that is implanted in the tibia during repair, especially repair with dynamic augmentation. Suture tape augmentation seems to be a safer technique than DIS, as a lower reoperation rate was reported. 23 Given the findings in this study that the failure rates, reoperations rates, and hardware removal rates were relatively higher with arthroscopic ACL repair, future systematic reviews with a larger cohort and longer mean follow-up time are necessary to assess the reproducibility of our results.
For strength testing and hop testing, the ACL repair group showed a better hamstring strength but a slower 6-m timed hop test. It is worth noting that, in 2 of the included studies that reported hamstring strength,35,36 most of the patients in the ACL reconstruction group used hamstring tendon autografts, which might lead to the weakness of hamstring muscles. 35 It is unclear why the ACL repair group had slower 6-m timed hop test while other hop test results showed no significant difference, but a study by Reinke et al 40 suggested that the timed test is not a predictor of patient-reported outcomes at 2 years after ACL reconstruction.
In the 21st century, investigations of and interests in primary ACL repair have reemerged. Several reasons account for this renewed interest. First is strict patient selection; in the historical literature, repair was performed for all ACL tear types, which was one of the main reasons for poor historical outcomes. Recent ACL repair techniques have gained better clinical outcomes by being performed only on proximal tears because the proximal and distal ends of the ligament have better vascularity and healing potential. 48 The second reason is the prevalence of arthroscopic surgery, which is less invasive and leads to higher postoperative activity function level, lower reoperation rates, and earlier start of rehabilitation than open arthrotomy. 29 Another important reason for the revisitation of primary repair is the invention of new surgical techniques to enhance the biomechanical properties of the repaired ACL (SAR, suture augmentation repair, DIS, IBLA, and BEAR).
Because of the safety and stability of the procedure, with consistently satisfactory long-term outcomes and a recent failure rate of <5%, 24 ACL reconstruction is considered the gold standard surgical treatment for ACL ruptures. Considering the advantages of less invasive surgical techniques, avoidance of donor-site morbidity, and faster postoperative recovery, primary ACL repair is expected to become an alternative for ACL reconstruction in the selected group of patients. Future prospective comparative studies, especially those reporting knee functional outcomes, postoperative knee laxity, and patient-reported outcomes, are needed because existing studies are inadequate to draw reliable clinical conclusions.
Limitations
Our study has some limitations. First, although the minimum follow-up time ranged from 24 to 60 months, only 2 RCTs reached 5 years. The minimum follow-up of our study was still not long enough and more patients need to be followed up until at least 5 years. Most included studies were cohort and case-control studies, and the total number of RCTs was only 4. Second, we did not conduct subgroup analysis. Previous meta-analysis found no significant differences between different rupture locations and repair techniques at short-term follow-up. However, whether the results will be sustained at long-time follow-up is still unknown because there are too few long-term comparative studies focusing on different surgical techniques and patient populations to conduct subgroup analysis. Some potential confounders, such as age and preoperative activity level, were not corrected, which might cause risk of bias because younger age and (pursuit of) higher activity level have been reported to negatively influence the outcomes of both modern ACL repair and ACL reconstruction.50,51 Third, because all recent studies comparing primary ACL repair using the IBLA technique with ACL reconstruction had a follow-up time of <2 years, this technique was not included in our study, which might have created bias in the overall pooled outcomes.
Conclusion
At minimum 2-year follow-up, augmented ACL repair was associated with higher rates of reoperation, hardware removal, and failure compared with ACL reconstruction. However, augmented ACL repair showed higher Lysholm scores and hamstring strength when compared with autograft ACL reconstruction.
Supplemental Material
sj-pdf-1-ojs-10.1177_23259671231223743 – Supplemental material for Comparison of Clinical Outcomes Between Modern Augmented ACL Repair and Autograft ACL Reconstruction: A Systematic Review and Meta-analysis of Studies With Minimum 2-Year Follow-up
Supplemental material, sj-pdf-1-ojs-10.1177_23259671231223743 for Comparison of Clinical Outcomes Between Modern Augmented ACL Repair and Autograft ACL Reconstruction: A Systematic Review and Meta-analysis of Studies With Minimum 2-Year Follow-up by Yunong Ren, Jia Wang, Junjie Ji, Chao Zhang and Qingyang Meng in Orthopaedic Journal of Sports Medicine
Footnotes
Final revision submitted July 23, 2023; accepted August, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: Research support was received from the Peking University Medicine Sailing Program for Young Scholars’ Scientific & Technological Innovation (BMU2023YFJHMX008). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.