
Abstract
Purpose:
We studied the effect of using wide contoured pneumatic tourniquet (PT) versus ultra-narrow sterile exsanguination tourniquet (SET) on the length of hamstring autograft for anterior cruciate ligament (ACL) reconstruction in patients with tubular and conical thighs.
Methods:
Fifty-eight patients undergoing ACL reconstruction between 2012 and 2013 were assigned to either SET or PT groups. We measured the tendon graft length and width as well as the patients’ height, weight, and thigh circumference of 10 cm proximal to the patella and the distance from the anterior–superior iliac spine to the medial malleolus (ASIS-MM). We defined the ratio between the ASIS-MM and the thigh circumference as the conicity index (CI). All grafts were measured after folding into half, and the found value was recorded as functional graft length (FGL). Tendon graft dimensions were correlated with the individual anthropometric data and with CI in each of the groups.
Results:
PT was used in 34 patients and SET on 24 patients. FGL was 12.7 ± 0.84 mean + standard deviation for the SET group versus 11.5 ± 1.61 for the PT group (p = 0.0011) with a strong positive correlation between FGL and CI for the PT group (R 2 = 0.625; p = 2.6 × 10−8) but nonsignificant correlation for the SET (R 2 = 0.222). Graft thickness was correlated with the patient age (R 2 = 0.450) but not with CI or type of tourniquet used. We found the CI to be a better measure of thigh conicity than thigh circumference, length, height, weight, or body mass index individually.
Conclusion:
We conclude that using the SET which occupies less space on the thigh yielded significantly longer hamstring autologous ACL graft compared to the PT and the FGL became essentially independent from the CI when the SET was used.
Introduction
Anterior cruciate ligament (ACL) is the second-most injured structure of the knee joint, preceded by the meniscal cartilage. Hamstring or patellar tendon autografts and allografts are currently used, and various fixation practices are performed for ACL reconstruction. Hamstring autografts can easily be harvested from their insertion at the proximal tibia by a tendon stripper when anatomical details of fascial attachments at the distal portion of both tendons are well recognized. 1 Also, as described by Solman and Pagnani, when harvesting the gracilis tendon, the stripper is aimed toward the ipsilateral lesser trochanter; when harvesting the semitendinosus, the stripper is aimed toward the ipsilateral ischial tuberosity. 2 Diverting the stripper away from its natural course may cause early strike off, affecting the length of the harvested graft. The tissue pressure exerted by the tourniquet may affect such diversion. Although there are many reports about graft length required for ACL reconstruction in literature, there is no consensus about exact graft length needed. At least 22-cm graft (11 cm as folded) is advised for appropriate ACL reconstruction. 3,4
Harvesting longer graft may allow doubling of the graft with an increased diameter, providing enough length for adequate graft within the femoral tunnel and for the fixation of the graft outside the tibial tunnel. 5 Furthermore, a longer graft can also enable reconstructing the ACL with only semitendinosus as reported by Kyung at al. before. 6,7
A bloodless field is generally preferred by many surgeons at the time of ACL reconstruction. Tourniquet use facilitates both graft harvesting procedure and arthroscopic reconstruction of the ACL with or without intra-articular pathology management. To date, the effect of tourniquets on thigh structures was evaluated, but the actual effect of the tourniquet type on the graft length especially for patients with tapered and short thigh and overweight patients is not available in the literature. 8 –11
The purposes of the current study were to investigate the effect of the type of tourniquet used during ACL reconstruction with autologous harvested hamstring ligaments and to correlate the results with anthropometric measurements of the patients and the extent of taper of their thighs. We hypothesized that pneumatic tourniquet (PT) prevents harvesting a longer ligament on tapered limbs so sterile exsanguination tourniquet (SET) can be an alternative to overcome this. PT when used on tapered limbs may cause early strike off the tendon grafts and this can be prevented with the use of SET with a diameter of 3 cm.
Methods
The trial was approved by the appropriate Ethics Committee of the hospital. Fifty-eight consecutive patients undergoing ACL reconstruction using hamstring autograft tendons between 2012 and 2013 were included in the study. Preoperative physical examination was performed; Lachman and pivot shift tests were used to assess the integrity of the ACL. The diagnosis was confirmed by magnetic resonance imaging. The same surgical team implementing the same procedure for all cases carried out all ACL reconstruction operations. Patients received written information about the trial. Before randomization, informed consent was obtained from each patient. Each patient received numbered and blinded randomization envelopes and data on all ACL reconstruction patients were prospectively recorded on a structured pro forma by independent data clerks.
SET (HemaClear®; OHK Medical Devices Ltd, Haifa, Israel) and wide contoured PT (A.T.S®; Zimmer Ltd, Warsaw, Indiana, USA) were applied on the patients’ thighs to facilitate bleeding-free surgical field during the operation. The applied PT was a contoured cuff with a width of 14 cm. The tourniquet cuff was placed as described by Genuario et al. at the most proximal point of the limb, while both the knee and hip joints were flexed. 12 The SET was advanced to the most proximal point of the thigh and its width was 3 cm.
Before reconstructing the ACL, arthroscopy of the knee was performed to detect any coexisting additional pathology; if found, these pathologies were first repaired. ACL of all the patients was reconstructed using autologous hamstring tendon grafts harvested with a tendon stripper. This was followed by a longitudinal incision made at the medial proximal tibial metaphysis and distal part of the graft was fixed to the tibia with a bioabsorbable screw.
The semitendinosus and gracilis tendons were harvested from all of the patients and were folded into half; then their length was measured. This length was named as “functional length.” Additionally, the width of the four-strand autografts was recorded. Patients’ height, weight, anterior–superior iliac spine to the medial malleolus (ASIS-MM) distance, the thigh circumference, and their body mass index were recorded preoperatively. The circumference of the thigh was measured 10 cm proximal to the upper pole of the patella. The duration of surgery was measured starting from the onset of tourniquet pressure (PT or SET) administration and ended at the end of the procedure.
The use of straight tourniquets on conical thighs should be avoided, especially in extremely muscular or obese individuals. 13,14 As noted by Schwartzberg et al., there is no broadly accepted criterion to characterize the shape of a conical thigh. 5 Neither Pedowits nor Schwartzberg reported an objective criterion for describing the conicity of the thigh. In our study, we used the ratio between the ASIS-MM distance and the thigh circumference as conicity index (CI) to describe the conicity.
Linear regression analysis (MS Excel 2010 add-in statistical tools) was used to determine the slope, intercept, regression coefficient (R 2), confidence intervals, and p value of the correlations, when p < 0.05 was accepted as statistically significant. κ-Coefficients were also calculated for determining the agreement levels between observers regarding all measurements including tendon length and width and patients’ demographics.
Results
The mean age of the study population was 30.7 ± 7.7 years (range, 18–46 years). Study groups in Table 1 show demographics and measurements of the study population. The groups’ demographics were not statistically different. PT was applied to 34 patients (58.6%) and SET to 24 patients (41.4%). The κ-coefficient for tendon length and width assessments was 0.731 and 0.840, respectively, for patients’ demographics assessments, and both assessments had a p-value of <0.001.
Patients’ demographics by groups.
SD: standard deviation; SET: sterile exsanguination tourniquet; PT: pneumatic tourniquet; BMI: body mass index.
The graft width and the functional graft length (FGL) values of the two groups are shown in Table 2. There was no significant difference in the graft width among the groups, but there was a substantial (12 mm) and highly significant difference (p = 0.0011) in the FGL between the SET and the PT groups. Besides, finding the variability of FGL (i.e. the standard deviation) was twice as high in the PT group compared to the SET group.
Leg length, thigh circumference, and CI as well as graft width and length are shown by tourniquet groups.a

FGL: functional graft length; CI: conicity index; SET: sterile exsanguination tourniquet; PT: pneumatic tourniquet; SD: standard deviation; ASIS-MM: anterior–superior iliac spine to the medial malleolus.
a Note that the FGL was significantly longer by 1.3 cm in the SET group.
Mean ASIS-MM distances by groups, thigh circumference values, and CI defined as the ratio between the two are shown in Table 2. There were no significant differences in these anthropometric measurements between the groups. Figure 1 shows the relationship between FGL and CI in the SET group (A) and in the PT group (B). In the PT group, 18 of the 34 patients had an FGL of 11 cm or less. This was particularly noticed in patients who had a CI that was less than 2.0 (i.e. short leg and/or large circumference), so that there was a strong influence of CI on the FGL (R 2 = 0.63; p < 0.0001). In the SET group, all the patients except one had an FGL that was longer than 11 cm and there was only a weak correlation between the FGL and CI in the SET group (R 2 = 0.22; p = 0.02).

FGL versus CI in the SET group (a) and the PT group (b). Note that in the PT group, 18 of 34 patients had a length of 11 cm or less, whereas in the SET group, there was only one patient with 11-cm graft (none with less). Also, note the strong dependence of the FGL on CI in the PT group, but not in the SET group. FGL: functional graft length; CI: conicity index; SET: sterile exsanguination tourniquet; PT: pneumatic tourniquet.
Surgical time was 90.6 + 21.1 min with the PT and 80.9 + 20.7 min with the SET (p = 0.085) with mean time for the entire population being 84.9 ± 21.2 (range 45–125) min. The type of anesthesia (general or spinal) and age did not affect the graft length. However, graft width positively correlated with the patients’ age (Figure 2). This observations in agreement with the findings presented by Melville at the American Orthopedic Society for Sports Medicine 2011 Annual Meeting who reported that younger patients had narrower hamstring graft. 15
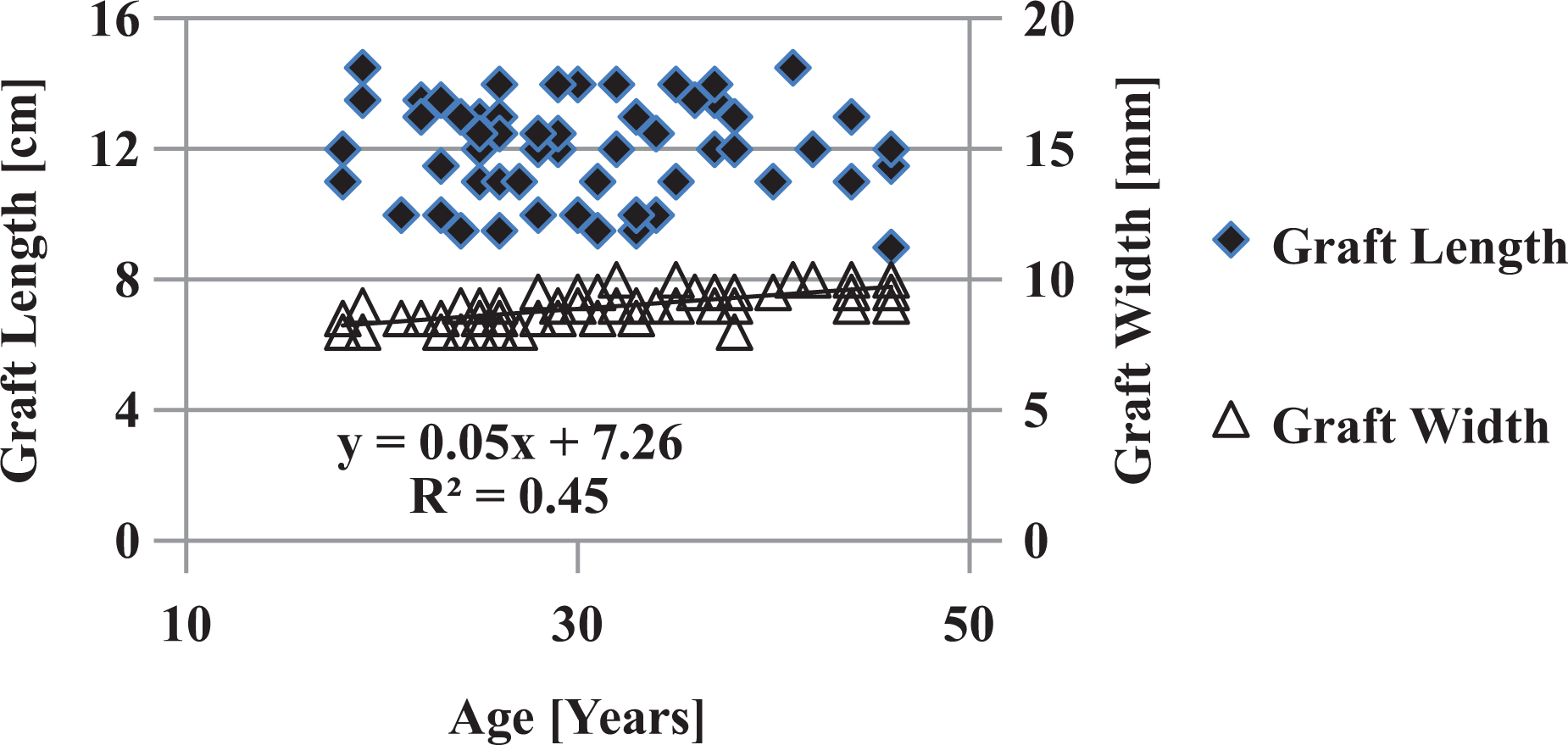
Correlation between FGL and width with the patients’ age. Note the linear increase in graft width with age, but no correlation of graft length. FGL: functional graft length.
Discussion
In this study, we compared a group of patients undergoing ACL autologous reconstruction using a wide contoured PT cuff (A.T.S; Zimmer Ltd) with a similar group undergoing the procedure with an ultra-narrow surgical exsanguination tourniquet (HemaClear; OHK Medical Devices Ltd). The wide contoured tourniquet cuff, recommended for tapered limbs of shorter and overweight patients by McEwen et al., occupies an area that is 14-cm wide on the thigh, while the SET occupies about 3 cm. 16 The main finding in the present study is that when using the SET, the length of the harvested graft was significantly longer than with the PT. Perhaps, more important is the observation that in patients with low CI (i.e. more tapered thigh), the use of the PT resulted in an FGL that was exceedingly short—11 cm or less as shown in Figure 1. When the SET was used, the dependence of the FGL on CI was substantially less than with the PT (slope of 1.5 vs. 5.5). In addition, all grafts were more than 11-cm long except in one patient whose FGL was 11 cm (Figure 1). The fact that the SET can be placed higher on the thigh thereby providing more space for stripping the ligament without the compression effect of the tourniquet as shown in Figure 3 may play an important effect in this outcome.

Space to the distal end of the patella from the distal end of the PT (left panel) and the distal end of the SET (right panel). Note the substantially greater free field when both devices are positioned near the groin. SET: sterile exsanguination tourniquet; PT: pneumatic tourniquet.
In fact, in autologous ACL reconstruction, tendon graft length is as important as its width. A longer graft may allow doubling of the graft into half with an increased diameter and enable reconstructing the ACL with only semitendinosus as reported before. 6 And also a longer tendon-bone contact can be achieved with a longer harvested graft in femoral tunnel. Fixation techniques outside of the tibial tunnel such as staples and some other proprietary fixation devices require that the grafts exit the tibial tunnels for a certain minimal distance. 5 On the basis of the report of the second ESSKA scientific workshop concerning reconstruction of the cruciate ligament held in 1996, it was noted that choosing different graft tunnel positions affected the graft length. 17
Recent studies showed that hamstring autograft ACL reconstruction was associated with more satisfactory results especially on the patients aged 40 and over. 18 American Orthopedic Society for Sports Medicine argued that the underlying reason was that younger patients had narrower graft size. 15 A positive correlation between graft width and patients age is defined in the literature and this was confirmed by our study. Yet no relationship was detected between graft length and patients age (Figure 2). So other factors must be considered to achieve a longer graft for the patients at any age, for example, tourniquet type as stated in this study.
A limitation of the study is lack of preoperative magnetic resonance imaging of the cross-sectional area of the interested tendons for their length and width. Although it seems better to predict the structural properties of the tendons preoperatively by such techniques, measuring leg length and body weight can do a simpler way of prediction. However, this is not always the case, as we showed the inverse effect of the PT on the length of the grafts obtained by the stripper. There is no data in literature about incidence of harvesting short hamstring autografts due to the PTs, but this study demonstrated that autograft lengths may vary via tourniquet types. We speculate that the wide contoured pneumatic cuff when used on tapered limbs caused the tendon stripper to divert from the natural course of the tendon resulting in an early cut, possibly due to the cuff pressure compression of the muscles with migration of some of the muscle mass toward the distal thigh. The results of this study indicate that this is not the case when the SET is used, possibly because there is much less shifting of compressed muscles distally. The strengths of this study are prospective data collection and being the first comparative study evaluating the two different tourniquets on proper graft derivation.
In a study published by Apostolopoulos et al., including 72 patients, it was reported that the length of the hamstring autograft ranged from 11 cm to 13.5 cm and the diameter from 7 mm to 9 mm. 19 In our study, the length of the autologous hamstring tendon ranged from 9.5 cm to 14.5 cm and the diameter from 8 mm to 10 mm. The failure to harvest long enough tendon graft may lead to the use of alternative graft sources. Schwartzberg et al. questioned whether common anthropometric measurements in patients undergoing ACL reconstruction with autologous hamstring tendon graft could predict autograft length and diameter. They found that doubled semitendinosus and gracilis graft length for ACL reconstruction was strongly associated with leg length. 5
Although it is not statistically significant, SET provided quite shorter surgery time in this study. This situation can be explained by the easiness of the SET application. The application of PT is more complex in terms of need for elevation, Esmarch bandage usage, or pressure adjustment according to arterial blood pressure level.
The most prominent factor influencing the length of the hamstring autograft is surgical technique. While harvesting the gracilis and semitendinosus tendons, all fascial branches of the tendon need to be freed so that the body of the tendon is not amputated in mid-substance before the entire muscle is stripped. Incomplete removal may cause the tendon stripper to follow one of the branches and prematurely amputate the tendon. 20 When harvesting the gracilis tendon, the stripper is aimed toward the ipsilateral lesser trochanter; when harvesting the semitendinosus, the stripper is aimed toward the ipsilateral ischial tuberosity. 2 Figure 4 shows the dissection of a cadaver featuring the linear course of the gracilis tendon and its muscular portion, which is longer than the semitendinosus tendon. Previous studies that established a link between early cut of hamstring tendon autograft and fascial branches also correlate shorter tendon grafts with lower extremity length.

The dissection of a cadaver featuring gracilis and semitendinosus ligaments.
Conclusions
We conclude that the use of SET provides a longer autologous graft for ACL reconstruction. This was particularly prominent in patients having lower CI value (more tapered).
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.