
Abstract
Background:
Anterior cruciate ligament (ACL) injury reduction training has focused on lower body strengthening and landing stabilization. In vitro studies have shown that quadriceps forces increase ACL strain, and hamstring forces decrease ACL strain. However, the magnitude of the effect of the quadriceps and hamstrings forces on ACL loading and its timing during in vivo landings remains unclear.
Purpose:
To investigate the effect and timing of knee muscle forces on ACL loading during landing.
Study Design:
Descriptive laboratory study.
Methods:
A total of 13 young female athletes performed drop vertical jump trials, and their movements were recorded with 3-dimensional motion capture. Lower limb joint motion and muscle forces were estimated with OpenSim and applied to a musculoskeletal finite element (FE) model to estimate ACL loading during landings. The FE simulations were performed with 5 different conditions that included/excluded kinematics, ground-reaction force (GRF), and muscle forces.
Results:
Simulation of landing kinematics without GRF or muscle forces yielded an estimated median ACL strain and force of 5.1% and 282.6 N. Addition of GRF to kinematic simulations increased ACL strain and force to 6.8% and 418.4 N (P < .05). Addition of quadriceps force to kinematics + GRF simulations nonsignificantly increased ACL strain and force to 7.2% and 478.5 N. Addition of hamstrings force to kinematics + GRF simulations decreased ACL strain and force to 2.6% and 171.4 N (P < .001). Addition of all muscles to kinematics + GRF simulations decreased ACL strain and force to 3.3% and 195.1 N (P < .001). With hamstrings force, ACL loading decreased from initial contact (time of peak: 1-18 milliseconds) while ACL loading without hamstrings force peaked at 47 to 98 milliseconds after initial contact (P = .024-.001). The knee flexion angle increased from 20.9° to 73.1° within 100 milliseconds after initial contact.
Conclusion:
Hamstrings activation had greater effect relative to GRF and quadriceps activation on ACL loading, which significantly decreased and regulated the magnitude and timing of ACL loading during in vivo landings.
Clinical Relevance:
Clinical training should focus on strategies that influence increased hamstrings activation during landing to reduce ACL loads.
Injury reduction is the optimal concept to avoid the complications of extended rehabilitation, failure to return to sport, and high rates of second injury that are associated with anterior cruciate ligament (ACL) rupture. 1,16,38,44 Literature indicates that incidence of ACL injury can be mitigated across a population by interventions targeted at modifiable risk factors, such as neuromuscular control and movement biomechanics. 20,56 Specifically, implementation of neuromuscular training programs that incorporate lower body strength, landing stabilization, core strength, agility, plyometrics, and balance 39 influence muscle activations in a manner that mitigates biomechanical risk factors associated with ACL injury during landing tasks. 17,18,39,49 However, the specific impacts of targeting muscular recruitment and strengthening strategies on ACL loading have not been well established owing to the difficulty of assessing direct ACL loads in vivo.
In vitro experimental testing indicates that quadriceps forces increase ACL loads, as opposed to hamstrings forces, which reduce ACL strain. 32,43,47 In quasi-static conditions, 400 N of quadriceps tension was shown to increase ACL strain by 3% to 5%. 43,47 This is consistent with an in vivo study that reported ACL strain increased with quasi-static quadriceps contraction. 4 Conversely, greater quadriceps tension decreased (or did not change) ACL loading during simulated in vitro landings. 15,30 These studies suggested that the response of ACL loading to quadriceps force would be different between quasi-static and dynamic conditions. The effect of muscle contractions on ACL loading during in vivo landing tasks remains unclear, as multiple interactions take place between dynamic kinematics, muscle forces, and ground-reaction force (GRF). Specifically, the magnitude of the effect of quadriceps and hamstrings forces on ACL loading and its timing during landing remains unexplored.
Musculoskeletal models are helpful, as they allow investigators to estimate in vivo muscle forces and ligament loading, which is not experimentally measurable. 24,28,35,36,51,53,55 A previous musculoskeletal modeling study revealed that hamstrings force is more effective at decreasing anterior tibial shear force during a drop vertical jump (DVJ) than quadriceps force at increasing it. 36 However, that study did not investigate ligament loading because ligamentous structures were not included in the model.
A validated knee joint model is necessary to provide physiologic knee ligament loading because generic material properties fail to account for the specimen-specific coupling of shape and structural properties. 34 Only some musculoskeletal modeling studies have reported ligament loading with validated material properties and a 6 degrees of freedom (DOF) knee joint, which is optimal for the accurate assessment of ligament loading. 24,28,35,48,55 Once a musculoskeletal model is validated, it can be used to simulate the individual effect of multiple factors, including kinematics, muscle forces, and/or GRF during landing. 34 A similar technique utilizing a validated model was used in previous studies to test other joints and tasks, 13,23,24,29,35,48 but ACL loading during a landing task has not been studied.
The purpose of this study was to employ a validated musculoskeletal model to test the individual effect of kinematics, GRF, and muscle forces on ACL loading during a simulated landing task. We hypothesized that isolated quadriceps force would increase ACL loading, whereas hamstrings would decrease ACL loading above and beyond the effect of quadriceps contributions during landing simulations. 15,30,57 Furthermore, because ACL injury occurs at 40 to 60 milliseconds after initial contact with anterior tibial translation, 3,26,27,37,52 we hypothesized that hamstrings would decrease ACL loading around this time range as an agonist of ACL. This would shift the time of peak ACL loading to the initial contact, at which time the knee flexion angle is at its minimum. 8
Methods
Experimental Testing
The experimental data collection for this study was previously described in detail. 53 In brief, 13 female high school volleyball players (mean age, 15.6 ± 1.6 years; mean height, 169.8 ± 5.6 cm; mean weight, 62.6 ± 5.2 kg) participated in this study. Each participant performed 3 DVJ trials from a 30 cm–high box. Individuals’ 3-dimensional body positions and surface electromyography (EMG) data for the right leg were recorded during the DVJ using 35 reflective markers and a motion capture system and telemetry surface EMG system. 11 EMG was recorded for biceps femoris, semitendinosus, rectus femoris, vastus lateralis, vastus medialis, gastrocnemius medialis, hip adductors, and gluteus medius.
Computational Simulations
Sequential OpenSim 6 simulations and 2 finite element (FE) simulation steps were conducted to estimate ACL strain and force during landings. Joint kinematics and kinetics as well as muscle forces were estimated with OpenSim simulations and used as inputs to FE simulations. The individual effect of kinematics, GRF, and muscle forces were investigated by the inclusion/exclusion of these factors in separate simulations of the same motion task (Figure 1).

Workflow of the computational modeling to estimate ligament loading during the drop vertical jump, in which individual landing strategies were maintained. Joint motion and muscle forces were estimated using electromyography-informed optimization in OpenSim simulations. Joint motion was input to a first FE simulation to simulate landing with patient-specific kinematics and to obtain the trajectories of the knee and ankle joint centers. To simulate more physiologic knee joint mechanics, the joint center position was kinematically driven and muscle forces from OpenSim simulation were applied in the second FE simulation. Black arrows on the joint center indicate kinematically driven DOFs. Inferosuperior DOF on the ankle joint was unconstrained to apply vertical GRF, whereas rotation on the transverse plane was kinematically driven to track toe direction. The pelvis was kinematically driven according to the OpenSim inverse kinematics. This allowed hip internal/external rotation as well as knee abduction/adduction and the 3 translations of the knee to be unconstrained and dependent on muscle force, joint contact force, and GRF (see main text for more detailed description). DOF, degrees of freedom; FE, finite element; GRF, ground-reaction force.
OpenSim Simulations
Individual muscle forces were estimated in OpenSim as previously described. 53 Briefly, a generic musculoskeletal model 42 with additional DOFs added for knee abduction/adduction and internal/external rotation as well as additional hip external rotator muscles was scaled to the anthropometric parameters of each participant. These scaled models were used to calculate joint kinematics and muscle forces using EMG-informed direct collocation. 5 The objective function aimed to track participant-specific, experimentally measured EMG signals. In the musculoskeletal modeling step, 2 of 39 trials did not achieve the tolerance of muscle force optimization and were excluded from the analysis.
FE Simulations
A musculoskeletal FE model was created in Abaqus/Explicit (SIMULIA). 34 A generic model of the pelvis was added to 1 of 4 previously developed and validated specimen-specific FE models of the knee (male, left leg in Navacchia et al 34 ). The model included a 3-DOF ball joint at the hip, a 12-DOF knee joint, and a 1-DOF hinge joint at the ankle. The knee joint included specimen-specific bone and cartilage geometries and tibiofemoral and patellofemoral ligaments. The material properties of the ligaments including reference strain and stiffness were calibrated to match simulated kinematics and ACL strain with in vitro experimental testing measurements. 14,34 The 24 muscles (iliacus, psoas, 5 of adductors, 3 of gluteus maximus, 3 of gluteus medius, piriformis, 4 of hamstrings, 4 of quadriceps, 2 of gastrocnemius) that span the hip and knee joints were modeled as unidimensional connectors consistent with the OpenSim simulations.
The same landing tasks simulated with OpenSim were also simulated with the FE model. The FE landing simulation aimed to maintain physiologic mechanics at the knee and individual landing strategies such as knee-in, toe-out landing, which is determined by the knee and ankle joint center locations and toe direction in this study (the toe direction would not change during landing because of the friction). In the first FE simulation, pelvic, hip, knee, and ankle joint motions obtained from the OpenSim simulation were applied in the musculoskeletal FE model. The position in space of the knee joint center (midpoint between the medial and lateral knee condyles) and ankle joint center (midpoint between the medial and lateral malleoli) during landing were recorded. In the second FE simulation, the knee and ankle joint centers tracked their positions recorded in the first FE simulation, while rotational and translational DOF on the hip and knee joints remained unconstrained. The inferosuperior position of the ankle joint center was left free to transfer the ground force (vertical component only, as the other DOFs were kinematically driven) to the knee. In addition, a node on the ankle located 10 mm in front of the ankle joint center was kinematically driven in the mediolateral position to track the toe direction during landing. The muscle forces estimated in OpenSim and the vertical GRF were applied to each muscle and to the ankle, respectively.
This strategy was adopted to simulate the physiological knee joint mechanics while maintaining the individual landing strategies. Skin marker–based joint motions contain skin artifacts 31 and do not take into account the mechanical equilibrium of forces at the knee. Therefore, the knee joint motion obtained from OpenSim simulation in this study was not physiologic enough to assess ACL loading. The first FE simulation was necessary to obtain the joint center location of the FE model in the simulation of motion from OpenSim. The second FE simulation was separately conducted to satisfy mechanical equilibrium of forces at the knee joint. While hip flexion/extension, hip abduction/adduction, knee flexion/extension, and knee internal/external rotation were constrained owing to the kinematically driven knee and ankle joint centers, the positions of internal/external hip rotation, knee abduction/adduction, and translational DOF depended on muscle, ligament, contact forces, and GRF.
ACL strain and force were averaged and summed across the 4 modeled fibers (2 fibers each in the anteromedial and posterolateral bundles of the ACL), respectively. ACL strain was calculated as 100 × (L – L 0)/L 0, where L and L 0 are current length and reference length 9 (slack length determined by optimization in the validation study 34 ), respectively. The FE simulation was conducted under 5 different conditions to sequentially investigate the individual effect of GRF and muscle forces on ACL loading with respect to the kinematics-only condition:
Kinematics condition (no application of GRF and muscle forces)
GRF condition (kinematics + GRF)
Quadriceps condition (kinematics + GRF + quadriceps)
Hamstrings condition (kinematics + GRF + hamstrings)
Normal condition (kinematics + GRF + all muscles)
Statistical Analysis
The Friedman test with post hoc Nemenyi multiple comparison test was used to examine the differences in ACL loading and peak time between the 5 conditions. Statistical tests were performed with R, package “PMCMR” 41 using jamovi V 1.2 (The jamovi project, https://www.jamovi.org). Statistical significance was set at P < .05.
Results
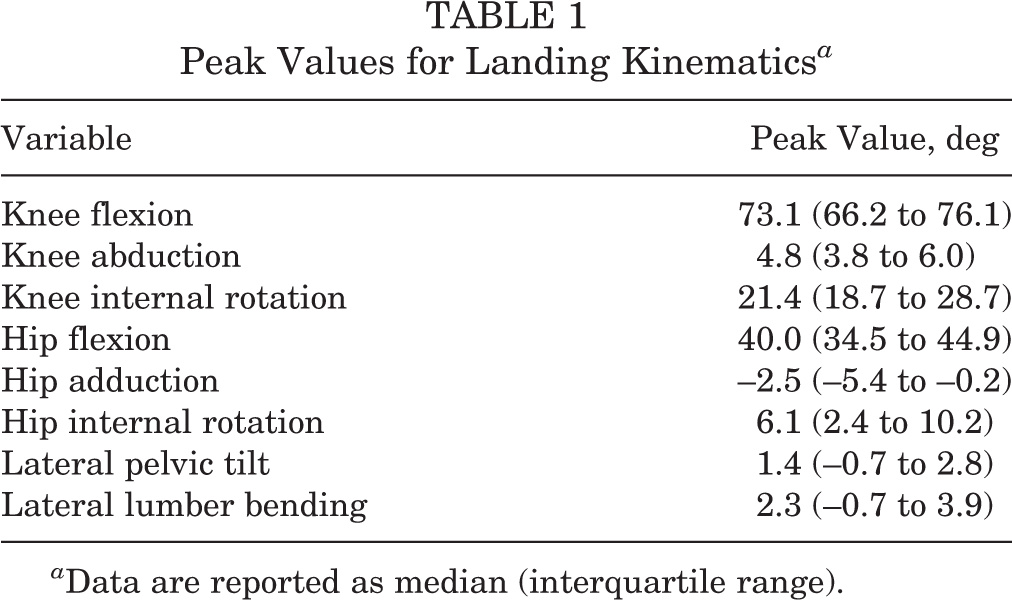
The peak values for the landing kinematics are presented in Table 1, and Figure 2 shows the median ACL strain and force plotted across time for the 5 study conditions. For the kinematics condition, the median peak ACL strain and force were 5.1% (interquartile range [IQR], 4.3%-6.1%) and 282.6 N (IQR, 241.1-379.7 N), respectively (Table 2 and Figure 3, A and B). Significant increases in ACL strain and force were seen in the GRF condition compared with the kinematics condition, by 33% (P = .017) and 48% (P = .011), respectively. Nonsignificant increases in ACL strain and force were seen in the quadriceps condition compared with the GRF condition, by 5% (P = .824) and 14% (P = .890), respectively. ACL strain and force were significantly decreased in the hamstrings condition compared with the GRF condition, by 62% and 59%, respectively (P < .001 for both). Similarly, strain and force were significantly decreased in the normal condition compared with the GRF condition, by 51% and 54%, respectively (P < .001 for both), as well as the quadriceps condition, by 45% and 41%, respectively (P < .001 for both).
Peak Values for Landing Kinematics a
a Data are reported as median (interquartile range).

Median waveforms of ACL (A) strain and (B) force across time for the 5 different study conditions. Time zero indicates the time of initial contact with the ground. ACL, anterior cruciate ligament; GRF, ground-reaction force.
Magnitude and Timing of Peak ACL Strain and Force by Study Condition a

a Data are reported as median (interquartile range). ACL, anterior cruciate ligament; GRF, ground-reaction force.

(A, B) Magnitude and (C, D) timing of peak anterior cruciate ligament (ACL) strain and force compared across the 5 study conditions. Dots indicate outliers. Asterisks indicate statistically significant differences: *P < .05; **P < .01; ***P < .001. GRF, ground-reaction force.
The timing of peak ACL strain and force after initial contact was significantly later in the kinematics, GRF, and quadriceps conditions compared with the hamstrings and normal conditions (P = .024-.001) (Table 2 and Figure 3, C and D). The median knee flexion angle at initial contact was 20.9° (IQR, 15.9°-27.7°) and reached 73.1° (IQR, 66.2°-76.1°) at 100 milliseconds after initial contact.
Discussion
To our knowledge, this was the first study to investigate the effect of muscle forces on ACL loading during simulations of in vivo landing with a validated musculoskeletal model. The hypothesis tested was that quadriceps force would increase ACL loading whereas hamstrings force would decrease ACL loading in this model. The hypothesis was partially supported, as the application of hamstrings force significantly decreased ACL loading during landing. Conversely, application of quadriceps force did not induce a statistically significant increase in ACL loading. Accordingly, relative to ACL loading, these observations indicate that the agonist effect of hamstrings contraction is larger than the antagonist effect of quadriceps during a landing task.
The results of the quadriceps condition did not directly support or contradict the previously cited in vitro literature that ACL loading remained unchanged when stiffness or preloading of quadriceps muscles was increased. 15,30 In a previous study, 30 the knee flexion angle was decreased because of higher quadriceps force. However, the FE simulation of the present study was designed to keep the knee flexion motion regardless of the quadriceps force or any other force. Therefore, the relationship between ACL strain, quadriceps force, and knee flexion angle found in the previous study 30 was not accounted for in the FE simulation. The kinematics + quadriceps condition without GRF was not tested in this study. ACL loading in such a condition is not expected to exceed the results of the quadriceps condition (kinematics + GRF + quadriceps) since the GRF significantly increased ACL strain when added to joint kinematics.
The result of the hamstrings condition was consistent with previous in vitro landing simulations. 57 The results of the normal condition indicated that the hamstrings compensated for most of the ACL loading that was incurred from GRF and quadriceps. These data indicate that ACL loading can be effectively regulated through hamstrings contraction, even when the applied hamstrings force is smaller (956.5 ± 232.0 N) than the quadriceps force (7278.4 ± 1308.1 N). This is consistent with a previous study that stated 55% of hamstrings force turned into posterior tibial force, whereas only 15% of quadriceps force turned into anterior tibial shear force. 36 These findings provide evidence that hamstrings muscle activation contributes to protection of the ACL during landing tasks. At the same time, they indicate that isolated quadriceps force is not likely sufficient to induce ACL rupture on its own during landing. 7 Rather, the lack of hamstrings contraction combined with risky kinematics and GRF would be the most likely factors to induce ACL injury.
The time of peak ACL loading was delayed when hamstrings force was removed from the simulation. The hamstrings activation presented an increasing trend throughout the landing (see Ueno et al 53 ), whereas the time of peak vertical GRF, knee abduction, internal tibial rotation, and anterior tibial translation, which induce higher ACL strain, were observed from 50 to 90 milliseconds (see Ueno et al 54 for more detailed knee kinematics). When hamstrings force was applied, 17 of 37 trials presented the peak ACL strain within 10 milliseconds after initial ground contact, where the knee flexion angle was at its minimum. These details indicate that kinematics, GRF, and quadriceps force strained the ACL from 50 to 90 milliseconds while hamstrings force canceled out these forces and shifted peak ACL loading to immediately after initial contact (0-10 ms) for the majority of trials. Note that peak ACL loading in the hamstrings condition was significantly smaller than in the other conditions. The time of peak ACL loading with hamstrings activation is consistent with previous fluoroscopic studies. 8,50 This result supports the fact that the hamstrings force regulates knee joint kinematics and ACL loading.
A limitation of this study was that the effect of the gastrocnemius was not tested. Fleming et al 10 reported that the gastrocnemius acts as an antagonist to the ACL as it pulls the femur backward relative to the tibia with an in vivo quasi-static study. Similarly, Navacchia et al 36 reported a musculoskeletal modeling study showing that the gastrocnemius induces anterior tibial shear force more than the quadriceps during landing. However, the similar effect was not simulated because of the constraints used in the FE analysis of this study. In addition, previous studies indicated that the gastrocnemius and quadriceps may contribute to stabilize the knee joint under a complexity of co-contraction. 2,25 These points should be improved and tested further in a future study.
Second, the magnitude of the effect of high-risk kinematics (such as higher knee abduction and internal tibial rotation with laterally leaned trunk) on ACL loading during landing remains unclear. 19,53 This concept should be examined in future studies to clarify the causal effects of individual landing strategies, including asymmetrical landing in the frontal plane and upright landing by changing landing posture. 21,45,46,53 However, these strategies will affect muscle force estimations. Therefore, muscle estimations must be reprocessed with respect to altered landing kinematics. Third, the effect of the anteroposterior and mediolateral components of GRF was not investigated since these DOFs were kinematically driven at the ankle to maintain individual landing strategies. Although the strategy used in this study maintains mechanical equilibrium without the application of horizontal GRFs, those ankle DOFs must be unconstrained to address this limitation. However, the natural landing kinematics would be affected when kinematically driven ankle DOFs were unconstrained. Finally, the muscle force estimation would involve errors. Even though the EMG-informed method helped to account for the co-contraction of quadriceps and hamstrings, 36 surface EMG information would contain errors from crosstalk 33 ; in addition, the estimation was not calibrated to be specific for patients as conducted in a previous study. 22,40 Uncoupled modeling between OpenSim and the FE model in this study would be another factor for the potential errors in the estimation of muscle force and subsequent ACL loads. 12,24,29,35,48
Conclusion
The effect of quadriceps force on increasing ACL loads was smaller than the effect of GRF, whereas relatively small hamstrings force significantly decreased ACL loads during landing. ACL loading was effectively regulated by hamstrings force in a landing simulation model with kinematics, GRFs, and quadriceps co-contraction. The hamstrings muscle was a more influential agonist to ACL loading than any other input parameter was an antagonist. Clinicians should ensure appropriate hamstrings contraction and avoidance of risky kinematics and large GRF to reduce the relative risk of ACL injury.
Footnotes
Acknowledgment
The authors acknowledge the support of the staff at the Materials Structural Testing CORE at Mayo Clinic, the Biomechanics Research Lab at Mayo Clinic, and the Sports Health and Performance Institute at The Ohio State University.
Final revision submitted March 15, 2021; accepted April 30, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was supported by funding from the National Institutes of Health (grants R01AR049735, R01AR056259, R01AR055563, K12HD065987, and L30AR070273). A.N. is an employee of Smith & Nephew. G.D.M. has received royalties from Human Kinetics and Wolters Kluwer and is an inventor of biofeedback technologies (2017 Non Provisional Patent Pending- Augmented and Virtual reality for Sport Performance and Injury Prevention Application 62/420,119, software copyrighted) designed to enhance rehabilitation and prevent injuries and has potential for future licensing royalties. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Cincinnati Children’s Hospital Medical Center (study ID: 2008-0023).