
Abstract
Background:
Understanding the morphology of cartilage/bony maturation in preadolescents may help explain adult trochlear variation.
Purpose:
To study trochlear morphology during maturation in children and infants using magnetic resonance imaging (MRI).
Study Design:
Descriptive laboratory study.
Methods:
Twenty-four pediatric cadaveric knees (10 male and 14 female knees; age, 1 month to 10 years) were included. High-resolution imaging of the distal femoral secondary ossification center was performed using 7-T or 9.4-T MRI scanners. Three-dimensional MRI scans were produced, and images were reformatted; 3 slices in the axial, sagittal, and coronal planes images were analyzed, with coronal and sagittal imaging used for image orientation. Biometric analysis included lateral and medial trochlear height (TH); cartilaginous sulcus angle (CSA); osseous sulcus angle (OSA); trochlear depth; and trochlear facet (TF) length symmetry. Sex comparisons were considered when ≥1 specimen from both sexes of the same age was available; these included 11 knees spanning 4 age groups (ages 1, 3, 4, and 7 years).
Results:
The analysis of trochlear morphology showed a lateral TH greater than the medial TH at all ages. The thickest cartilage was found on the lateral TF in the younger specimens. Regarding the development of osseous and cartilaginous trochlear contour, a cartilaginous sulcus was present in the 3-month-old specimen and continued to deepen up to the age of 4 years. The shape of the osseous center evolved from round (1 month) to oval (9 months) to rectangular (2 years); no distinct bony trochlear sulcus was present, although a well-formed cartilaginous sulcus was present. The first evidence of formation of a bony sulcus was at 4 years. By the age of 7 to 8 years, the bony contour of the adult distal femur resembled its cartilaginous contour. Female samples had a shallower CSA and OSA than did the male ones in all samples that had a defined OSA.
Conclusion:
Female trochlear grooves tended to be shallower (flatter). The lateral trochlea was higher (TH) and wider (TF length) during growth than was the medial trochlea in both sexes; furthermore, the development of the osseous sulcus shape lagged behind the development of the cartilaginous sulcus shape in the authors’ study population.
Clinical Relevance:
Bony anatomy of the trochlear groove did not match the cartilaginous anatomy in preadolescent children, suggesting that caution should be used when interpreting bony anatomy in this age group.
Introduction
Knowledge of patellofemoral (PF) joint anatomy is important to understand PF disease and injury. Specifically, a dysplastic femoral trochlea is a central risk factor for both PF instability 1,3,6,30 and PF arthritis. 11,14 The femoral trochlea is represented by the lateral and medial trochlear condyles and the sulcus between the condylar structures. Morphological changes in the medial and lateral trochlear shape, as well as the depth of the sulcus, affect the stability of the patella. Richerand, 28 in 1805, was the first to relate the symptoms of patellar “luxation” to anatomic anomalies, specifically the shape of the trochlea. Maldague and Malghem 18 reported on the proximal trochlear depth (TD) as judged on the true lateral radiograph and demonstrated that it was shallower in patients with recurrent lateral patellar dislocations. With the introduction of axial radiographs, 31 the femoral sulcus angle was a point of interest in the assessment of PF anatomic risk factors. 15,17 –19 Trochlear dysplasia has been classically described by the “crossing sign” as viewed on a true lateral radiograph. 6
More recently, using the true lateral radiograph as the gold standard, studies have described magnetic resonance imaging (MRI) criteria for trochlear dysplasia, 27 with excellent reproducibility. 3,21 The main measurements used to describe the femoral trochlea and its dysplastic variants focus on the axial view of the distal femur and compare TD to the height of the medial and lateral condyles, the lengths of the medial and lateral trochlear facets (TFs), and the lateral trochlear inclination angle. 2,5,27
There is continued debate about whether the femoral sulcus angle is largely genetically determined or is influenced by other developmental causes. Glard et al 10 studied 44 formalin preserved specimens aged 13 to 38 weeks and believed their results favored a genetic origin. Using ultrasound, Øye et al 25,26 examined 349 knees in 174 newborns and found a relationship between the knee position in utero and the cartilaginous sulcus angle (CSA), favoring some developmental component to the development of the femoral sulcus angle. Looking specifically at the CSA, 2 studies defining the sulcus via ultrasound 22 and direct inspection 33 concluded that the cartilaginous sulcus is well formed at birth and approaches its adult form, and neither found sex-based differences in trochlear measurements. An additional ultrasound study of infants aged 0 to 24 months found no difference in the femoral CSA according to side or sex. 20
This contrasts with Mundy et al, 21 who studied PF measurements in a random sample of patients aged 1 to 16 years using MRI. They found that many common PF measurements in adults can be accurately reproduced regardless of age; however, the CSA decreased as age increased. More recent studies, most with cohorts of individuals aged 8 to 18 years and adults, have found differences in some trochlear measurements because of age, 8,21,29 sex, 4 and a history of patellar instability. 3,8,30
The purpose of this study was to describe the morphology of cartilage/bony maturation of the femoral sulcus in preadolescents utilizing high-powered MRI scanners to add detail in the development of the femoral sulcus and possible sex variations in these very young specimens.
Methods
Study Population
The study population consisted of 24 knees from pediatric cadavers provided by AlloSource. The specimens were aged 1 month to 10 years and consisted of 10 male and 14 female knees. The procurement, management, and disposition of cadaveric tissue followed all institutional standards for appropriate use. Only the intact osseous morphology and cartilaginous surfaces of the knee specimens were used, with age and sex identified.
The biometric imaging measurements that were used on axial imaging slices have previously been reported. 2,3,5,10,27,30 MRI scans of the 24 specimens were analyzed; 4 age-matched pairs of both sexes were separately analyzed (ages 1, 3, 4, and 7 years). The MRI scans of 4 samples (two 2-year-old female, one 5-year-old male, and one 10-year-old female specimens) were excluded because of the low quality of the images acquired, as procurement issues of the original specimens prevented the cartilaginous detail needed for measurements. Table 1 presents the age and sex of the specimens included. Cartilage thickness was not measured in samples from individuals aged <4 years because of difficulties encountered in determining cartilaginous/osseous borders.
Age and Sex Breakdown of the Knee Specimens Included in the Study (N = 20) a

a Paired specimens.
Magnetic Resonance Imaging
Imaging of all specimens was conducted using an ultra–high field MRI scanner. 9 Smaller specimens (age, <5 years) were scanned using a small-bore animal scanner at 9.4 T (Agilent Technologies). Three-dimensional MRI scans were produced and images were reformatted; three slices in the axial/sagittal/coronal planes images were analyzed, with coronal and sagittal imaging used for image orientation. A quadrature volume transceiver coil (Millipede; Varian NMR Systems) was used for all acquisitions at 9.4 T. 23,24 The specimens were placed in test tubes immersed in perfluoropolyether to avoid susceptibility mismatch on tissue-air interfaces. MRI of larger specimens (age, ≥5 years) was performed using a whole-body human scanner at 7.0 T (Magnetom 7 T; Siemens Medical Systems) with an 8-channel transmit/receive knee coil (Virtumed LLC) driven by a B1 shimming unit (CPC) with 8- × 1-kW amplifiers. The slice thickness was 0.1 mm in all 3 dimensions on the 9.4-T MRI scanner and 0.32 mm on the 7-T scanner. Transmit B1+ shimming 12 was applied to maximize flip angle homogeneity. Respective B1+ maps were calibrated using a fast estimation technique as previously described. 12,13,16
For each specimen, the MRI biometric analysis was performed in the axial plane analyzing 3 slices (Figure 1) by an orthopaedic research resident (G.P.). The slide used corresponded to the slice with the first full cartilage coverage, consistent with other investigations. 2 –4

Image showing the sagittal, axial, and coronal planes of the slice analyzed.
The patella was absent in the majority of the specimens, and consequently patellar measurements were not performed. The biometric analysis was performed evaluating the following parameters (Figure 2):
Lateral trochlear height (TH) (A): the perpendicular line connecting the highest point of the lateral cartilaginous TF and a line tangent to the posterior femoral condyles.
Medial TH (B): the perpendicular line connecting the highest point of the medial cartilaginous TF and a line tangent to the posterior femoral condyles.
Sulcus height (C): the perpendicular line connecting the lowest point of the cartilaginous trochlear groove and a line tangent to the posterior femoral condyles.
Lateral TF length (D): the distance between the lowest point of the cartilaginous trochlear groove and the highest point of the lateral cartilaginous TF.
Medial TF length (E): the distance between the lowest point of the cartilaginous trochlear groove and the highest point of the medial cartilaginous TF.
Lateral TF angle (F): the angle formed between a first line passing through the lowest point of the cartilaginous trochlear groove and the highest point of the lateral cartilaginous TF and a second line passing through the posterior femoral condyles.
Medial TF angle (G): the angle formed between a first line passing through the lowest point of the cartilaginous trochlear groove and the highest point of the medial cartilaginous TF and a second line passing through the posterior femoral condyles.
CSA (H): 180 – (F + G).
Osseous sulcus angle (OSA) (I): the angle formed between a first line passing through the lowest point of the trochlear osseous groove and the highest point of the medial TF and a second line passing through the lowest point of the trochlear osseous groove and the highest point of the lateral osseous TF.
TD: [(A + B) ÷ 2] – C.
TF asymmetry: E ÷ D.
The OSA was not well visualized in the younger specimens and, therefore, was calculated only in specimens that were aged ≥4 years and only in the slices where the osseous form was well visualized (slices 2 and 3).
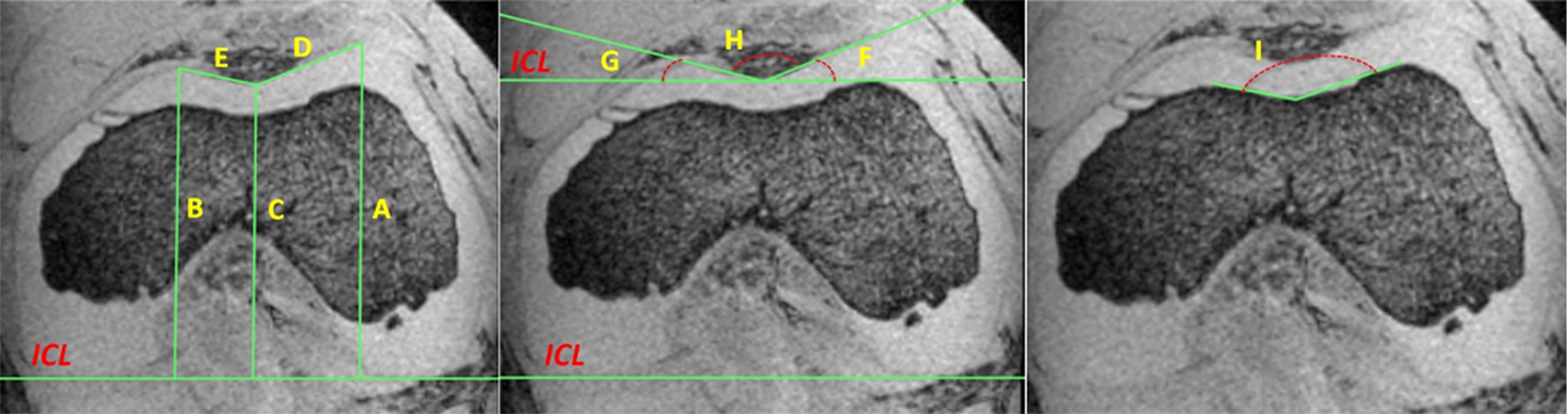
Measurements performed on each specimen. See text for full description. ICL, intercondylar line.
Results
The osseous shape changed from the youngest samples to the older samples, progressing from round (age, 1 month) to oval (age, 9 months), to rectangular (age, 2 years), to the shape of aviator glasses (age, 5 years), and to finally follow the contour of the adult distal femur (age, 7-8 years) (Figure 3). There was symmetry between the medial and lateral aspects of the osseous sulcus, which contrasted with the asymmetry of the cartilaginous tissue, resulting in thicker cartilage overlying the bone of the lateral trochlea (Figure 4, 9-month-old and 4-year-old samples). We found that after the ossification front reaches the articular cartilage and forms to the adult template, the asymmetric thickening of the epiphyseal cartilage of the lateral trochlea, when compared with the medial trochlea, has resolved and, as in the adult, the articular cartilage thickness of the medial and lateral trochlea is of equal thickness (Figure 4, 10-year-old sample).

Distal femoral epiphysis at the level of the trochlea. Representative stages of the development of the osseous shape at age 1 month (boy), 9 months (girl), 2 years (boy), 5 years (boy), and 7 years (boy).

Thickness of the trochlear cartilage among 3 different male samples, aged 9 months, 4 years, and 10 years. Cartilage thickness was not measured in those samples aged <4 years because it was challenging to recognize. The analysis of trochlear morphology showed a lateral trochlear height greater than medial trochlear height at all ages. The thickest cartilage was found on the lateral trochlear facet in the younger specimens. m.o., month old; y.o., year old.
Cartilaginous trochlear sulcus seems to be formed in early development (age, ≥3 months) and stabilizes to its adult shape at an early age (Figure 5).

Stable values of the cartilaginous sulcus angle among 3 different samples: 3-month-old girl, 4-year-old girl, and 8-year-old girl. CSA, cartilaginous sulcus angle; ICL, intercondylar line; m.o., month old; y.o., year old.
Observational differences between boys and girls were evaluated using the 4 age-matched pairs (aged 1, 3, 4, and 7 years). Girls had greater (flatter) CSAs and OSAs compared with boys. OSA was only analyzed in the 4- and 7-year-old specimens because of the lack of osseous development in the younger specimens. Girls showed a greater (shallower) average OSA than did boys in the 4-year-old specimens (Table 2). Conversely, OSA values were comparable between the 7-year-old male and female knees (Table 2).
Comparative Trends Between Male and Female Samples (n = 8) a

a Data are presented as mean ± SD. CSA, cartilaginous sulcus angle; OSA, osseous sulcus angle; TD, trochlear depth; TF, trochlear facet.
Discussion
The most important finding in this small series was that a cartilaginous trochlear sulcus is established early in development (age, ≥3 months) and continues to be present throughout development; this cartilaginous sulcus is independent of the shape of the osseous sulcus. Values of the OSA were inversely related to the age of the specimen; conversely, the CSA showed stable values across different ages. In addition, the results of the descriptive analysis of our small sample suggest a female predilection for a flatter femoral sulcus and shallower TD, which needs to be further explored in a larger sample. The study encompasses a descriptive analysis of a small sample of fresh-frozen cadaveric knees, aged 1 month to 10 years. The uniqueness of the cohort, combined with the high-quality imaging detailing previously accepted measurements for trochlear morphology, contributes to the existing knowledge of trochlear shape.
The first series to focus on the shape of the femoral trochlea in embryos was reported by Walmsley, 32 who examined fetal specimens from the 2-mm stage to full term. He concluded that the cartilaginous trochlear sulcus is already in adult form in the embryo and is well developed at birth. He also believed that the shape of the sulcus was independent of the shape of the patella. Doskocil 7 studied embryos via gross visual observation of the specimens, concluding that the lateral trochlear was higher and wider than was the medial trochlear starting in the earliest stages of development, with a corresponding asymmetry of the femoral trochlear sulcus. Both measured the external (cartilaginous) surface of the specimens only. Glard et al 10 performed a biometric evaluation of the femoral trochlea among 44 fetuses using a measurement technique similar to that used by Wanner 33 in an analysis of adults. The measurements of Glard et al were from digitized images of specimens, thereby looking at the topographic (cartilaginous) surfaces only. The results concerning the angles of both the lateral and medial TFs, as well as CSA values, were then compared with the measurements that Wanner made in adults. Glard et al found no significant difference between the patellar femoral groove in their fetal series and the adult series of Wanner. The authors concluded that the morphology of the lower femoral sulcus appears to be the same shape in fetuses and adults. Mundy et al 21 evaluated MRI measurements in 141 normal knees of patients aged 1 to 16 years with open physes and measured numerous parameters, including the CSA (not osseous). Looking specifically at the sulcus angle in those aged 1 to 8 years, they reported the sulcus angles of 149.4° to 151.7°. Sulcus angles in those aged 9 to 16 years ranged approximately 10° less (range, 138.7°-145.5°). This suggests that the cartilaginous sulcus may decrease with age; however, the values in all groups did not follow a linear pattern.
Recently, Richmond et al 29 published a descriptive analysis of 31 skeletally immature cadaveric knees (trochlea and patella; age, 2-11 years) using computed tomography (CT) scans. The authors measured both osseous and cartilaginous structure. They found an increase in the medial and lateral TH as age increases. The study also found that the shapes of the trochlea and the patella change concurrently, suggesting a correlation between these 2 structures during development. This deepening of the osseous and cartilaginous sulcus was true through age 8 years. This finding—that the shape of the trochlea and patella change concurrently as the sulcus develops—is in contrast to our findings possibly because of the lower-quality images of CT in distinguishing cartilage from osseous shape.
The abovementioned studies used slice imaging or topographic visual measurements to assess trochlear shape, largely viewed along the axial plane. Using ultrasound offers an orthogonal view. In 1994, Nietosvaara 22 conducted an ultrasonographic study among 50 normal patients aged from birth to 18 years. He concluded that OSA was inversely correlated with age while CSA was almost constant from birth to adolescence. Mizobuchi et al 20 used ultrasound to measure 80 knees of normal children aged 0 to 24 months at flexion angles of 1° to 90° and observed no significant difference with respect to knee flexion angle, with a range of 148.7° to 149.3°. These studies, with the exception of Richmond et al, 29 indicate that the cartilaginous sulcus is formed early in development, with stable values across different age groups.
Values of the OSA were inversely related to the age of the sample. Conversely, the CSA showed stable values across different ages, which is consistent with the findings of previous authors, 8,22 with a progressive flattening as the slices progress more proximal in the sulcus. With regard to a sexual dimorphism in the shape of the femoral sulcus, the literature is inconclusive. Nietosvaara 22 did not find a sex-based difference in his cohort of normal knees from 25 males and 25 females aged from birth through 18 years. Mundy et al 21 evaluated MRI measurements in a larger cohort (N = 141) and found a statistically significant sex difference in TD (0.65 mm between boys and girls) but not CSA. The difference is of doubtful clinical significance. Biedert and Bachmann 4 found a significant difference between men and women comparing the different heights of the trochlea (lateral, central, and medial) to the total width of the femoral condyle. They concluded that this difference was due to the width of the distal femur being larger in women than men with respect to the height of the trochlear measurements. Mizobuchi et al, 20 using ultrasound measurements in children aged 0 to 24 months, observed no sex-based difference in sulcus angles in their cohort of 80 knees. Øye et al 25 examined 348 knees in newborns and found a small statistical difference in sulcus angle between the sexes (male, >146.1°; female, 147.8°).
In our series, female specimens had shallower CSA and OSA with respect to male specimens; this was true for specimens of all ages sampled, including those at the earliest stages of development.
Limitations
The small sample size, with relatively large age gaps between some of the specimens, is the main weakness; the sample size was not enough to draw definitive conclusions regarding the development of trochlear morphology. Furthermore, we do not know whether these knees had a history of abnormality or were considered normal. The study lacks a statistical analysis; therefore, no significant differences among the samples can be shown.
Conclusion
This study supports earlier studies that have found that a cartilaginous trochlear sulcus is formed in early development (≥3 months) and stabilizes to its adult shape at an early age. It was independent of the shape of the osseous contour; a bony sulcus was not visualized until age 4 years or later. The bony anatomy of the trochlear groove did not match the cartilaginous anatomy in preadolescent children, suggesting that caution should be used when interpreting bony anatomy in this age group and the need for more advanced 3-dimensional imaging to more fully understand the development and degree of trochlear dysplasia in these young age groups.
This descriptive study suggests that genetically determined morphology may play a role in trochlear development. The question of possible sexual dimorphism in trochlear development remains inconclusive given our current literature.
Footnotes
Final revision submitted January 22, 2021; accepted February 24, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: Cadaveric tissue was provided by the nonprofit organization AlloSource. K.G.S. has received educational support from Arthrex and Evolution Surgical and research support from Vericel and Ossur (for the ROCK Research Group). E.A.A. has received consulting fees from Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.