
Abstract
Background:
The close proximity of the popliteal neurovascular bundle to the posterior horn of the lateral meniscus puts it at risk of compromise during lateral meniscal repair. This is particularly important in smaller pediatric patients, who are commonly treated for lateral meniscal abnormalities in isolation (discoid meniscus) or concomitantly with anterior cruciate ligament reconstruction.
Purpose:
To quantify the distance between the posterior horn of the lateral meniscus and the popliteal neurovascular bundle along the path of meniscal repair and to investigate for associations with age, sex, height, weight, body mass index (BMI), and skeletal maturity.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
A total of 144 magnetic resonance imaging scans were evaluated in a cohort of patients aged 10 to 18 years without meniscal or ligament abnormalities. Measurements were made along a line from the anterolateral portal between the popliteal neurovascular bundle and the free edge, midpoint, and meniscocapsular junctions of the posterior horn of the lateral meniscus. In addition to descriptive statistics of these distances by age and sex, analyses of variance and linear regression analyses were performed to investigate for associations with age, sex, height, weight, BMI, and skeletal maturity.
Results:
Male participants had a significantly larger mean free edge distance (14.4 ± 2.5 vs 13.1 ± 2.5 mm, respectively; P = .005) and midpoint distance (9.6 ± 2.2 vs 8.9 ± 1.8 mm, respectively; P = .011) than female participants but not a significantly larger meniscocapsular distance (5.2 ± 1.6 vs 4.6 ± 1.4 mm, respectively; P = .096). Linear regression analyses revealed significant associations between these distances and age, height, weight, and BMI (P < .001 for all). There were statistically significant pairwise differences for free edge and midpoint distances to the neurovascular bundle between patients with open and closed physes.
Conclusion:
The distance between the posterior horn of the lateral meniscus and the popliteal vasculature along a trajectory from the standard anterolateral arthroscopic portal increases linearly throughout development between the ages of 10 and 18 years. There were also significant associations between height, weight, BMI, and skeletal maturity and these anatomic distances. Knowing the safe distance to the popliteal vasculature will increase the safety of arthroscopic lateral meniscal repair in children, especially with all-inside devices that require setting the penetration depth for the advancement of a sharp delivery device beyond the posterior capsule.
The rate of knee arthroscopic surgery in children and adolescents is increasing rapidly. 10,20,44 In 2006, there were 105,733 knee arthroscopic procedures performed in the United States in children younger than 19 years compared with 61,232 performed in 1996, and this rate has continued to grow. 20 In children, meniscal tears, particularly lateral meniscal tears, are commonly treated arthroscopically, either in isolation, in the setting of a discoid meniscus, or in association with an anterior cruciate ligament (ACL) injury. 11,15,23,25,31,38,42 Despite the prevalence and minimally invasive nature of arthroscopic knee procedures, such procedures are not without a risk of complications to the patient. Potential complications include venous thromboembolism, septic arthritis, wound complications, arthrofibrosis, persistent effusion/hemarthrosis, nerve damage, and superficial wound infections. 2,5,6,36,39 One rare, albeit potentially devastating, complication is an accidental injury to the popliteal vasculature, with a reported incidence as high as between 0.5% and 1%. 9,17,26,27,34,39 The popliteal artery lies lateral to the midline and anterior to the popliteal vein. 18,21 At the distal border of the popliteal fossa, the popliteal artery passes between the 2 heads of the gastrocnemius muscle before splitting into the posterior and anterior tibial arteries as it enters the leg. 21
Vascular injuries most often occur during knee arthroscopic surgery from either direct penetration or accidental laceration. ¶ A systemic review of the literature performed in 2015 identified 39 articles and 62 individual cases of iatrogenic popliteal lesions after knee arthroscopic surgery between 1985 and 2014. 29 Of these case reports, the most common procedure that led to this complication was treatment for meniscal tears, which accounted for 53.2% of the total procedures. 29 Another literature review found 47 cases of pseudoaneurysm in arthroscopic knee procedures, 60% of which were for meniscal injuries and 23% for ACL injuries. 12 Of those 47 cases, the popliteal artery was compromised in 46%. 12
Because of the potential for popliteal neurovascular compromise, it is extremely important for orthopaedic surgeons to thoroughly understand the anatomy of the knee, especially the distance to these vessels from various anatomic landmarks, as it relates to standard anteromedial and anterolateral arthroscopic portals. 43 Previous researchers have demonstrated that the popliteal artery is, on average, 4.27 ± 0.05 mm posterior to the joint capsule at the level of the medial epicondyle, as measured in 12 cadaveric male knees with an age range between 68 and 81 years. 40 However, this relationship at the level of the joint and how it changes through development remains unclear in children. When performing arthroscopic procedures in the pediatric population, such information can better ensure that the neurovascular structures in the posterior knee joint remain at a safe distance from surgical instruments.
The purpose of the current study was to quantify the distance of the popliteal vasculature from various points of the posterior horn of the lateral meniscus, specifically at the level of the joint and along the trajectory from the anterolateral arthroscopic portal, where it is at the greatest risk of compromise. Additionally, this investigation sought to quantify how this distance changes as a function of patient age, height, weight, body mass index (BMI), and skeletal maturity.
Methods
Patient Cohort
This was an institutional review board–approved retrospective study of children aged 10 to 18 years presenting to an urban tertiary-care hospital. A review of the hospital’s picture archiving and communication system (PACS) was performed to identify eligible patients for inclusion in the study. The search criteria included all knee magnetic resonance imaging (MRI) scans obtained from March 1, 2017, to September 1, 2017, on patients between the ages of 10 and 18 years. This generated 779 unique cases. Radiologist reports were manually reviewed to exclude any participants who had a discoid meniscus, tumors, infections, previous knee surgery, motion degradation, or injuries to the meniscus, ACL, or tibia (n = 423). From the remaining cases (n = 356), 16 patients (8 male and 8 female) from each chronological age group of 10 to 18 years (total of 144 MRI scans) were randomly selected for inclusion in the final data analysis using a random number generator in Excel (Microsoft) and then choosing the first 8 numbers in each age and sex. Age 10 years was chosen as the lower age limit because a preliminary search revealed that a majority of the MRI scans at the study institution for children younger than 10 years revealed abnormal menisci, active infections, or congenital abnormalities that would affect the validity of the results.
Measurements
All MRI examinations were performed on a standard clinical 1.5-T or 3.0-T MRI scanner with 3-mm image slices (GE Healthcare), with a standardized quadrature or 8-channel knee coil (Invivo) with the knee in extension. For this investigation, a proton density axial image through the meniscus at the level of the free edge was used for all measurements . The measurement process involved making a line (Figure 1, line A) starting just lateral to the patellar tendon (simulating an anterolateral arthroscopic portal) and ending at the closest wall of either popliteal vessel. This line depicts the most direct path of instruments from the anterolateral portal to the popliteal vessels. The closest popliteal vessel was chosen, regardless of whether it was the artery or vein, because the purpose of the study was to find the shortest distance to avoid hitting any of the popliteal neurovascular structures. Next, a second line (Figure 1, line B) was drawn along line A from the anterior free edge of the posterior horn of the lateral meniscus to the closest point of the popliteal artery or vein. Finally, a third line (Figure 1, line C) was drawn, once again along line A, from the meniscocapsular junction to the closest wall of the popliteal vessels. The distances of lines B (free edge distance) and C (meniscocapsular distance) were measured and recorded by 2 investigators (J.M.S., P.D.F.). Last, the midpoint distance was calculated by taking the average of the free edge and meniscocapsular distances. These points were chosen to illustrate the range of distances from the entry of a meniscal suture needle or device from the surface of the meniscus to the popliteal neurovascular structures.

Demonstration of the methodology of measuring distance on axial magnetic resonance imaging. Line A is drawn from the anterolateral arthroscopic portal entry site to the closest point on the wall of the popliteal vessel. Line B (free edge distance) is measured along line A from the anterior free edge of the posterior horn of the lateral meniscus to the popliteal vessel. Line C (meniscocapsular distance) is measured along line A from the joint capsule to the popliteal vessel.
Clinical and Demographic Data Collection
Patient sex, age, height, weight, and BMI at the time of MRI were obtained from the medical record. The proximal tibial and distal femoral growth plates were evaluated to classify the patient as having open, closing, or closed growth plates. Physes were evaluated on both coronal and sagittal MRI scans and were considered “closed” if they were greater than 90% closed and “open” if they were greater than 90% open. The physis was considered “closing” if it was determined to be between 90% open and 90% closed.
Statistical Analysis
After visually ensuring data normality using histograms, descriptive statistics were used to report the means and SDs for continuous variables (age, height, weight, BMI) and frequencies for count variables (sex, physeal status). Linear regression analyses were performed to investigate the relationship between age, height, weight, BMI, and distances between the popliteal vessels and each of the following: the anterior free edge of the posterior horn of the lateral meniscus (Figure 1, line B), the meniscocapsular junction (Figure 1, line C), and the midpoint between the free edge and meniscocapsular junction (where meniscal sutures frequently penetrate the meniscal tissue during repair). Finally, 1-way analyses of variance with Dunnett-corrected pairwise comparisons were performed to investigate for any relationship between growth plate status and the free edge, midpoint, and meniscocapsular distances. All analyses were 2-tailed and used P = .05 as the threshold for statistical significance. Because this study was not designed as a comparative analysis between different cohorts, an a priori power calculation was not performed. 22
Results
Sixteen knees (8 male, 8 female) were analyzed for each chronological age from 10 to 18 years, resulting in a total of 144 participants (mean age, 14.5 ± 2.6 years). The mean values, across all ages, were 13.8 ± 2.3 mm for free edge distance, 9.1 ± 2.2 mm for midpoint distance, and 4.9 ± 1.5 mm for meniscocapsular distance. Male participants had a significantly larger mean free edge distance (14.4 ± 2.5 vs 13.1 ± 2.5 mm, respectively; P = .005) and midpoint distance (9.6 ± 2.2 vs 8.9 ± 1.8 mm, respectively; P = .011) than female participants but not a significantly larger meniscocapsular distance (5.2 ± 1.6 vs 4.6 ± 1.4 mm, respectively; P = .096). The mean free edge distance, midpoint distance, and meniscocapsular distance for each age group were calculated for males, females, and combined sexes, as displayed in Table 1. The results for combined sexes for each age group are presented in Figure 2, and a linear trend line was calculated. Linear regression analyses showed that age explained 18% of the variance in free edge distance (R 2 = 0.181, B = 0.38, P < .001), 16% of the variance in midpoint distance (R 2 = 0.157, B = 0.27, P < .001), and 9% of the variance in meniscocapsular distance (R 2 = 0.085, B = 0.16, P < .001).
Free Edge, Midpoint, and Meniscocapsular Distances for Each Age Group by Sex a

a Data are shown as mean ± SD.
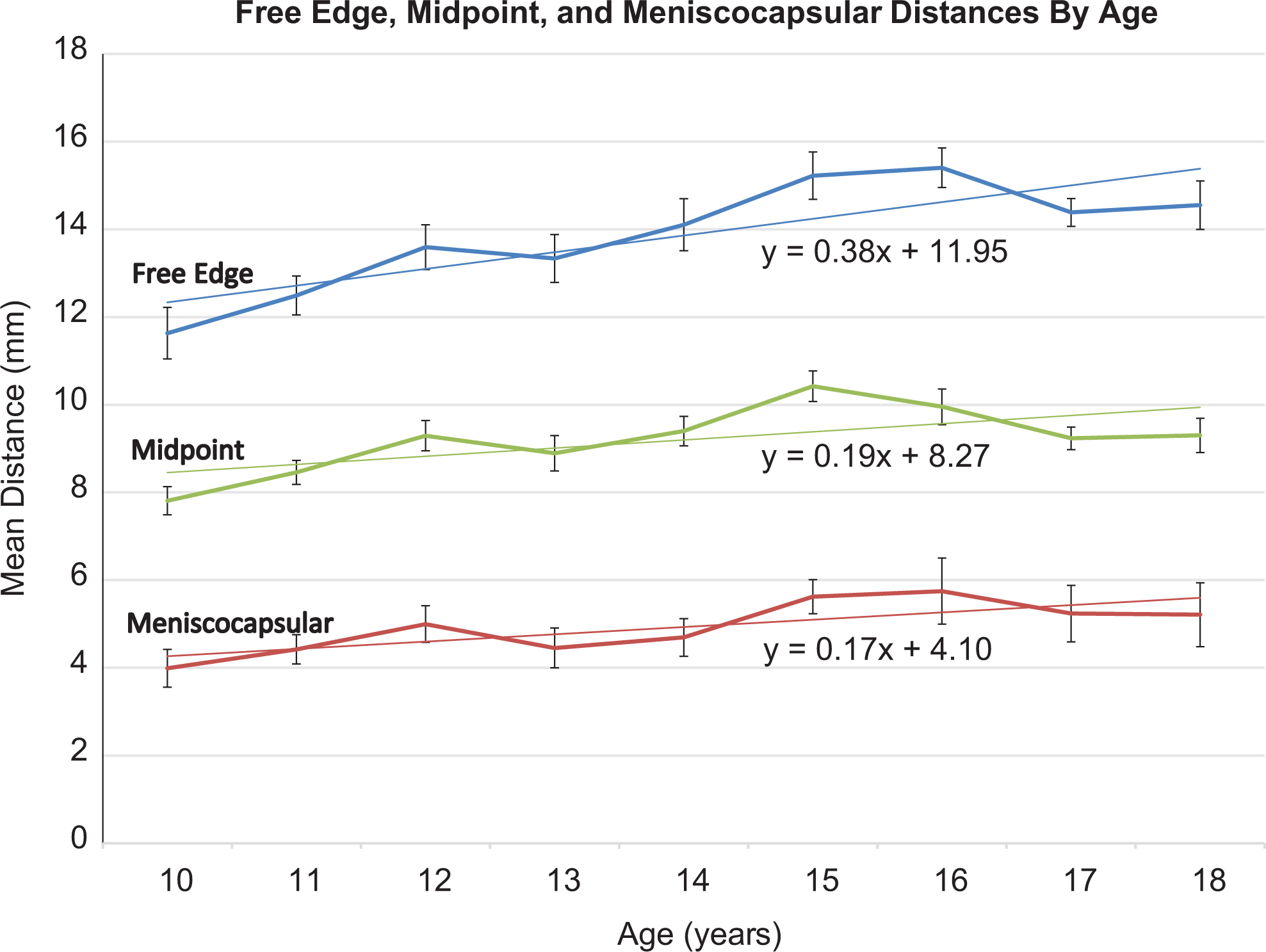
Graph of mean free edge, midpoint, and meniscocapsular distances for each age group. Linear trend lines were calculated, and the equations are shown on the graph. Error bars represent 1 SEM.
Of the 144 total participants, 118 (82%) (mean age, 14.3 ± 2.6 years) had height and weight data from an office visit within 14 days of MRI. For those 118 participants, the free edge and meniscocapsular distances were plotted relative to height (Figure 3), weight, and BMI (Figure 4), and linear regression analyses were performed. The mean height across all the participants was 163.7 ± 12.3 cm, and the mean weight was 58.5 ± 17.0 kg. The mean BMI was 21.4 ± 4.1 kg/m2. Regression analyses showed that height predicted 36% of the variance in free edge distance (R 2 = 0.36, B = 0.117, P < .001), 32% of the variance in midpoint distance (R 2 = 0.32, B = 0.083, P < .000), and 16% of the variance in meniscocapsular distance (R 2 = 0.16, B = 0.048, P < .001). Additionally, weight predicted 42% of the variance in free edge distance (R 2 = 0.42, B = 0.089, P < .001), 38% of the variance in midpoint distance (R 2 = 0.38, B = 0.065, P < .000), and 23% of the variance in meniscocapsular distance (R 2 = 0.23, B = 0.042, P < .001). Finally, BMI predicted 30% of the variance in free edge distance (R 2 = 0.30, B = 0.310, P < .001), 28% of the variance in midpoint distance (R 2 = 0.28, B = 0.234, P < .001), and 19% of the variance in meniscocapsular distance (R 2 = 0.19, B = 0.159, P < .001).

Plot of free edge distance (blue circles), midpoint distance (green “x”s), and meniscocapsular distance (red triangles) by participant height (cm). Regression lines were calculated, and the equations are shown on the graph.
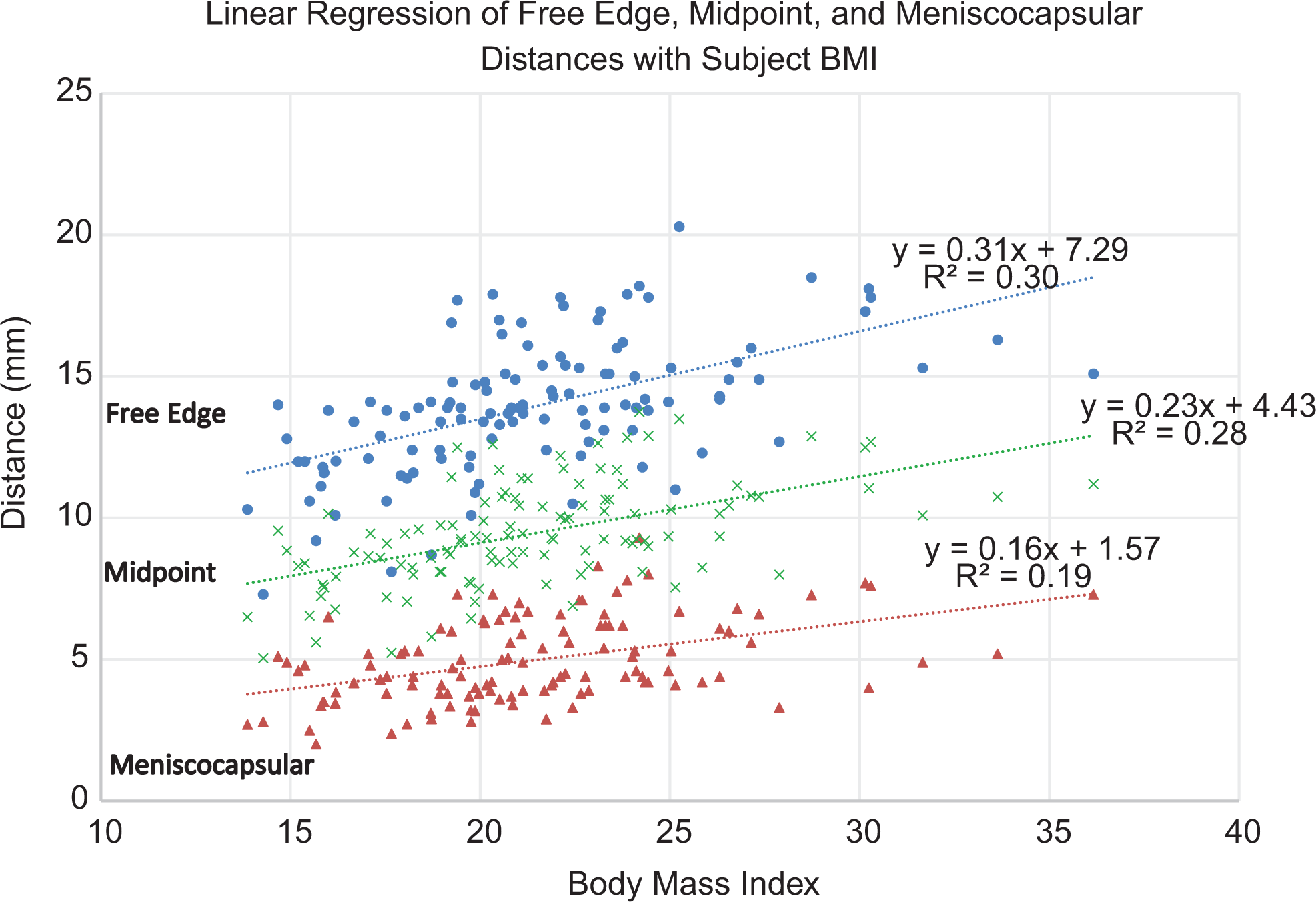
Graph of free edge distance (blue circles), midpoint distance (green “x”s), and meniscocapsular distance (red triangles) by participant body mass index. Regression lines were calculated, and the equations are shown on the graph. BMI, body mass index.
Last, the proximal tibial and distal femoral growth plates were analyzed to classify each knee as open, closing, or closed. The percentage of each growth plate status by age is displayed in Figure 5. The percentage of patients with open growth plates began decreasing at age 12 years, reaching 0% by age 17 years. The percentage with closed growth plates was 0% until age 14 years and then increased before reaching 100% by age 18 years. Participants in the closing phase were exclusively between the ages of 12 and 17 years, with a peak at age 15 years. Table 2 reports the free edge distance, midpoint distance, and meniscocapsular distance by growth plate status.

Graph of the percentage of participants within each age group with open (dotted blue line), closing (solid red line), or closed (dashed green line) growth plates by sex.
Free Edge, Midpoint, and Meniscocapsular Distances by Growth Plate Status a

a Data are shown as mean ± SD.
bP < .05 for Dunnett 2-tailed post hoc comparison with closed growth plate status.
One-way analyses of variance with Dunnett-corrected pairwise comparisons were performed to investigate for any relationship between growth plate status and the free edge, midpoint, and meniscocapsular distances. For the free edge distance, the pairwise difference between open and closed physis groups was statistically significant (mean difference, 1.6 mm; P = .001). For the midpoint distance, the difference between open and closed physis groups was statistically significant (mean difference, 0.8 mm; P = .003). For the meniscocapsular distance, no pairwise comparisons were statistically significant.
Discussion
Knee arthroscopic surgery is an increasingly common procedure in children, 10,20,44 particularly for ACL reconstruction and meniscal repair. 1,4,7,10,24,44 A sound knowledge of knee anatomy is necessary to minimize the risk of complications, which is particularly important in children and adolescents because there is a lower tolerance for errors, given their smaller anatomy. The purpose of this study was to investigate the relationship between the popliteal neurovascular bundle and the posterior capsule of the knee, specifically the distance from the meniscus along a line from the standard anterolateral arthroscopic portal, and how this is affected by clinical and demographic variables. This is especially vital when treating lateral meniscal tears, which are common in children and adolescents, both as an isolated abnormality (eg, discoid meniscal tears) and in combination with ligament reconstruction (eg, combined ACL and meniscal tears). 11,15,23,25,31,38,42
The results of the current study demonstrated that the distance between the meniscus and the popliteal vasculature increased in a linear pattern throughout development between the ages of 10 and 18 years. This upward trend was not perfectly linear, which is in part likely because of the small sample size and individual differences in each age cohort. However, age was determined to have a strong positive association with free edge, midpoint, and meniscocapsular distances. There was also a significant modest positive association between participant height, weight, and BMI and the free edge, midpoint, and meniscocapsular distances to the popliteal neurovascular bundle. It was particularly important to quantify the distances from the midpoint and meniscocapsular locations (red-white and red-red zones, respectively) to the popliteal vasculature, as suture devices are most commonly inserted in these meniscal zones. 30,35,37
Analyses of growth plate anatomy demonstrated that it was not until the age of 18 years that 100% of patients in the study cohort were skeletally mature. Because of this, physicians should not consider their patients to be fully developed until the late teenage years. These results are supported by a 2018 article in which Pennock et al 32 demonstrated the age of closure for both the proximal tibial and distal femoral growth plates. The authors found that the femoral physis was completely closed at the age of 19.8 and 18.3 years for male and female patients, respectively. 32 They also found that the tibial physis was completely closed at the ages of 19.8 and 17.2 years for male and female patients, respectively. 32 These ages are slightly older than the age that we found for 100% of participants to be closed, likely because of slight differences in the definition of terms. We defined “closed” as greater than 90% of the physis closing, while Pennock et al 32 defined it as complete physeal closure. In the current study, progressive physeal closure was significantly associated with an increase in the distance from the lateral meniscal free edge and midpoint to the popliteal neurovascular bundle.
The results of the current study can be used to increase the safety of pediatric knee arthroscopic surgery. By knowing the distance to the popliteal vessels from commonly used anatomic landmarks within the knee joint, surgeons can maintain a safe distance from the neurovascular bundle. Preliminary data from a study of a limited number of pediatric cadaveric knee specimens revealed the close proximity between the popliteal neurovascular bundle and the posterior horn of the lateral meniscus. 45 However, this is the first study, to our knowledge, to demonstrate the distance to the popliteal vessels in pediatric patients and to demonstrate how those distances change throughout puberty and skeletal development.
In knee arthroscopic surgery, 2 common portal sites, anteromedial and anterolateral, are used to allow the surgeon to access and work within the knee joint. 43 Although both are frequently used, the posterior vascular structures are too far lateral to be at risk when performing a procedure from the anteromedial portal entry site toward the medial meniscus. When viewing from the medial portal and working on the posterior horn lateral meniscus from the anterolateral portal, the risk of injuring the popliteal vessels is greater because the popliteal vessels are often directly behind the lateral meniscus in a line from the anterolateral portal. 18 This increased risk during procedures of the lateral meniscus is especially noteworthy, as research has demonstrated that lateral meniscal tears are particularly common, especially in the pediatric population. 38 One study found that of 293 pediatric patients with meniscal tears, 67% had lateral meniscal tears compared with 22% with medial tears and 11% with tears in both. 38
Although the incidence of popliteal vascular injuries during arthroscopic knee procedures is relatively low, it is still a widely reported complication. ¶ Knowing how the safe distance to the popliteal vessels changes through development and with varying heights, weights, BMIs, and skeletal maturity will allow physicians to ensure the safety of the popliteal neurovascular bundle by avoiding penetration depth with devices during surgery greater than these distances. This is even more important in pediatric knees, as the maximum preset penetration depth of several commercially available all-inside meniscal repair devices is frequently more than 20 mm, which is greater than even the largest distances from the most anterior free edge of the posterior horn of the lateral meniscus to the popliteal neurovascular bundle noted in the current study (15 mm).
Despite its strengths, this study contains a number of potential limitations. One such limitation is that all distance measurements were performed in individual patients and associated by age. While it would be more methodologically sound to longitudinally follow patients and investigate changes in these distances over time, such a study would be economically and logistically unfeasible, and therefore, the current study methodology using a cross-sectional design is more appropriate. Another limitation is that no multivariable regression analysis was conducted to determine independent or best predictors of the measured distances because of the high level of collinearity between the predictor variables. Therefore, the predictors noted in the current study should not be thought of as independent predictors of the measured distances but rather that they are associated with these distances.
Additionally, the distances were measured linearly on axial slices, where the meniscus was most clearly visible, with the knee in extension. This does not account for (1) the increasing distance between the joint and neurovascular bundle in flexion, which is the position most frequently used for lateral meniscal repair (figure-of-4 position); (2) the distance in the proximal-distal (axial) plane; and (3) the use of curved meniscal fixation implant devices. However, because each of these factors would effectively increase the distance traveled between the meniscus and neurovascular bundle, the measurements made here are, if anything, an underestimate of this distance and therefore provide the safest (shortest) estimate of the penetration/laceration distance. Furthermore, MRI was performed with the knee in full extension, while lateral meniscal repair is typically performed with the knee flexed in the figure-of-4 position. Knee flexion typically results in the vessel moving away from the posterior capsule, so again, this study provides a more cautious estimate of the penetration/laceration distance. 19,28 Finally, we did not examine how other physical factors such as varus or valgus alignment would affect the penetration distance. Factors other than those investigated here may affect the penetration distance and could be the subject of future investigation.
Conclusion
There was a strong positive association between age and the distance from various points on the posterior horn of the lateral meniscus and the popliteal vasculature when measured along a line from the standard anterolateral arthroscopic portal. Furthermore, there was a significant association between these anatomic distances and patient height, weight, BMI, and skeletal maturity. It is important to know these distances to appropriately set the meniscal suture implant penetration depth and reduce the chance of intraoperative vascular compromise during arthroscopic knee surgery, particularly when viewing through a medial portal and working through the anterolateral portal. Before any meniscal repair, the individual patient’s MRI scan must be studied carefully to discern the exact location and distance of the popliteal vessels from the meniscus and posterior capsule. Taken together with the results of the current study, this will maximize safety during arthroscopic lateral meniscal repair in children and adolescents.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: Y.-M.Y. is a paid consultant for OrthoPediatrics and Smith & Nephew. K.G.S. has received research support from AlloSource and Vericel, is an unpaid consultant for Clinical Data Solutions and SourceTrust, is a paid consultant for HealthTrust, and has received hospitality payments from DePuy and Sanofi-Aventis. D.W.G. receives royalties from Arthrex, Pega Medical, and Wolters Kluwer Health; is a paid consultant for Arthrex; and is a paid speaker/presenter for Synthes. P.D.F. has received educational support and hospitality payments from Smith & Nephew and Medical Device Business Services. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Hospitality for Special Surgery Institutional Review Board (No. 29079).