
Abstract
Background:
The optimal timing of surgical intervention for multiligament knee injuries remains controversial.
Purpose:
To review the clinical and functional outcomes after acute and delayed surgical intervention for multiligament knee injuries.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
We performed a search of the PubMed, Embase, Cochrane Library, and Web of Science databases from inception to September 2020. Eligible studies reported on knee dislocations, multiligament knee injuries, or bicruciate ligament injuries in adult patients (age, ≥18 years). In addition to comparing outcomes between acute and delayed surgical intervention groups, we conducted 3 subgroup analyses for outcomes within isolated knee injuries, knee injuries with concomitant polytrauma/fractures, and high-level (level 2) studies.
Results:
Included in the analysis were 31 studies, designated as evidence level 2 (n = 3), level 3 (n = 8), and level 4 (n = 20). These studies reported on 2594 multiligament knee injuries sustained by 2585 patients (mean age, 25.1-65.3 years; mean follow-up, 12-157.2 months). At the latest follow-up timepoint, the mean Lysholm (n = 375), International Knee Documentation Committee (IKDC) (n = 286), and Tegner (n = 129) scores for the acute surgical intervention group were 73.60, 67.61, and 5.06, respectively. For the delayed surgical intervention group, the mean Lysholm (n = 196), IKDC (n = 172), and Tegner (n = 74) scores were 85.23, 72.32, and 4.85, respectively. The mean Lysholm (n = 323), IKDC (n = 236), and Tegner (n = 143) scores for our isolated subgroup were 83.7, 74.8, and 5.0, respectively. By comparison, the mean Lysholm (n = 270), IKDC (n = 236), and Tegner (n = 206) scores for the polytrauma/fractures subgroup were 83.3, 64.5, and 5.0, respectively.
Conclusion:
The results of our systematic review did not elucidate whether acute or delayed surgical intervention produced superior clinical and functional outcomes. Although previous evidence has supported acute surgical intervention, future prospective randomized controlled trials and matched cohort studies must be completed to confirm these findings.
Multiligament knee injuries can be defined as the disruption of at least 2 of the 4 primary knee ligaments and can result from dislocations of the tibiofemoral joint. Knee dislocations are uncommon pathologies, accounting for less than 0.02% of all orthopaedic injuries. 17,21,27,44,46 Many have postulated that the reported incidence of knee dislocations underestimates the true burden of these injuries as a result of spontaneous reductions and missed diagnoses during the initial examination. 6,44,56 Multiligament knee injuries and knee dislocations are devastating and potentially life-threatening. Amputation of the lower limb has an incidence of 12% after knee dislocation and is a feared outcome associated with these pathologies because of concomitant vascular injury to the popliteal artery. 37
As a result of the complexity of multiligament knee injuries, their associated complications, and low rate of occurrence, the proper treatment strategy and the timing of surgical intervention remains controversial. Acute surgical intervention within the first 3 weeks after injury has been supported by many authors and surgeons because of reported improvements in functional and clinical outcomes 15,24,31 –33,55 without compromising the range of motion when early postoperative mobilization protocols were utilized. 50 Moreover, surgical intervention has been recommended within 3 weeks of injury before significant scar formation 15,33,55 and also has been shown to reduce the risk of articular cartilage and meniscal injuries. 33,51 On the other hand, delayed surgical intervention has been supported because of improved preoperative knee range of motion, extra-articular structure healing, and recovery of associated soft tissues injuries. 10,11,28,31,49,51
This lack of consensus within the literature has been examined in previous systematic reviews; however, studies with skeletally immature patients were included, 19,31,50 cases with associated polytraumatic injuries or fractures were excluded, 19 and only the most severely classified injuries were examined. 40 Therefore, the main purpose of this systematic review was to examine whether acute or delayed surgical intervention would result in superior clinical and functional outcomes in patients at least 18 years of age sustaining knee dislocations, multiligament knee injuries, or bicruciate ligament injuries. A secondary focus of our review was to complete a subgroup analysis between an isolated injury cohort and concomitant polytrauma/fracture cohort to further examine how these factors affect surgical timing and outcome measures. It was hypothesized that acute surgical intervention would result in superior clinical and functional outcomes in our study population.
Methods
Literature Search
The PubMed, Embase, the Cochrane library, and Web of Science databases were systematically searched for studies published from inception to September 2020. The Boolean search terms and operators used are as follows: (“knee dislocation”) OR (“multi-ligament” AND “knee” AND [“injury” OR “reconstruction” OR “repair” OR “surgical management”]) OR (“traumatic” AND “knee” AND [“dislocation” OR “ligament repair”]). The current systematic review was conducted according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines.
Eligibility Criteria
Studies were eligible for inclusion if they met the following criteria: (1) full-text publications reporting surgical treatment, reconstruction or repair, and outcomes of knee dislocations, multiligament knee injuries, or bicruciate ligament injuries in patients 18 years and older; (2) total sample size >10 patients; and (3) studies published in English. Publications were excluded if patients presented with an injury to fewer than 2 ligaments, with isolated patellar or tibiofibular dislocations, after total knee arthroplasty as well as if insufficient demographic detail was provided. All review articles, meta-analyses, editorials, commentaries, case reports, biomechanical studies, book chapters, epidemiological/incidence reports, and technical notes were excluded.
Study Selection and Data Extraction
After duplicate article exclusion, titles and abstracts were screened by 1 investigator (R.S.M.) according to the inclusion criteria. A full-text review was performed to further determine eligibility on all studies included after the screening process and on any studies in which uncertainty was encountered. All relevant data from eligible studies were independently extracted by the same single investigator. The information (if reported) retrieved from each publication included (1) general study information (author, title, year, journal of publication, and study design); (2) characteristics data (sample size, age, and sex); (3) injury data (laterality, velocity, mechanism, and Schenck classification); (4) timing of surgery and follow-up; (5) graft type utilized during surgery; and (6) outcomes reported (objective, subjective, and concomitant injuries). Based on operative timing definitions used in previous studies, 15,31,53,55 cases treated within the first 3 weeks of injury were defined as acute. All other cases treated after the 3-week time period were defined as delayed. In addition to the analysis of all 31 included articles, 3 subgroup analyses (isolated knee injuries, knee injuries with concomitant polytrauma/fractures, and high-level studies [level of evidence 2]) were completed. The isolated injuries subgroup included patients who sustained knee dislocations and bicruciate/multiligament knee injuries (1) without concomitant injuries and (2) with concomitant damage limited to meniscal, articular cartilage, neural, or vascular structures. The concomitant polytrauma/fractures subgroup included all other cases where polytrauma/fractures were associated with the clinical presentation. The high-level studies subgroup analysis was based on cutoffs within the literature that defined "high levels of evidence” as publications that were reported to have level 1 and 2 designations. 7,12 No statistical analyses were completed because of the inherent heterogeneity of the patient population included in this systematic review.
Results
Study Selection and General Characteristics
Our online database search yielded a total of 4506 publications (1330, 2367, 44, and 765 reports in PubMed, Embase, Cochrane Library, and Web of Science, respectively) as well as 1 additional record obtained from other sources. Of those, 231 were selected for further evaluation. Ultimately, after full-text reading and analysis, 31 studies § met all the eligibility requirements and were included in our systematic review. The PRISMA flowchart is shown in Figure 1.

PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flowchart summarizing the literature search, screening, and review of eligible articles. MRI, magnetic resonance imaging; PCL, posterior cruciate ligament.
All studies were published over a 21-year period between 1999 and 2020, reporting on 2594 knee dislocations, multiligament knee injuries, or bicruciate knee injuries sustained by 2585 patients. Of the 31 publications, 5 of these 4,5,8,48,52 did not report the timing from injury to surgical repair/reconstruction of the cruciate ligaments. Based on each study’s stated mean time to surgery, 10 studies ∥ reported outcomes for acute surgical intervention, 8 studies 1,3,14,26,30,34 –36 reported outcomes for delayed surgical intervention, and 8 studies 16,32,38,39,41,53,57,58 included outcomes on both. According to sex distributions and male-to-female ratios, all but 2 studies 1,48 reported that men represented the majority in each cohort of patients. The mean age ranged from 25.1 to 65.3 years with a mean follow-up time ranging from 12 to 157.2 months. Additional general characteristics of the included studies are summarized in Appendix Table A1.
Analysis of Included Studies
The majority of the included studies (64.52%) were retrospective case series by design, which corresponds to a level 4 evidence designation (Appendix Table A1). The remaining studies were divided among evidence level 2 (9.68%) and level 3 (25.81%). Of the 31 studies, 7 did not report the surgical intervention utilized, 3,5,8,9,38,48,52 while autografts were the most highly reported graft used for anterior cruciate ligament (ACL) reconstruction (12 studies), ¶ and autografts # and allografts** were the most highly reported graft used for posterior cruciate ligament (PCL) reconstruction (9 studies each). The most commonly reported outcome measures were the Lysholm knee scoring scale (70.97%), International Knee Documentation Committee subjective knee evaluation form (IKDC) (61.29%), range of motion (ROM) (54.84%), and Tegner activity score (51.61%). Based on the reported values, the mean Lysholm (n = 375), IKDC (n = 286), and Tegner (n = 129) scores for patients who underwent acute surgical intervention were 73.60, 67.61, and 5.06, respectively. For the delayed surgical intervention group, the mean Lysholm (n = 196), IKDC (n = 172), and Tegner (n = 74) scores were 85.23, 72.32, and 4.85, respectively. The total number of reported concomitant peroneal nerve and vascular injuries for the acute surgical intervention group were 68 (19.2%) and 29 (16.1%), respectively. For the delayed surgical intervention group, the total number of reported concomitant peroneal nerve and vascular injuries were 32 (23.4%) and 27 (19.7%), respectively.
Isolated Knee Injuries Subgroup Analysis
Seventeen studies †† were included in our isolated knee injuries subgroup analysis. The Lysholm, IKDC, and Tegner scores for the entire isolated subgroup are listed in Appendix Table A2. Based on the reported values, the mean Lysholm (n = 323), IKDC (n = 236), and Tegner (n = 143), scores were 83.7, 74.8, and 5.0, respectively. The total number of common peroneal nerve and vascular injuries were 125 (7.3%) and 236 (13.9%), respectively. Table 1 contains the concomitant peroneal nerve and vascular injury data for the entire isolated subgroup. The mean ROM at the final follow-up and the number of patients with flexion limitations of 5° to 15° for all studies included in the isolated subgroup are summarized in Table 2.
Concomitant CPN and Vascular Injuries in the Isolated Knee Injuries Subgroup a

a CPN, common peroneal nerve; NR, not reported
b Calculated using entire cohort of patients before exclusion criteria.
c Patients were removed from the study based on exclusion criteria.
ROM in the Isolated Knee Injuries Subgroup a
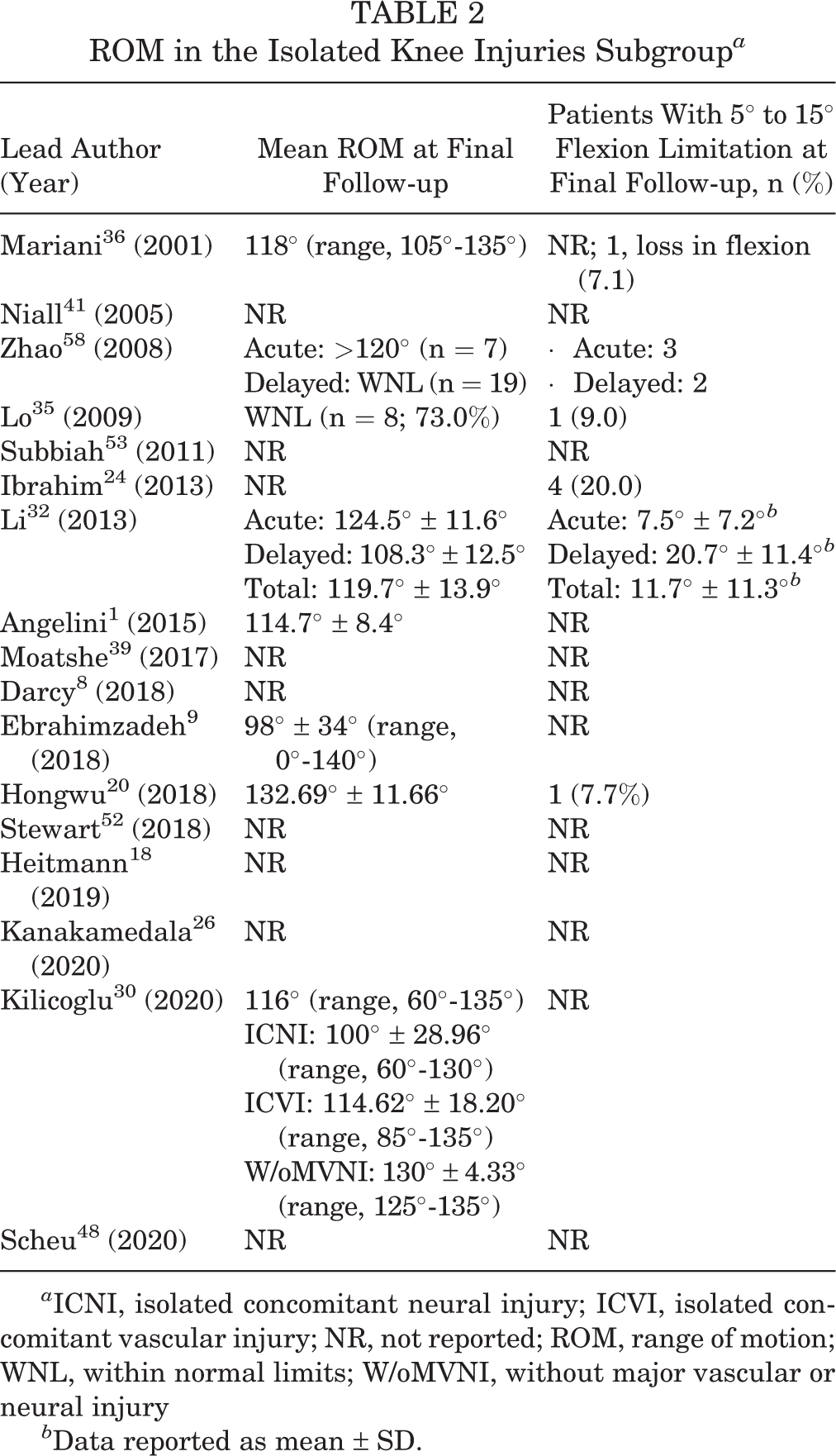
a ICNI, isolated concomitant neural injury; ICVI, isolated concomitant vascular injury; NR, not reported; ROM, range of motion; WNL, within normal limits; W/oMVNI, without major vascular or neural injury
b Data reported as mean ± SD.
Concomitant Polytrauma/Fractures Subgroup Analysis
Sixteen studies ‡‡ were included in our polytrauma/fractures subgroup analysis. The Lysholm, IKDC, and Tegner scores for the entire subgroup are summarized in Table 3. The mean Lysholm (n = 270), IKDC (n = 236), and Tegner (n = 206) scores for the polytrauma/fracture subgroup were 83.3, 64.5, and 5.0, respectively. The total number of concomitant peroneal nerve and vascular injuries is provided in Table 4. The total number of common peroneal nerve and vascular injuries were 151 (17.4%) and 71 (9.5%), respectively. The mean ROM at the final follow-up and the number of patients with flexion limitations of 5° to 15° for all studies included in the polytrauma/fractures subgroup are summarized in Table 5.
Lysholm, Tegner, and IKDC Scores in the Concomitant Polytrauma/Fractures Subgroup a
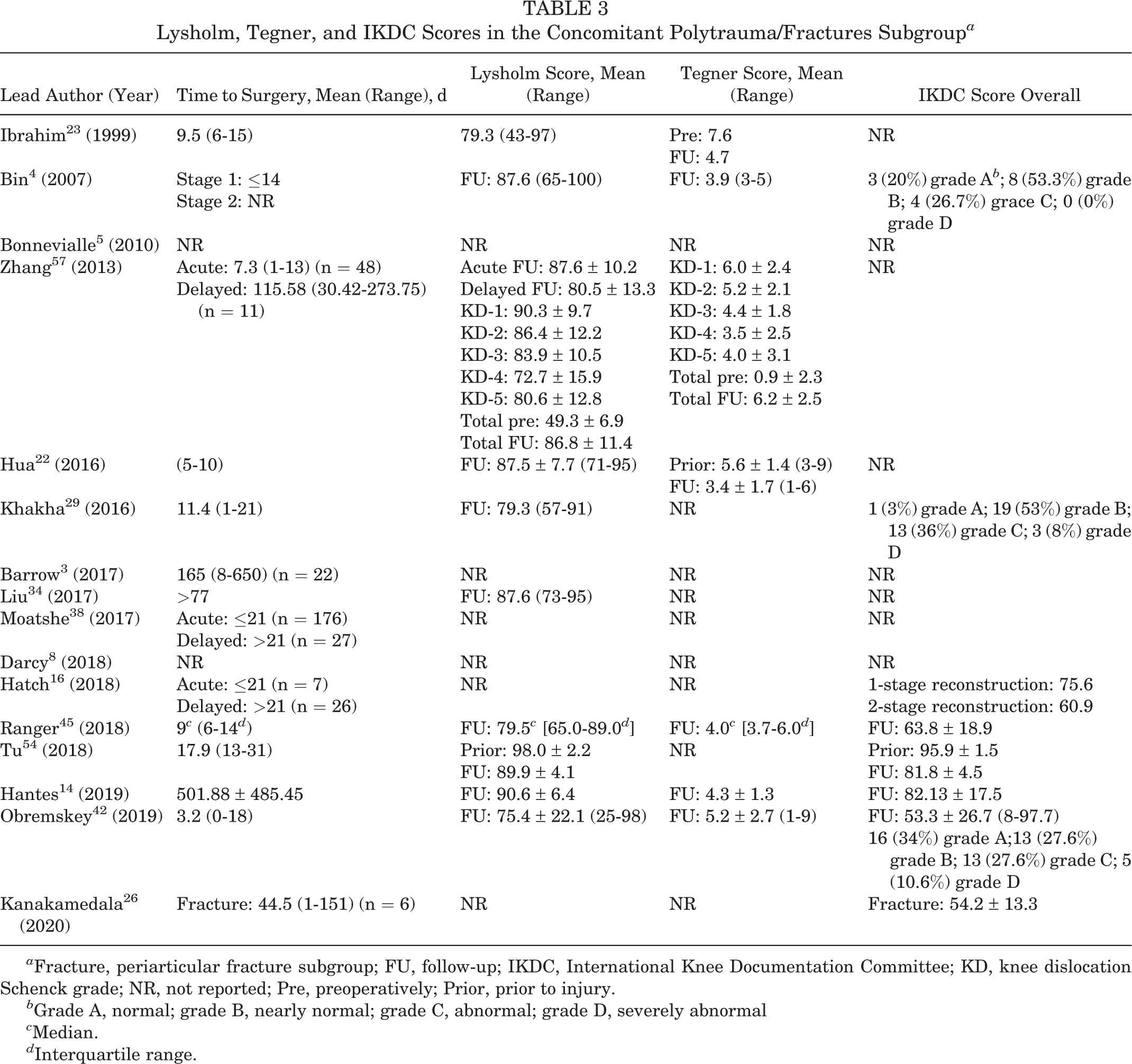
a Fracture, periarticular fracture subgroup; FU, follow-up; IKDC, International Knee Documentation Committee; KD, knee dislocation Schenck grade; NR, not reported; Pre, preoperatively; Prior, prior to injury.
b Grade A, normal; grade B, nearly normal; grade C, abnormal; grade D, severely abnormal
c Median.
d Interquartile range.
Concomitant CPN and Vascular Injuries in the Concomitant Polytrauma/Fractures Subgroup a
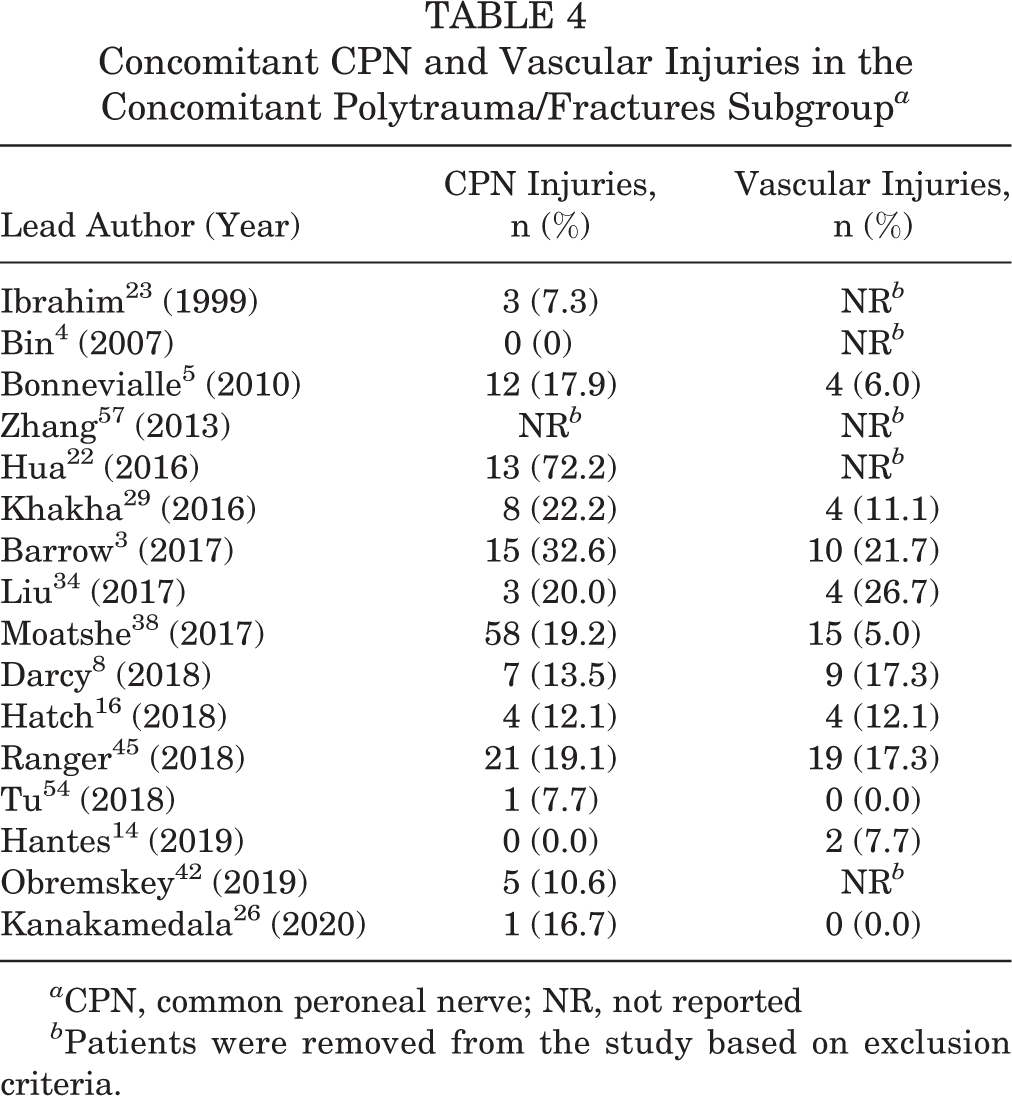
a CPN, common peroneal nerve; NR, not reported
b Patients were removed from the study based on exclusion criteria.
ROM in the Concomitant Polytrauma/Fractures Subgroup a

a AROM, active range of motion; NR, not reported; PROM, passive range of motion; ROM, range of motion; RTD, return to duty; Separated, separated from duty; WNL, within normal limits.
b Median.
c Interquartile range.
Subgroup Analysis of High-Level (Level of Evidence 2) Studies
Three studies 18,29,35 were included in the high-level studies subgroup analysis. Lo et al 35 was the only high-level study to report outcomes for delayed surgical intervention. The mean Lysholm score (n = 11), percentage of patients within IKDC grade A (normal)/grade B (nearly normal) (n = 11), and mean Tegner score (n = 11) for delayed intervention were 88, 82%, and 6.2, respectively. In comparison, the Lysholm (n = 105), IKDC (n = 105), and Tegner (n = 69) scores for acute surgical intervention were 80.42, 75.75, and 5.0, respectively. The total number of common peroneal nerve and vascular injuries was 19 (18.10%) and 4 (11.1%), respectively, for acute surgical intervention among the high-level studies subgroup. These values were not reported for delayed surgical intervention among the high-level studies subgroup.
Discussion
The results of our systematic review suggest that there is insufficient evidence to determine whether acute or delayed surgical intervention produces superior clinical and functional outcomes in patients who sustained multiligament knee injuries. Barfield et al 2 also concluded that evidence was lacking when examining acute versus staged treatment for multiligament knee injuries in 2015. Our reported mean IKDC and Tegner scores provide inconclusive evidence concerning whether acute or delayed surgery should be utilized as the superior therapeutic intervention for patients who are recovering from multiligament knee injuries. In contrast, the mean Lysholm scores showed quantitative (73.60 vs 85.23) and qualitative (fair vs good outcomes) variation in favor of the delayed surgical intervention cohort. In 2015, Jiang et al 25 reported that there was not a statistically significant difference between acute and delayed surgical intervention cohorts based on IKDC and Lysholm scores. These results simultaneously support and refute the results of our current systematic review. In addition, our results seem to diverge from those of other previous systematic reviews, meta-analyses, and journal articles 15,31,33,40,50,55 that concluded that acute surgical intervention may result in superior clinical and functional outcomes in comparison with delayed intervention. One possible explanation for the divergence in these results may be because of our exclusion of patients under the age of 18 years. Hohmann et al, 19 Levy et al, 31 and Sheth et al 50 all included skeletally immature patients in their systematic reviews, which could have affected the clinical and functional outcomes favoring acute surgical intervention. Although the decision to exclude skeletally immature patients is an arbitrary cutoff, our systematic review attempted to limit the potential bias of analyzing outcomes in both skeletally mature and immature patients. In addition, the results of Barfield and colleagues’ systematic review in 2015, which included patients between 23.5 and 45.5 years of age, reported results that align with our current conclusion that evidence to suggest superiority of either treatment strategy remains insufficient. Another explanation for this lack of consensus with previous systematic reviews may be because of another aspect of our inclusion criteria: severity of injury. Mook et al 40 only included the most severe multiligament knee injuries based on the Schenck knee-injury classification system, 47 whereas our review included patients from all levels of severity. This difference in patient selection based on injury severity may help explain the inconsistency among our results and previous studies.
Our subgroup analysis between isolated knee injuries and knee injuries with concomitant polytrauma/fractures did not produce conclusive evidence concerning clinical and functional outcomes. The Lysholm and Tegner scores for both groups were nearly identical, whereas the mean IKDC scores suggested a potential difference in function and activity in favor of the isolated subgroup. In comparison with the reported frequency of nerve (18%) and vascular (25%) injuries associated with knee dislocations, 37 both the isolated and polytrauma/fracture subgroups reported lower rates of occurrence. This could be explained by the wide range of frequencies reported within the literature and the difference of opinion regarding the proper diagnostic evaluation of vascular injuries (eg, routine angiography, selective angiography, or ankle-brachial indexes). 13,43 In addition, the heterogeneity among mechanism, velocity, and classification of injury among studies and cohorts of patients can cause the frequency of nerve and vascular injuries to vary and fluctuate accordingly. 37
This systematic review is not without limitations and weaknesses. First, the majority of the studies included in our analysis were retrospective case series with a level 4 evidence designation. The low methodological quality of these studies, lack of randomization, and lack of control groups used for comparison limits the quality and clinical utility of our results. Even the results of our high-level studies subgroup analysis remained inconclusive. It is apparent that future studies with higher methodological quality are necessary to clarify whether acute or delayed surgical intervention is superior. Second, there was an inherent amount of heterogeneity that existed among the patient characteristics, injury characteristics (laterality, mechanism, velocity), and surgical technique utilized within the included studies. In addition, the reporting of outcomes and results was inconsistent among studies, which may have affected the synthesis of data within our analysis. For these 2 reasons, the generalizability and clinical utility of the reported outcomes must be interpreted with caution. Last, the Lysholm and IKDC scores have not been validated as outcome measures for multiligament knee injuries, yet both have been utilized across the board as measures of functional and clinical improvement in patients. This lack of reliability in the 2 most frequently utilized outcome measures within our systematic review further limits the clinical utility of our results and reinforces the controversy that exists concerning the timing of surgical intervention for multiligament knee injuries. However, the major strength of our study stems from our methodological and in-depth analysis of the current literature pertaining to multiligament knee injuries and the timing of surgical intervention.
Conclusion
Multiligament knee injuries are complex orthopaedic pathologies. Because of this inherent complexity and the rarity of multiligament knee injuries, the proper treatment protocol concerning timing of surgical intervention (acute vs delayed) remains controversial. This systematic review attempted to determine whether acute or delayed surgical intervention would result in superior clinical and functional outcomes for patients at least 18 years of age; however, our review concluded that there is insufficient evidence to make this determination remains at this time. Future studies must focus on improving their methodological quality by performing prospective, randomized controlled studies or prospective cohort studies with patient matching for characteristics, injury severity, and surgical technique.
Footnotes
Notes
Final revision submitted February 18, 2021; accepted March 2, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: B.A.Z. has received nonconsulting fees and honoraria from Vericel and hospitality payments from Arthrosurface. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Appendix
Lysholm, Tegner, and IKDC Scores in the Isolated Knee Injuries Subgroup a

| Lead Author (Year) | Mean Time to Surgery (Days, Range) | Mean Lysholm Score (Range) | Mean Tegner Score (Range) | Overall IKDC Score b |
|---|---|---|---|---|
| Mariani 36 (2001) | 105 (5-190) | Pre: 65.5 ± 9.1 (48-78) FU: 95.1 ± 4.5 (88-100) |
Prior: 6.9 ± 1.7 (4-9) FU: 5.5 ± 1.6 (2-9) |
NR |
| Niall 41 (2005) | Acute: ≤4 (n = 10) Delayed: >21 (n = 3) |
NR | NR | NR |
| Zhao 58 (2008) | Acute: ≤21 (n = 7) Delayed: 273.75 (91.25-577.92) (n = 14) |
Total FU: 91.9 ± 4.2 Delayed pre: 64.9 ± 4.7 Delayed FU: 92.7 ± 3.9 |
Total prior: 6.2 ± 1.8 Total FU: 5.0 ± 1.9 Delayed pre: 1.6 ± 1.4 Delayed FU: 5.1 ± 1.6 |
Total FU: 85.5 ± 5.8 Delayed pre: 46.1 ± 5.7 Delayed FU: 87.4 ± 6.1 |
| Lo 35 (2009) | 76 (30-150) | Pre 34 ± 12 (22-74) FU: 88 ± 5.8 (76-95) |
Prior: 7.0 ± 1.6 (5-9) Pre: 3.1 ± 1.6 (2-5) FU: 6.2 ± 2.0 (3-9) |
Pre: 0% grade A/B; 100% grade C/D FU: 82% grade A/B; 18% grade C/D |
| Subbiah 53 (2011) | Acute: 5.4 (1-14) (n = 11) Delayed: 127.74 (30.42-547.50) (n = 8) |
Acute FU: 93 Delayed FU: 90 Total FU: 92 ± 7 |
NR | 0 (0%) grade A; 15 (79%) grade B; 2 (10.5%) grade C; 2 (10.5%) grade D |
| Ibrahim 24 (2013) | >15 (15-21) | FU: 90 ± 2 (75-95) | Prior: 8-9 (n = 5); 6-7 (n = 11); 5-6 (n = 4) FU: 4-7 (n = 5); 5-7 (n = 11); 4-5 (n = 4) |
0 (0%) grade A; 9 (45%) grade B; 9 (45%) grade C; 2 (10%) grade D |
| Li 32 (2013) | Acute: 10.5 ± 6.9 (n = 6) Delayed: 186.5 ± 140.1 (n = 9) |
Acute FU: 87.7 ± 5.6 Delayed FU: 82.1 ± 6.4 Total FU: 84.3 ± 5.7 |
Delayed prior: 4.9 ± 0.6 Delayed FU: 3.4 ± 0.5 Total prior: 5.1 ± 0.6 Total FU: 3.6 ± 0.5 |
Acute: 3 (50%) grade A; 1 (16.7%) grade B; 2 (33.3%) grade C; 0 (0%) grade D · Delayed: 2 (22.2%) grade A; 3 (33.3%) grade B; 1 (11.1%) grade C; 3 (33.3%) grade D |
| Angelini 1 (2015) | 76.95 | FU: 81.5 ± 12.2 (49-95) | NR | FU: 71.7 ± 13.3 (37.9-90.8) 0 (0%) grade A; 10 (71.4%) grade B; 3 (21.4%) grade C; 1 (7.1%) grade D |
| Moatshe 39 (2017) | Acute: 10 (8-13
c
) (n = 33) Delayed: 279 (133-628 c ) (n = 32) |
Acute: 86.9 ± 15 Delayed: 81 ± 19 Total: 84 ± 17.2 |
Acute: 4
d
(3-4.25
c
) Delayed: 4 d (3-5 c ) Total: 4 d (3-5 c ) |
Acute: 75.6 ± 19.5 Delayed: 70.5 ± 18.3 Total: 73 ± 18.9 |
| Darcy 8 (2018) | NR | NR | NR | NR |
| Ebrahimzadeh 9 (2018) | 11 (0-90) | 68 (18-100) | NR | NR |
| Hongwu 20 (2018) | 1.84 (1-3) | Pre: 1.53 ± 2.40 FU: 83.53 ± 6.64 |
Pre: 0 ± 0 FU: 4.84 ± 0.89 |
Pre: 8.56 ± 1.80 FU: 75.42 ± 3.86 |
| Stewart 52 (2018) | NR | NR | NR | NR |
| Heitmann 18 (2019) | 7.3 ± 1.6 | Total FU: 81.0 ± 15.5 CPN FU: 65.6 ± 26.3 · ULV FU: 31.3 ± 7.1 Without CPN or ULV FU: 85.6 ± 5.6 |
Total prior: 6 (3-8) Total FU: 5 (1-7) CPN prior: 5 (3-7) CPN FU: 4 (1-6) ULV prior: 4 (3-4) ULV FU: 2.5 (1-3) Without CPN or ULV Prior: 6 (3-8) Without CPN or ULV FU: 5 (3-7) |
Total FU: 75.5 ± 14.5 9 (13%) grade A; 29 (42%) grade B; 22 (32%) grade C; 9 (13%) grade D |
| Kanakamedala 26 (2020) | Control: 63.8 (0-306) (n = 12) | NR | NR | Control: 74.0 ± 19.6 |
| Kilicoglu 30 (2020) | Collateral ligaments: <7 Cruciate ligaments: (21-180) |
Total: 80 (40-100) KD-1: 75 (59-95) KD-2: 64 (40-90) KD-3: 88 (75-100) KD-4: 78 (59-95) KD-5: 75 (59-95) ICNI: 68.40 ± 17.17 (40-95) ICVI: 77.69 ± 12.45 (59-100) W/oMVNI: 90.53 ± 5.97 (82-100) |
NR | Total: 72 (32-89) KD-1: 70 (57-84) KD-2: 58 (32-85) KD-3: 79 (65-89) KD-4: 70 (48-86) KD-5: 70 (57-84) ICNI: 60.60 ± 16.01 (32-84) ICVI: 71.54 ± 9.20 (57-88) W/oMVNI: 82.12 ± 5.25 (70-89) |
| Scheu 48 (2020) | NR | NR | NR | NR |
a CPN, common peroneal nerve subgroup; FU, follow-up; ICNI, isolated concomitant neural injury; ICVI, isolated concomitant vascular injury; IKDC, International Knee Documentation Committee; KD, knee dislocation Schenck grade; NR, not reported; Pre, preoperatively; Prior, prior to injury; ULV, ultra-low velocity subgroup; W/oMVNI, without major vascular or neural injury.
b Grade A, normal; grade B, nearly normal; grade C, abnormal; grade D, severely abnormal.
c Interquartile range.
d Median.