
Abstract
Background:
Repetitive microtrauma may contribute to osteochondritis dissecans (OCD) lesions of the femoral condyle. The effect of differential loading between OCD weightbearing (WB) zones has not been studied.
Purpose:
To determine whether clinical and radiographic variables differ by WB zone in lateral femoral condyle OCD lesions.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
We retrospectively reviewed a consecutive series of patients aged
Results:
A total of 62 lateral femoral condyle OCD lesions (mean follow-up, 24.1 months) presented within the study period: 26 WB lesions and 36 nonweightbearing (NWB) lesions. At presentation, no differences between the lesion types were observed in symptom chronicity or symptomatology. NWB lesions were deeper on MRI scans (sagittal depth, 7.11 vs 5.96 mm; P = .046; coronal depth ratio, 0.05 vs 0.01 mm; P = .003), were more likely to develop progeny bone (69.4% vs 44%; P = .047), and demonstrated higher radiographic healing rates (52.8% vs 24%; P = .025) compared with WB lesions. PROMs at follow-up were available for 25 of 62 patients (40.3%), with no statistically significant differences between cohorts at any time. Return to full activity was observed in 72% of WB and 82.1% of NWB lesions (P = .378).
Conclusion:
Lateral femoral condyle OCD lesions of the knee in WB and NWB zones presented similarly at initial evaluation; however, NWB lesions demonstrated higher rates of progeny bone formation and radiographic healing at mean 2-year follow-up.
Keywords
Juvenile osteochondritis dissecans (OCD) is described as a focal, idiopathic alteration of subchondral bone and the overlying articular cartilage. 8 Disease initiation occurs when a localized area of epiphyseal cartilage or subchondral bone undergoes an ischemic event, resulting in alteration of subchondral support that may eventually lead to changes at the articular surface. Repetitive microtrauma is the most commonly suggested external mechanism that may contribute to the condition, with lesions forming in regions of high compressive loads, particularly the lateral aspect of the weightbearing (WB) portion of the medial femoral condyle (MFC). At-risk patients may include those with smaller intercondylar notches, larger anterior tibial spines, increased posterior and medial tibial slope, and discoid lateral menisci in the case of lateral femoral condyle (LFC) lesions. 4,6,20,24 However, lesions may also present in traditionally nonweightbearing (NWB) articular regions, such as the posterior femoral condyles. 14,15 The relative contribution of loading to the pathophysiology of OCD development therefore remains controversial and warrants further investigation.
OCD lesions can take on several variations with regard to radiographic appearance. During the healing phase, newly ossified epiphyseal bone is termed “progeny” bone, whereas the remainder of the surrounding epiphysis is termed the parent bone. 22 Management of juvenile OCD lesions of the knee has traditionally been guided by lesion stability and size, with an emphasis on offloading the lesions. Whether nonoperative or operative management is recommended, patients are subsequently treated via activity modification to minimize joint loading and, oftentimes, via WB restrictions.
While the most common site of an OCD lesion in the knee is the lateral border of the MFC, LFC lesions have received less focused study. These LFC OCD lesions may occur commonly in anterior zones of full WB in the standing position or in more posterior, lesser WB zones. It is unclear whether lesion location, and possibly differential loading, results in differing lesion size and bone-forming characteristics. The purpose of this study was to examine LFC OCD lesions to determine whether clinical and radiographic variables differ by WB zone location. It was hypothesized that the healing potential of lesions within these distinct WB zones may vary as a result of differential loading.
Methods
Study Design and Setting
Institutional review board approval was obtained for this study. Data from 62 consecutive patients with juvenile OCD lesions of the knee were collected over a 15-year period between 2004 and 2018 (Figure 1). All patients were aged

Data collection flow CONSORT (Consolidated Standards of Reporting Trials) diagram. JOCD, juvenile OCD; OCD, osteochondritis dissecans.
Prospective Collection of PROMs
Patients who were evaluated after March 2015 were enrolled in an institutional review board-approved multicenter prospective cohort in which knee functional assessments were collected prospectively. PROMs for each patient included the Knee injury and Osteoarthritis Outcome Score (KOOS), Pediatric International Knee Documentation Committee (Pedi-IKDC) subjective knee form, and Hospital for Special Surgery Pediatric Functional Activity Brief Scale (Pedi-FABS). Of the 62 enrolled patients, 26 (41.9%) were administered the PROMs at baseline, and 25 (40.3%) had PROMs meeting a minimum of 1-year follow-up. Remaining data collection was performed in a retrospective review of medical records, radiographs, and magnetic resonance imaging (MRI) studies.
Retrospective Collection of Clinical and Radiographic/MRI Data
Clinical Assessment
Descriptive data included sex, age, athletic status, and body mass index at diagnosis. Additional baseline data available for all patients included laterality of lesion site, symptoms, and duration of symptoms before clinic presentation, and inciting mechanism. Duration of follow-up was determined by the date of the latest clinical examination and imaging. Surgical technique was reported in patients who underwent operative management. Reported metrics at final follow-up included rate of return to full activity for 53 of 62 patients (85.5%), presence or absence of a pain-free knee for 56 of 62 patients (90.3%), and whether the patient underwent a revision procedure.
Imaging
All radiographic studies were performed at the institution where the current study was conducted. Radiographic views included anteroposterior, notch, merchant, and lateral projections. Given the retrospective nature of this study over a 14-year period, variation in MRI and sequencing was noted because of institutional changes and select patients presenting with MRI scans from external sources. The radiographic appearance of lesions on radiographs and MRI scans was quantified based on width and depth in the coronal and sagittal planes, as described by the Research in Osteochondritis Dissecans of the Knee (ROCK) Study Group. 22 Localization of OCD lesions to WB and NWB zones on lateral knee radiographs was defined according to the Cahill and Berg classification, 3 with zone B lesions defined as WB in the sagittal plane and zone C defined as NWB, as shown in Figure 2. 9,10 Lesions in >1 zone were classified in the zone in which the majority of the lesion was located. Progeny fragments were characterized based on radiographic presence, whether a distinct border was noted between parent bone, location, and displacement as described by the ROCK Study Group. 22 Additionally, the presence or absence of a discoid meniscus was determined on MRI evaluation. Preoperative assessment of lesion stability was determined by the treating surgeon using previously published MRI criteria. 11,17
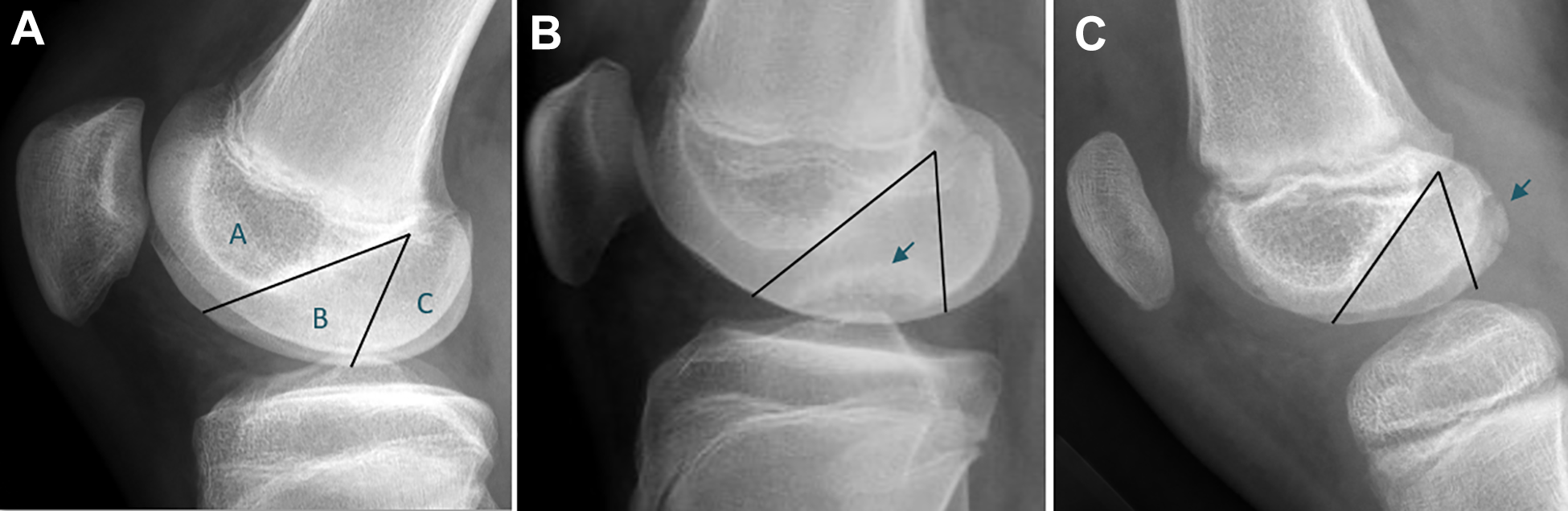
Classification of osteochondritis dissecans (OCD) lesions by weightbearing zone according to Cahill and Berg. 3 (A) Zone A is bordered by a line overlying the roof of the intercondylar notch. Zones B and C are separated by a line projecting distally from and parallel to the posterior femoral cortex. (B) OCD localized to the weightbearing portion of the femoral condyle (arrow). (C) OCD localized to the nonweightbearing portion of the femoral condyle (arrow).
Nested Treatment Analyses
Nested cohort analyses were retrospectively conducted for each management technique to determine whether an association with clinical or radiographic outcomes was present when comparing WB and NWB lesions. Data were analyzed among all patients who underwent nonoperative management, all patients who collectively underwent operative management, and patients who underwent the 2 most frequently utilized techniques (arthroscopic drilling and OCD fixation).
Statistical Analysis
Clinical and radiographic outcome comparisons between Cahill and Berg 3 sagittal B and C lesions as well as across various surgical techniques were analyzed for statistical significance. Continuous variables were analyzed using the Mann-Whitney test, while the chi-square test was used to compare categorical variables. A Kruskal-Wallis test was used when comparing >2 groups. SAS 9.4 (SAS, Cary, NC) was used to run the analysis. Statistical significance was defined as p-value <0.05.
Results
Characteristics
Of the 62 LFC OCD lesions that met the inclusion criteria, 26 (41.9%) were classified as WB, and 36 (58.1%) were NWB. There were no zone A lesions. No significant differences were noted in baseline characteristics between groups (Table 1). There were 9 patients who presented with bilateral lesions, with the designation of “primary side” being the side that was symptomatic first; 4 WB lesions and 5 NWB lesions presented as the primary side. There was no association between lesion localization and presentation as the primary side (P = .467). In the WB cohort, 53.8% were athletes compared with 63.9% in the NWB group (P = .089).
Patient Characteristics, Presenting Symptoms, and Baseline Functional Assessment Scores a

a Data are reported as n (%) or mean ± SD (range). ADL, Activities of Daily Living; FABS, Functional Activity Brief Scale; IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; NWB, nonweightbearing; Pedi, Pediatric; QOL, Quality of Life; WB, weightbearing.
There were no significant differences in clinical presentation between the WB and NWB groups (Table 1). The most common presenting symptom was activity-related pain (88.5% of WB, 91.7% of NWB; P = .689). Four patients (15.4%) in the WB group presented after a traumatic injury compared with 15 (41.7%) in the NWB group (P = .084). A minority of patients in each cohort reported mechanical symptoms (38.5% of WB vs 41.7% of NWB; P = .8). Although not statistically significant, 33.3% of NWB lesions presented with an effusion, while only 15.4% in the WB group had an effusion at presentation (P = .111). At presentation, there were no differences in baseline KOOS or Pedi-IKDC. Activity scale (Pedi-FABS) was also not significantly different between the WB and NWB groups. The mean duration for clinical follow-up for both cohorts was 24.1 months (29.27 ± 21.68 months for WB lesions and 19.99 ± 12.36 months for NWB lesions; P = .112).
A separate analysis comparing the same variables from Table 1 was performed between patients with and without 1-year PROM data to determine the degree of sampling bias within the former cohort (Table 2). A significantly higher proportion of patients with 1-year PROMs (84% vs 43.2%; P < .001) self-reported as athletes. No other significant differences were found in baseline characteristics, symptomatology, or mechanism of injury.
Comparison of Baseline Statistics and Presenting Symptoms Between Patients With and Without 1-Year PROM Data a
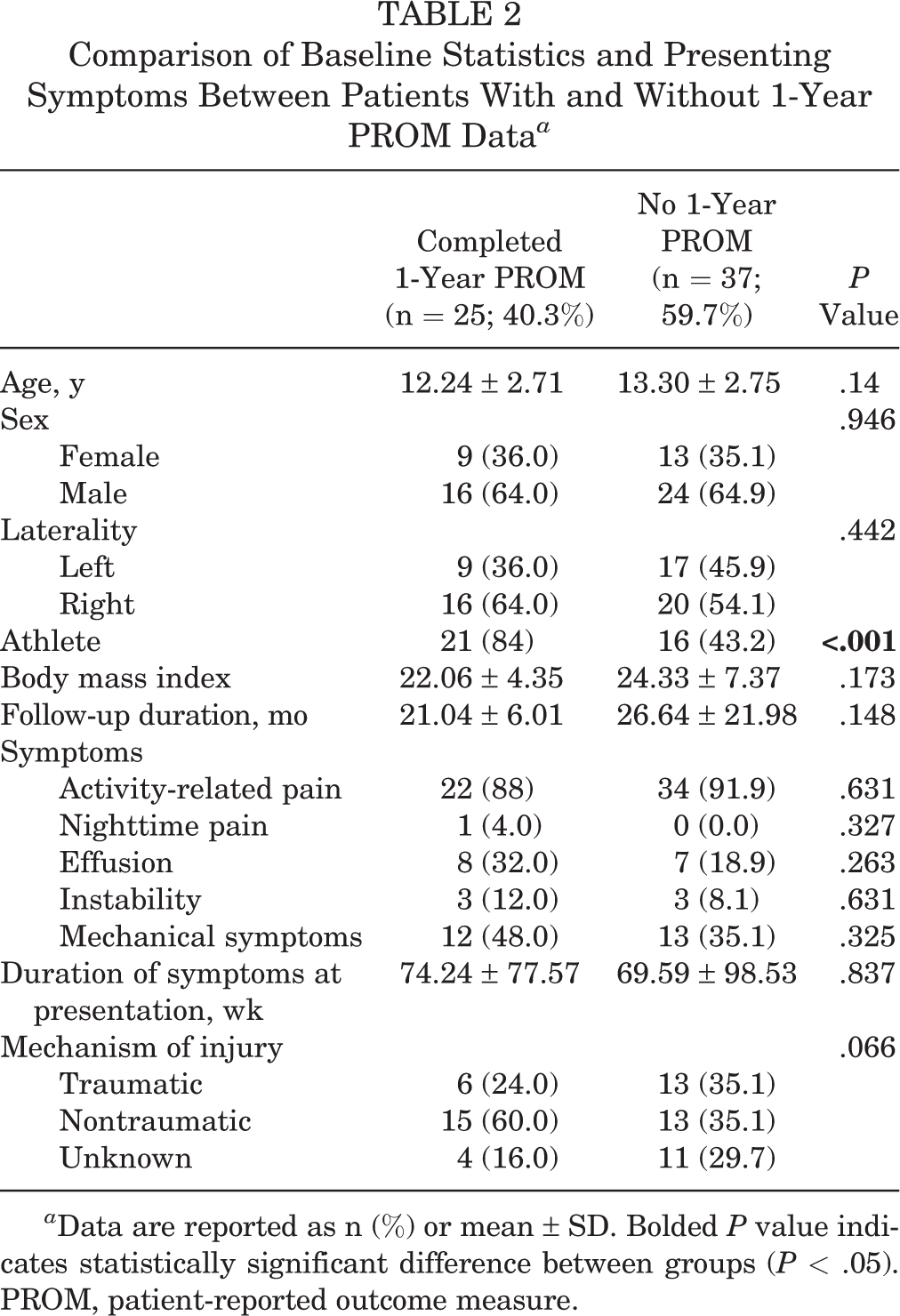
a Data are reported as n (%) or mean ± SD. Bolded P value indicates statistically significant difference between groups (P < .05). PROM, patient-reported outcome measure.
Imaging Findings
Lesion Size
Radiographic and MRI measurements taken at patient presentation are listed in Table 3. Out of 62 patients, 61 (98.4%) had available imaging studies. For each lesion, we also calculated normalized width and depth as a ratio in the coronal and sagittal planes and length and depth in the sagittal plane, using the technique described by Wall et al. 23 These calculations were performed by dividing the lesion size by the width, length, or depth of the condyle. Interestingly, NWB lesions tended to be deeper on MRI scans than were WB lesions, with a greater depth noted in the sagittal plane (7.11 ± 2.51 mm vs 5.96 ± 1.70 mm; P = .046) as well as a greater coronal plane depth ratio (0.05 ± 0.05 mm vs 0.01 ± 0.03 mm; P = .003). No statistically significant differences in any other baseline radiographic measurements were found between the WB and NWB groups.
Baseline Osteochondritis Dissecans Lesion Radiographic and MRI Measurements a
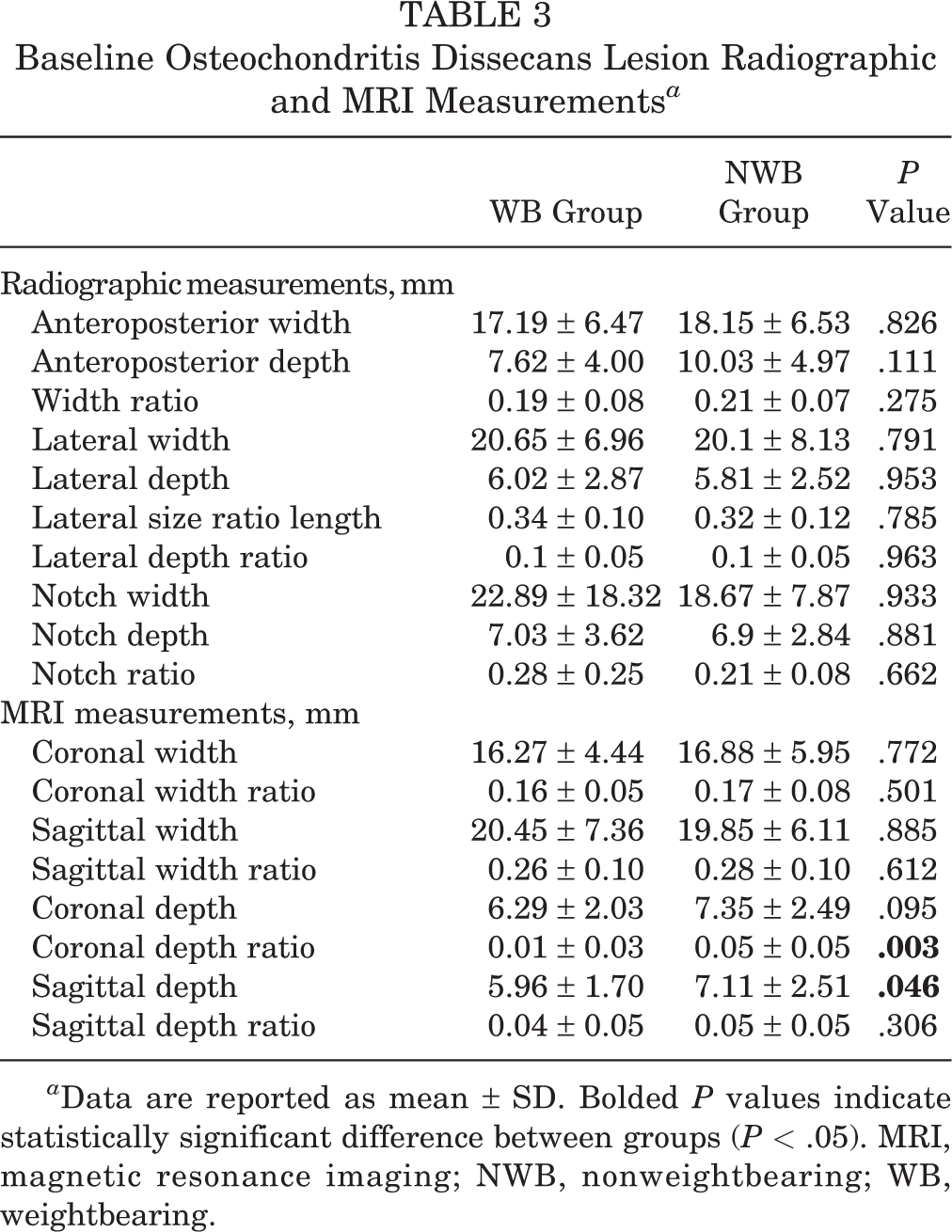
a Data are reported as mean ± SD. Bolded P values indicate statistically significant difference between groups (P < .05). MRI, magnetic resonance imaging; NWB, nonweightbearing; WB, weightbearing.
Progeny Characteristics
Progeny fragments can present with distinct appearances radiographically, ranging from radiolucent in a primarily cartilaginous form to opaque when well ossified (Figure 3). All progeny fragments within the WB cohort were nondisplaced from parent bone; however, no statistically significant differences were noted in the degree of progeny displacement between WB and NWB groups (Table 4). At initial presentation, a higher absolute percentage of progeny fragment formation was noted in the NWB group, although the difference was not significant (60.6% vs 36.4%; P = .078). When progeny bone was present, a higher proportion of NWB lesions presented with a distinct border between parent and progeny bone (70% vs 25%; P = .044).

Radiographs of lateral femoral condylar osteochondritis dissecans lesions with depicted variations in progeny fragment ossification. (A) Nonossified progeny bone appears radiolucent. (B) Ossified progeny bone with a distinct border from parent bone.
Radiographic Characteristics at Presentation and at Mean 24-Month Follow-up a

a Data are reported as n (%). Bolded P values indicate statistically significant difference between groups (P < .05). NWB, nonweightbearing; WB, weightbearing.
At mean 24-month follow-up, several radiographic dissimilarities were noted. Progeny bone formation was significantly higher among NWB lesions than WB lesions (69.4% vs 44%; P = .047). Additionally, a significantly greater proportion of NWB lesions progressed to healing, as determined by evidence of complete or near-complete radiographic union (52.8% vs 24%; P = .025). Possibly consistent with healing, the number of lesions with a distinct border between progeny and parent bone decreased in both the WB and the NWB groups relative to baseline values, and the difference between the 2 cohorts was no longer statistically significant (12% vs 11.1%; P = .999).
Treatment Modality
Nonoperative management was the initial treatment modality for 34.6% of WB lesions and 41.7% of NWB lesions (P = .574), as shown in Table 5. When a surgery was chosen as the primary treatment, several techniques were used, either in isolation or conjunction. These included chondroplasty, fixation of the OCD fragment, adjunct tibial autograft, arthroscopic drilling, completed excision of the OCD fragment, defect marrow stimulation (microfracture), and osteochondral allograft transplantation. Given the retrospective nature of the study, OCD localization to the WB or NWB zones did not influence the technique used. Arthroscopic drilling (11 WB and 15 NWB lesions) and OCD fixation (8 WB and 7 NWB lesions) were the 2 most commonly used techniques.
Initial Treatment Modality and Cumulative Frequency of Operative Techniques Utilized in Surgical Cases a
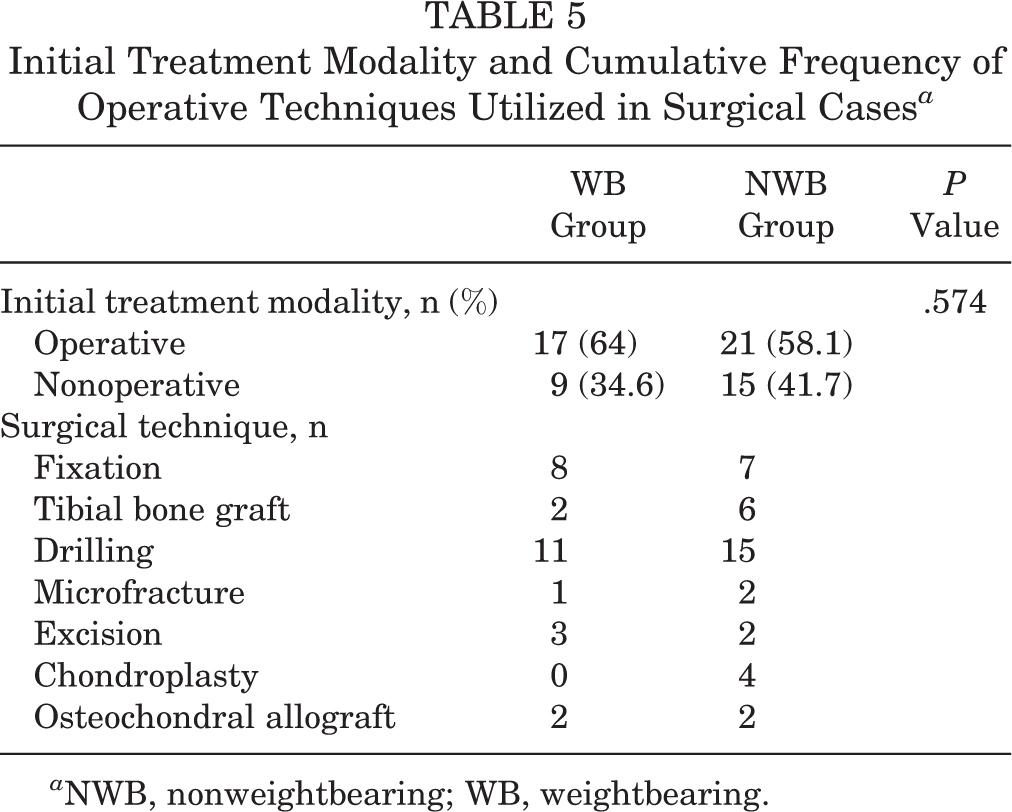
a NWB, nonweightbearing; WB, weightbearing.
Clinical Outcomes
Nonoperative Treatment
Table 6 shows the status of the OCD lesions in patients whose primary management was nonoperative (n = 24; 38.7% of all LFC OCD lesions), at mean 24-month follow-up. Final radiographs were available for 23 of 24 (95.8%) of these patients. There were no significant differences in the clinical or radiographic outcomes between WB and NWB lesions treated without surgery. A total of 9 patients (37.5%) had unsuccessful nonoperative management and converted to surgery, while 13 patients (54.2%) demonstrated radiographic healing. The majority of LFC OCD lesions initially treated nonoperatively were pain-free (n = 13; 54.2%), and patients had returned to full activity (n = 15; 62.5%) at final follow-up.
Clinical and Radiographic Outcomes of Nonoperative Management at 24-Month Follow-up a

a Data are reported as n (%). NWB, nonweightbearing; WB, weightbearing.
Operative Treatment
Outcomes after the 2 most commonly performed surgical techniques, arthroscopic drilling and OCD fixation, are presented in Table 7. Of the 16 lesions treated using isolated drilling, 6 were WB, and 10 were NWB. When comparing results by lesion localization, the rate of radiographic union was low in both groups (16.7% of WB lesions and 40% of NWB lesions; P = .29). The majority of patients achieved a pain-free knee (68.8%) and returned to full activity (68.8%). Finally, of the 9 lesions treated using both drilling and fixation, 5 were WB, and 4 were NWB. Radiographic union was achieved in 20% of the WB lesions and 25% of the NWB lesions (P = .49).
Among operatively managed patients with WB lesions, 5 patients (23.8%) underwent a second surgery. Procedures included osteochondral allograft transplantation (n = 3; 1 as a staged cartilage restoration procedure, 2 after failed fixation/drilling), OCD refixation after failed primary fixation (n = 1), and debridement/loose body removal after failed microfracture (n = 1). In operatively managed patients with NWB lesions, 6 patients (23.1%) underwent a second surgery. Procedures included bone marrow aspirate concentrate injection after failed arthroscopic drilling (n = 2), staged osteochondral allograft transplantation (n = 1), implant removal after OCD fixation/tibial bone grafting (n = 1), and debridement/loose body removal after failed fixation/drilling/bone grafting (n = 1). The mean time from index surgery to each revision procedure was 1.89 ± 2.09 years.
Clinical and Radiographic Outcomes After Most Frequently Utilized Operative Techniques at 24-Month Follow-up a

Data are reported as n (%) unless otherwise indicated. NWB, nonweightbearing; WB, weightbearing.
Overall Outcomes
Responses to PROMs were received from 25 patients (40.3%). Collective outcomes of all patients are shown in Table 8. When comparing the WB and NWB groups, no statistically significant differences were seen in the rate of return to full activity (72% vs 82.1%; P = .378) or presence of a pain-free knee (75% vs 71.9%; P = .794). No statistically significant differences were evident in all measured functional assessment scores.
Combined Clinical Outcomes and PROMs After All Treatment Modalities at 24-Month Follow-up a
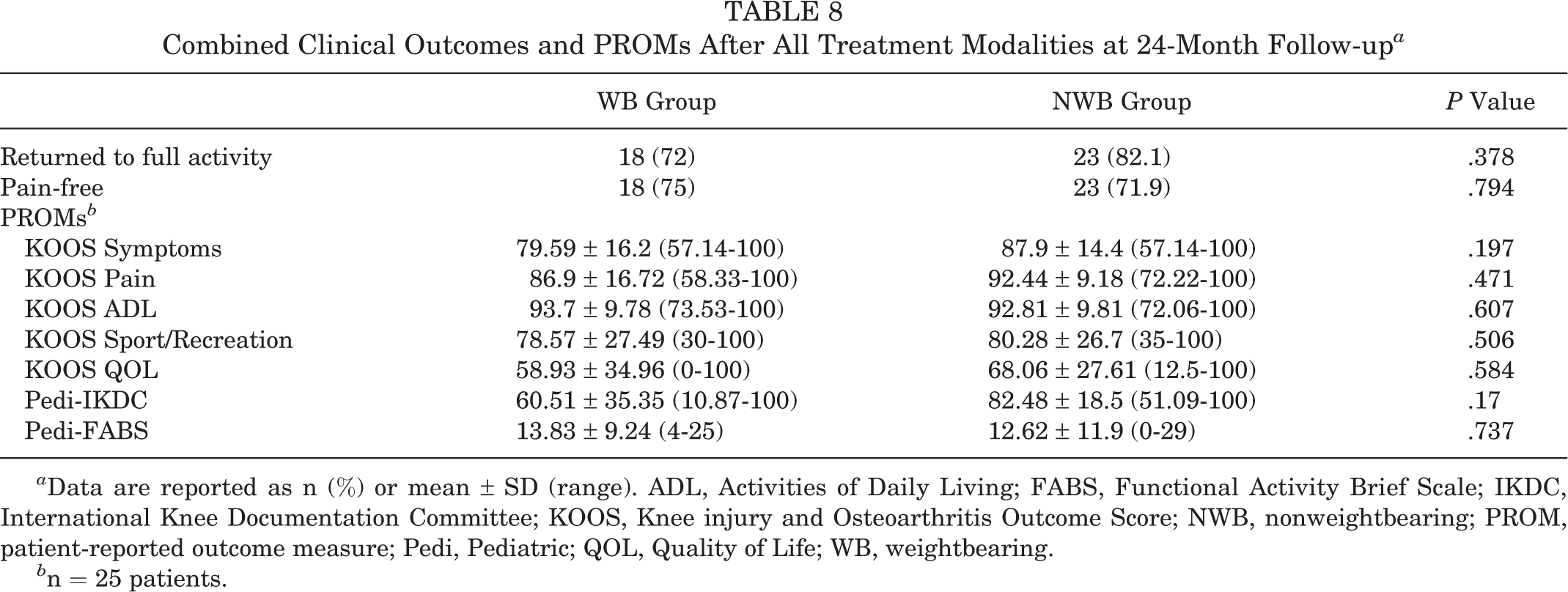
a Data are reported as n (%) or mean ± SD (range). ADL, Activities of Daily Living; FABS, Functional Activity Brief Scale; IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; NWB, nonweightbearing; PROM, patient-reported outcome measure; Pedi, Pediatric; QOL, Quality of Life; WB, weightbearing.
b n = 25 patients.
Discussion
Juvenile OCD lesions occur most commonly at the knee, and while the LFC is the second most common site of these lesions, literature on their management remains limited. Given the variability in presenting symptoms, imaging studies have been found to be of increasing utility in managing these lesions. Kijowski et al 11 proposed a set of MRI criteria for assessing the stability of OCD lesions, to include a rim of T2 signal, multiple breaks in the subchondral plate, fluid-filled defects, and surrounding cysts. While the authors reported a collective sensitivity of 100%, specificity for juvenile OCD lesions was 11%, suggesting limitations for the evaluation of stability and healing potential of these specific lesions. Harding 9 and Cahill 2 initially described on radiographs a discrete WB region projecting distally from the intersection of the Blumensaat line and the posterior femoral cortex. However, no studies have examined the prognostic potential of this radiographic landmark. We presented a retrospective cohort study of LFC OCD lesions, comparing clinical and radiographic variables by WB zone locations, and noted several key findings within our analyses.
First, the influence of external loading on OCD formation remains unclear. Previous studies have shown the evolution of changing vascular patterns or a genetic predilection affecting endochondral ossification to be potential sources of pathogenesis for OCD lesions. 19,21 While increased external loading has also been suggested to be a factor influencing the formation of an OCD lesion, at presentation these LFC OCD lesions did not have differing symptoms, sizes, or ossification characteristics when analyzed using localization to WB and NWB zones in the current study. 1 However, during follow-up, more posterior NWB than WB lesions were noted to have increased rates of progeny bone ossification (69.4% vs 44%) and bony union. Additionally, when LFC OCD lesions did initially present with an ossified progeny bone, those in the NWB zone were more likely to have a well-visualized, distinct border (70% vs 25%). The understanding of the formation of ossification within the progeny bone or the appearance of a distinct border remains unclear; however, this study may provide early evidence that WB zones or WB lesions may predispose to different characteristics in the formation and appearance of bone within the progeny. Future, larger studies will help further our understanding of these lesions.
Second, treatment modality did not differ by WB region in this study of LFC OCD lesions. Although various techniques have been described in the management of OCD lesions, current American Academy of Orthopaedic Surgeons Clinical Practice Guidelines report “strong recommendations” for 0 of 16 available techniques. 5 In a case series of 30 patients with stable OCD lesions, Kocher et al 13 demonstrated radiographic healing in all patients at a mean of 4.4 months after transarticular arthroscopic drilling. Edmonds et al 7 demonstrated a radiographic healing rate of 98.2% in 59 patients who underwent an extra-articular, intraepiphyseal drilling technique. In another case series of 26 knees at 14.7-year follow-up, internal fixation using either metal or bioabsorbable screws yielded a healing rate of 84.6%. 12 Schlechter et al 18 analyzed outcomes in 38 patients undergoing bioabsorbable fixation and reported Lysholm and Pedi-IKDC scores of 89.8 and 88.1, respectively. As such, when appropriately indicated, both arthroscopic drilling and fixation have demonstrated favorable outcomes. Our analysis showed no correlation between surgical technique used and lesion zone. This is not unexpected given that initial management was largely dependent on lesion stability, chronicity, and size, none of which was correlated with sagittal zone location and the implications of which are beyond the scope of this study. Third, we demonstrated that clinical outcomes after the most commonly used surgical techniques may be independent of radiographic WB zone, as a greater number of patients in both WB and NWB cohorts reported a pain-free knee (75% and 71.9%) and return to their previous activity level (72% and 82.1%) than demonstrated a healed lesion on subsequent imaging (24% and 52.8%).
The limitations of our study include the small number of patients, despite the fact that it was a relatively large series of exclusively studied LFC OCD lesions. While our shortened inclusion criteria of 1-year minimum follow-up was needed to maintain sample sizes for statistical analyses, increased duration of follow-up may improve the quality of our data. Furthermore, as previously stated, only 25 patients (40.3% of the study group) had 1-year PROMs available for review. While this limitation further reduces study power in the evaluation of functional assessment scores and introduces potential sampling bias, our analysis of baseline variables between patients with and without PROMs was significant only for a higher proportion of athletes among those with completed PROMs. This finding is reflective of general trends seen among youths in sports participation and the injury risks associated with recent increases in sports specialization. 16 Not all patients had completed knee pain, return to activity, or imaging assessments available for retrospective analysis. Taken collectively, these reductions in sample sizes may limit conclusions on comparative analyses pertaining to our study goals. Finally, the inherent biases associated with a retrospective review should also be considered.
Conclusion
We demonstrated that presentation symptoms, size, and ossification of LFC OCD lesions did not differ by sagittal WB zone location. However, lesions within NWB areas demonstrated comparatively higher rates of progeny bone formation and bony union at follow-up, suggesting that the influence of loading may be an important part of the osseous response of treated, and possibly untreated, lesions. While resolution of pain symptoms and return to baseline activity is expected in the majority of patients at short-term follow-up, radiographic evidence of incomplete bony union is common in both WB and NWB lesions. Future studies with longer follow-up duration are necessary to fully evaluate outcomes.
Footnotes
Acknowledgment
The authors thank Dr Chanhee Jo for her analysis of the data and contribution to the study.
Final revision submitted January 17, 2021; accepted February 24, 2021.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from University of Texas Southwestern Medical Center (protocol No. STU 082014-003).