
Abstract
Background:
While the deleterious long-term effects of microfracture are well documented, studies examining the long-term clinical outcomes in patients treated with osteochondral autograft transfer (OAT) are scarce.
Purpose:
To assess the mid- and long-term clinical outcomes of primary OAT performed for the treatment of symptomatic articular cartilage lesions of the knee.
Study Design:
Case series; Level of evidence, 4.
Methods:
The medical records of 63 patients who underwent primary OAT were retrospectively queried from an institutional cartilage registry. Patient-reported outcome measures (PROMs) for patients treated with OAT from the practice of 6 fellowship-trained knee specialists were recorded. Patients with symptomatic articular cartilage lesions of the medial or lateral femoral condyle or trochlea who were treated with OAT were included. All patients had preoperative baseline PROMs; the minimum follow-up was 2 years. Exclusion criteria were previous ipsilateral knee surgical procedures, generalized osteoarthritis, revision cartilage procedures, previous total meniscectomy, and history of inflammatory arthropathy. Clinical outcomes, reoperation rates, and conversion to arthroplasty were analyzed.
Results:
The mean patient age was 27.4 ± 12.4 years (range, 11-56 years), and 23/63 (31.7%) were female. The mean follow-up was 5.7 ± 3.2 years (range, 2-16 years). The mean lesion size was 2.3 ± 1.6 cm2 (range, 0.6-6.5 cm2), and the mean number of OAT dowels used per case was 2.2 ± 1.3 (range, 1-7). Sixteen patients had a 10-year follow-up. The mean International Knee Documentation Committee (IKDC) score significantly increased from 46.4 ± 15.1 preoperatively to 76.1 ± 19.0 at the 2-year follow-up, 78.0 ± 18.0 at the 5-year follow-up, and 70.4 ± 22.6 at the 10-year follow-up (P < .001). The mean Knee Outcome Survey–Activities of Daily Living score increased from 64.4 ± 16.3 preoperatively to 83.2 ± 12.7 at the 2-year follow-up, 85.1 ± 11.8 at the 5-year follow-up, and 83.8 ± 11.7 at the 10-year follow-up (P < .001). Overall, 69% and 67% of patients treated with OAT surpassed the minimal clinically important difference (MCID), for the IKDC and KOS-ADL scores, respectively, at the 2-year follow-up. Similarly, 60% and 33.3% of patients treated with OAT surpassed the MCID and SCB, respectively, for the IKDC score at the 10-year follow-up. The overall reoperation rate was 28.6% and occurred at a mean of 3.67 ± 6.2 years after the index procedure.
Conclusion:
Primary OAT is an effective and durable cartilage restoration procedure for some patients with symptomatic knee cartilage lesions at mid- to long-term follow-up, with a majority of patients demonstrating sustained improvements in clinical outcomes and achieving the MCID. However, a clinically important surgical failure rate exists, with up to one-third of patients needing a revision cartilage restoration procedure and only one-third of patients achieving the SCB for the IKDC score at the 10-year follow-up.
Osteochondral autograft transfer (OAT) and mosaicplasty are single-stage cartilage repair techniques. OAT is characterized by the transfer of single viable bone-cartilage dowels harvested from low-weightbearing areas to treat symptomatic chondral and osteochondral defects of the knee condyles, while mosaicplasty involves the transfer of multiple osteochondral cylinders. Both techniques allow for an immediate restoration of osteochondral architecture; the use of autograft tissue facilitates predictable bony healing, easier graft accessibility, and lower cost compared with other commonly used cartilage repair methods. 15 Additionally, OAT permits early weightbearing and faster rehabilitation compared with cell-based cartilage repair techniques. 11 In a cohort of 303 knees, Hangody et al 5 reported success rates of 91%, 86%, and 74% at a mean 9.6-year follow-up for femoral, tibial, and patellofemoral mosaicplasty procedures performed, respectively.
Previous studies focused on the clinical outcomes after OAT have emphasized short- and midterm results, with those presenting longer-term data representing case reports,2,8,13,14 smaller patient populations, and data derived from populations undergoing combined procedures. 2 Furthermore, many longer-term studies in cartilage restoration tend to group OAT, allograft transplantation, and cell-based cartilage repair techniques in clinical outcome reporting and have not reported on the propensity for clinically significant outcome achievement; this reporting phenomenon makes it difficult for clinicians to understand the expected long-term outcomes after OAT procedures, which is critical given the high expectations and demands of this patient population.3,9,15,23 As such, providing additional prognostic data, such as projected rates of clinically significant outcome achievement, may allow clinicians to better educate patients with chondral and osteochondral defects and help refine patient selection.
Microfracture (MFX) has been well established to be a poor long-term solution for symptomatic cartilage lesions, although it remains commonly performed due to its technical ease and avoidance of an arthrotomy. 9 While some studies have suggested favorable short-term results after MFX,1,26 others have reported deterioration in patient functional outcomes after 2 years.16,17 It has been reported that OAT may offer patients with symptomatic cartilage defects the highest rate of return to sport and return to play at their preinjury level.12,17,18 Given that the current body of literature reporting long-term data for patients treated with OAT is limited and infrequently defines clinically significant outcome achievement, quantifying the proportion of patients achieving the minimal clinically important difference (MCID) and substantial clinical benefit (SCB) in this unique population can provide valuable prognostic data. The purpose of this study was to assess the mid- and long-term clinical outcomes of primary OAT performed for the treatment of symptomatic articular cartilage lesions of the knee.
Methods
Patient Selection and Study Design
A longitudinally maintained prospective institutional registry dedicated to the tracking of patient outcomes after articular cartilage restoration procedures was retrospectively queried for patients who underwent OAT from September 1999 through April 2021. An institutional review board approved the institutional registry, and all patients signed an informed consent form before participation. For this study, inclusion criteria included patients undergoing OAT as a primary cartilage repair procedure with a minimum 2-year follow-up for a single patient-reported outcome measure (PROM). Patients who had undergone any previous ipsilateral knee cartilage repair procedure were excluded. Additional exclusion criteria included osteoarthritis, inflammatory arthropathy, previous total meniscectomy, and patients treated for bipolar lesions.
Study Population Selection and Data Collection
Of the 244 registry patients who underwent OAT of the knee, 63 patients met selection criteria and had a minimum 2-year follow-up. Of the selected 63 patients, 38 patients (60.3%; 38/63 knees), 32 patients (50.8%; 32/63 knees), and 16 patients (25.4%; 16/63 knees) had minimum 2-year, 5-year, and 10-year follow-ups, respectively, for a corresponding PROM that was necessary for clinically significant outcome analysis (Figure 1).
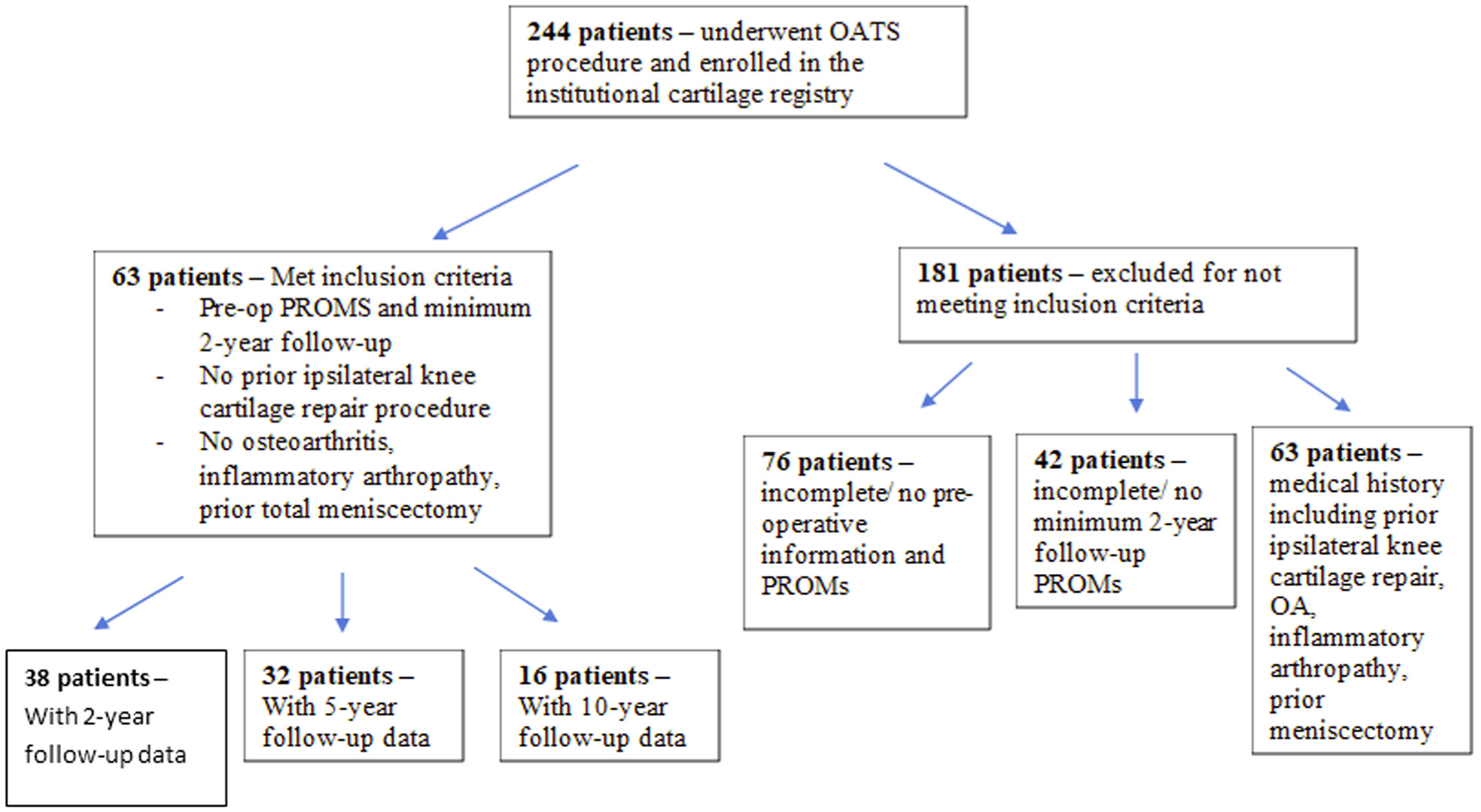
Flow diagram for inclusion and exclusion of patients who underwent osteochondral autograft transfer (OAT). OA, osteoarthritis; PROM, patient-reported outcome measure.
Demographic, preoperative, intraoperative, and postoperative data were collected. Demographic data included patient age, sex, and body mass index (BMI). Preoperative data included the number and type of previous ipsilateral knee surgical procedures and baseline PROMs. Analysis of magnetic resonance imaging (MRI) data included lesion location, lesion size, the presence of bony edema, an evaluation of the menisci, and an evaluation of the knee ligaments. Intraoperative data included an examination under anesthesia (range of motion and ligamentous stability), lesion location, lesion size, Outerbridge grade of the articular surfaces in the unaffected compartments, number of dowels used per case, and meniscal status. Postoperative data included PROMs at a minimum of 2 years after surgery.
Indications and Surgical Technique for OAT
OAT was selected as the treatment option for these patients based on clinical judgment of defect complexity, location, and size, as well as failure of previous nonsurgical or nonreparative cartilage treatments. Surgical procedures were performed by 6 fellowship-trained orthopaedic surgeons (R.J.W.) at a single academic institution with extensive experience in cartilage restoration.
MRI analysis of preoperative imaging demonstrated an isolated full-thickness articular cartilage lesion in all cases. Examination under anesthesia demonstrated ligamentously stable knees in all patients. All patients were noted to have achieved full extension (within 5°) and a minimum flexion angle of 130°. After examination under anesthesia, diagnostic arthroscopy was performed for chondral lesion assessment and characterization. An examination of articular cartilage in the untreated knee compartments demonstrated intact surfaces.
Any concomitant procedures were performed according to surgeon preference. Parapatellar arthrotomy was utilized for joint access. After insertion of deep retractors, the size and shape of the defects were determined. A commercially available OAT system was used to create both the donor plugs and recipient sites within the lesion.
Donor harvest was typically derived from the intercondylar notch anterior to the level of the sulcus terminalis or the superolateral trochlea. Each harvested cylindrical autograft plug was inspected and measured to match its respective recipient site diameter and depth. Each donor plug was then placed and gently tamped into position at the recipient site with press-fit graft fixation. After implantation, each dowel was inspected to match the natural osteoarticular contour of the native condyle. Dowel donor site backfill was performed using lesional bone, allograft cancellous bone chips, or acellular synthetic scaffolds.
Patient-Reported Outcome Measures
For patients included in the registry, outcomes were routinely collected preoperatively and at 1, 2, 3, 4, 5, and 10 years postoperatively. All patients had preoperative baseline PROMs. Routine office follow-up was not generally expected from patients past 1 year, and PROMs were not collected for patients after a revision cartilage procedure or arthroplasty. Patients were contacted remotely for the collection of postoperative outcome measures beyond 2 years. As not all postoperative PROMs were available, mean values of available data points were calculated for the aforementioned follow-up periods. General health outcomes for each patient were assessed using the 36-Item Short Form Health Survey (SF-36; Version 1.0), which has the ability to evaluate 8 domains of general well-being. Of the 8 domains, the Physical Function and Role Limitations–Physical Health domain scores were available for data analysis. Knee function was assessed using the International Knee Documentation Committee (IKDC) Subjective Knee Evaluation and Knee Outcome Survey–Activities of Daily Living (KOS-ADL) Scale. The IKDC score is a reliable and valid knee-specific measure of symptoms and function and has been shown to provide a good overall measure of knee-related disability among patients treated with a cartilage restoration procedure. 7 An independent observer performed all pre- and postoperative data collection for these PROMs. Additionally, the percentages of patients achieving the MCID and SCB for the IKDC and KOS-ADL scores were determined utilizing previously published thresholds.19,30
Reoperation Rate
Patients who underwent reoperation to the knee for any reason (ie, chondroplasty, meniscectomy or loose-body removal, or partial or total knee arthroplasty) were noted.
Conversion Rate
Patients who underwent conversion to arthroplasty (partial or total knee arthroplasty) to the knee were noted.
Statistical Analysis
All statistical analyses were performed using SPSS statistical software (Version 29.0, SPSS Inc). Descriptive statistics are quantified using means with standard deviations or ranges, while categorical variables are quantified using frequencies with percentage. Paired t tests were used to determine within-group differences between pre- and postoperative outcomes. A P value <.05 was deemed statistically significant.
Results
Patient Demographics and Characteristics
During the study period, the medical records of 63 patients who underwent primary OAT with a minimum follow-up of 2 years were analyzed. The final mean follow-up was 5.7 ± 3.2 years (range, 2-16 years). This final cohort had a mean age of 27.4 ± 12.4 years (range, 11-56 years) at the time of surgery. The cohort was 36.5% (23/63) female and 63.5% (40/63) male. The mean cohort BMI was 25.5 ± 5.0 kg/m2 (range, 18.2-38.7 kg/m2). Full details are given in Table 1.
Demographic Data for OAT/Mosaicplasty (N = 63) a

Data are given as mean ± SD (range) unless otherwise indicated. OAT, osteochondral autograft transfer.
The mean lesion size was 2.3 ± 1.6 cm2 (range, 0.6-6.5 cm2), requiring a mean of 2.2 ± 1.3 (range, 1-7) autograft plugs. Six-, 8-, and 10-mm diameter plugs were most commonly utilized. The most common lesion locations were the medial femoral condyle (47.6%) and lateral femoral condyle (27.0%). All lesions demonstrated underlying bone marrow edema on preoperative MRI and are further detailed in Table 2. The number of concomitant procedures was 21 (33.3%) in 63 patients. Partial meniscectomy/meniscal repair (9/21), lateral release (7/21), and tibial tubercle osteotomy (6/21) procedures were most frequently performed. Donor site backfill with acellular synthetic scaffold plugs was performed in 68.3% (43/63) of cases.
Osteochondral Lesion Characteristics a

Data are given as n (%) or mean ± SD (range). LFC, lateral femoral condyle; MFC, medial femoral condyle; MPFL, medial patellofemoral ligament.
Patient-Reported Outcome Measures
Statistically significant improvement in PROMs was observed from baseline to 2, 5, and 10 years postoperatively. The SF-36 Physical Function subscale increased from a mean score of 58.1 ± 23.1 to 83.3 ± 16.2, 85.1 ± 22.2, and 80.3 ± 23.0, at 2, 5, and 10 years, respectively (P < .001). Similarly, the SF-36 Role Limitations–Physical Health subscale increased from a mean score of 53.8 ± 35.0 to 88.1 ± 22.6, 90.0 ± 22.0, and 83.3 ± 33.2, at 2, 5, and 10 years, respectively (P < .001). Patients available at the 5-year follow-up achieved the MCID at rates of 78.3% and 68.8% for the IKDC and KOS-ADL scores, respectively. These patients also achieved SCB thresholds for IKDC and KOS-ADL measures at 60.9% and 68.8%, respectively. Fifteen patients available for the 10-year follow-up demonstrated sustained statistically significant improvement in IKDC scores (mean baseline score, 46.4 ± 15.1; mean 10-year score, 70.4 ± 22.6; P < .001). Of these patients, 60% (9/15) achieved the MCID, while 33.3% (5/15) achieved the SCB. These same patients also demonstrated significant improvement in KOS-ADL scores from 64.4 ± 16.3 to 83.8 ± 11.7 (P < .001), with 60% (9/15) meeting previously established thresholds of the MCID and SCB (Figure 2, Table 3).19,29

Patient outcomes at 2 through 10 years. IKDC, International Knee Documentation Committee; KOS-ADL, Knee Outcome Survey–Activities of Daily Living; SF-36, 36-Item Short Form Health Survey.
Patient Outcomes a

Data are given as n (%) or mean ± SD. IKDC, International Knee Documentation Committee; KOS-ADL, Knee Outcome Survey–Activities of Daily Living Scale; MCID, minimal clinically important difference; SCB, substantial clinical benefit; SF-36, 36-Item Short Form Health Survey; TKA, total knee arthroplasty.
Statistically significant from baseline score (P < .05).
Reoperation Rate
Eighteen of 63 (28.6%) patients (7 females) required reoperation after their index OAT procedure. Of these 18 patients, 6 (33.3%) required revision cartilage procedures, considered surgical failure, which included 2 repeat OAT procedures and 4 osteochondral allograft (OCA) transplantations. Six (33.3%) patients required arthroscopic procedures including chondroplasty, meniscectomy, loose-body removal, or lysis of adhesions. Three of 18 (16.7%) patients required removal of hardware. One patient required a diagnostic arthroscopy for persistent pain. Two patients underwent total knee arthroplasty (TKA). The mean age at reoperation was 34.32 ± 16.23 years, and the mean time to reoperation was 3.67 ± 6.2 years.
Conversion Rate
Two patients required conversion to TKA, considered surgical failure, for an overall conversion rate of 3.2%. One patient underwent TKA conversion 16 years after their index OAT procedure. The other patient converted at 8 months after the index procedure.
Discussion
These study results demonstrated statistically significant clinical improvement in patients treated with primary OAT at mid- and long-term follow-up for all recorded outcome measures. With appropriate preoperative counseling, the need for a revision cartilage procedure and conversion rate remain appropriately low as a temporizing procedure to maintain active individuals’ demands. The overall reoperation rate was nearly 30%, with a failure rate of 13%. However, only 33% of patients surpassed the SCB for the IKDC score at the 10-year follow-up. Additionally, 60% of those available at the 10-year follow-up met MCID thresholds for both IKDC and KOS-ADL measures. These findings have been corroborated by previous studies with long-term follow-up.3,4,9,22,23,28 Filardo et al 3 prospectively followed 26 patients undergoing OAT for chondral knee defects and found significant improvement in the IKDC subjective and Tegner scores obtained from baseline to the 12-year follow-up. Keszég et al 9 similarly demonstrated the durability of OAT treatments for osteochondral knee lesions (mean size, 2.1 ± 1.2 cm2) in a retrospective review of the records of 55 soccer players, with maintenance of significant improvement (IKDC subjective and magnetic resonance observation of cartilage repair tissue scores) at a mean of 17.5 years after the index procedure. In their comparative 2020 study, Solheim et al 23 additionally reported survival rates >80% for the first 7 years and >60% for 15 years in their OAT cohort (n = 84), which outperformed MFX (n = 119) in both success and longevity. Stratification of our cohort additionally suggested sustained improvement for all outcome measures at the 2-, 5-, and 10-year follow-ups. It is also worth noting that approximately 25% of patients in this series underwent OAT for chondral injuries involving the patellofemoral joint, and 6 patients underwent patellofemoral realignment through a tibial tubercle osteotomy. In this subset of patients specifically, it is challenging to delineate whether clinical improvement is a function of patellofemoral unloading or the cartilage procedure itself.
Importantly, this study individually evaluates OAT as a primary cartilage restoration procedure that reinforces its relative success and durability in stark contrast to the technically easier MFX operation that reproducibly precipitates joint failure beginning as early as 18 months postoperatively. Despite this, cartilage restoration is an imperfect procedure, and it is imperative to counsel patients that they will likely experience clinical improvement but certain patients may experience persistent symptoms, limitations in ADLs, and inability to return to sport at the same level of competition. This is evidenced in the current data, where although the majority of patients achieved clinically significant outcome improvement, it is still possible to experience early surgical failure, wherein 1 patient converted to TKA at 8 months postoperatively. Furthermore, when examining the PROMs of patients who have undergone OAT, overall the IKDC score at the follow-up time points is between 70 and 80, while the KOS-ADL score is between 80 and 86. While the postoperative scores were significant increases from the preoperative PROMs, there are still additional improvements that can be made. Furthermore, the PROMs for patients with a failed OAT were not included. Although data from the current study glean further insight into the midterm outcomes of patients undergoing OAT, it will be imperative to continue to examine the long-term results of this procedure both for prognostic purposes and to understand how to continue to refine patient selection.
In addition to longevity, the literature has also demonstrated the superiority of OAT to MFX in maintaining high-level performance in young, active populations. In 2017, Krych et al 11 published the results of a meta-analysis (2549 patients; mean age, 35 years) on return to sport after OAT, OCA, autologous chondrocyte implantation, or MFX at a mean 47-month follow-up. Return to sport was observed at 93%, 88%, 82%, and 58%, respectively. Additionally, OAT demonstrated the fastest return to sport at 5.2 ± 1.8 months, significantly faster than the other cartilage preservation techniques. 11 Because of the ability of OAT to restore native hyaline cartilage to treated defects, 6 long-term studies have also consistently demonstrated superior PROMs and physical function with OAT over MFX.10,25 In a retrospective comparative study of 96 patients undergoing OAT (n = 48; mean age, 29.7 years) versus MFX (n = 48; mean age, 32.5 years), earlier work by Krych and colleagues 10 demonstrated that patients who underwent OAT exhibited significantly higher Marx Activity Rating Scale scores from baseline at the 2-, 3-, and 5-year follow-ups compared with MFX patients. Despite the size limitations of lesions treated for donor site morbidity, these findings strongly support OAT as the superior treatment of choice for focal small- to medium-sized chondral lesions with and without bony involvement.20,24
Our results also demonstrated a reoperation rate of 28.6% (18/63 patients) at a mean of 3.7 years, with 33.3% of these patients requiring revision cartilage procedure and 22.2% returning for arthroscopic procedures. This rate is slightly higher than but comparable to rates in previously published reviews that have synthesized data from larger patient populations. A recent systematic review of return to sport and adverse events after OAT in 495 patients reported that reoperation rates ranged between 7.1% and 54.1% and conversion to TKA ranged between 3.1% and 16.0%. 18 In their analysis of a large US commercial database, Oeding et al 18 reported a reoperation rate of 11.14% at the 2-year follow-up after 1320 index OATs, with minor arthroscopic debridement surgeries consisting of 90% of these procedures. Arthroplasty conversion was reported at a rate of 9.5%. While low rates are reported in the early postoperative period, data suggest that the proportion of minor debridements decreases over time. In 2016, Pareek et al 21 systematically reviewed long-term outcomes after OAT at a mean follow-up of 10.2 years. The reoperation rate across all included studies (10 studies; 610 patients; mean age, 27.0 years) was 19%, with the largest proportion consisting of surgical debridement (54%), revision cartilage surgery (28%), and conversion to knee arthroplasty (14%). Our data also demonstrated an arthroplasty conversion rate of 3.2%, notably lower than that in aforementioned studies5,20,27; this finding suggests that the effectiveness of primary OAT is durable for most patients over 10 years. 21 However, it is worth noting that the 3.2% conversion rate is representative of patients with 2 years of follow-up; if extrapolated to the 10-year follow-up time point, then the rate may reach as high as 12.5% (2/16), which would be in accordance with the aforementioned systematic review. Furthermore, the fate of those who did not follow up at 10 years is unknown, and the rate of conversion to TKA may be even higher.
This study adds to the literature examining the long-term studies on OAT. This is likely reflective of the narrow clinical indications favoring younger (<40 years of age), higher-demand patients with focal femoral condyle or trochlear full-thickness chondral lesions measuring 2 to 4 cm2 in area. Given the concerns of donor site morbidity, patients may fall outside of these parameters, with more advanced chondral pathology better addressed with OCA or matrix-induced autologous chondrocyte implantation. Moreover, patients evaluated with more generalized cartilage disease may be more appropriately treated with partial or total knee arthroplasty.
Limitations
There are limitations of this study to consider when evaluating these data. First, the study sample size is relatively small; we suspect that this introduced selection bias into our analysis. Additionally, the limited sample size precluded appropriately powered subanalyses, such as stratification by age and BMI thresholds. There were only 16 patients with 10-year follow-up data, and there was a lack of changes in PROMs due to the small sample size and outcomes at different time points. Ideally, larger patient numbers and the addition of a control group would be better suited for generalizing outcomes, and future studies with large sample sizes are warranted to confirm or refute the findings presented in the current study. However, OAT remains a niche procedure that warrants increased use over MFX, which would in turn provide more patients to externally validate this experience. Second, the presented data were retrieved over a 22-year period by 6 fellowship-trained surgeons. This may have resulted in some heterogeneity in surgical technique and postoperative protocols. Finally, there was a paucity of patients treated with OAT available for the 15-year follow-up. As such, reoperation and arthroplasty conversion rates may possibly increase with time, although our study did not demonstrate this.
Conclusion
Primary OAT is an effective and durable cartilage restoration procedure for some patients with symptomatic knee cartilage lesions at midterm follow-up. Although a majority of patients demonstrate sustained improvements in clinical outcomes and achieve the MCID, only one-third achieve the SCB at the 10-year follow-up. Additionally, a clinically important surgical failure rate exists, with up to one-third of patients necessitating a revision cartilage restoration procedure.
Footnotes
Final revision submitted September 16, 2025; accepted October 6, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: K.N.K. is a paid consultant for AllaiHealth; holds stock or stock options in AllaiHealth and BICMD; and is an editorial board member of Arthroscopy. P.N.R. is a board or committee member of the American Association of Hip and Knee Surgeons; receives royalties from Globus Medical; is a paid consultant for Globus Medical and Stryker; receives other financial or material support from Stryker; holds stock or stock options in Johnson & Johnson, Overture, and Intelligent Health Analytics; and is on the editorial or governing board of Journal of Arthroplasty and Arthroscopy. R.J.W. receives royalties from Arthrex and holds stock or stock options in BICMD, Cymedica, Gramercy Extremity Orthopedics, Pristine Surgical, Overture Orthopaedics, Brainbox, Aegility, and Intelligent Health Analytics. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Hospital of Special Surgery Institutional Review Board.