
Abstract
Purpose:
This study aims to determine the prevalence and characteristics of bilateral osteochondritis dissecans of the knee in patients presenting with unilateral symptoms and compare this cohort to patients with unilateral disease.
Methods:
Records of patients ≤18 years old from 2003 to 2016 with a diagnosis of osteochondritis dissecans of the knee and strictly unilateral knee pain were identified. Contralateral (asymptomatic) knee imaging within 1 year of initial presentation was required. Lesion characteristics were evaluated by assessing size, location, and Hefti staging. Both surgical and nonoperative treatments were recorded. Patients with unilateral osteochondritis dissecans were compared to those with bilateral disease.
Results:
Eighty patients, 63 males (79%) and 17 females (21%), with an average age of 13.1 years old, were included. Twenty (25%) of the presenting/symptomatic lesions were deemed stable on magnetic resonance imaging. A positive correlation between lesion size and Hefti classification was appreciated. Twelve patients (15%) were found to have bilateral osteochondritis dissecans on contralateral imaging. There was no significant difference in skeletal maturity between patients with bilateral versus unilateral disease. Fifty-two patients (77%) with unilateral disease underwent surgical intervention, while 9 (75%) of those with bilateral disease underwent surgery on either knee. In patients with an asymptomatic contralateral lesion, 67% ultimately underwent surgical intervention on the contralateral knee.
Conclusions:
In patients presenting with unilateral osteochondritis dissecans symptoms, there was a 15% prevalence of bilateral disease, with no difference in age, sex, physeal status, or lesion characteristics between patients with unilateral vs bilateral osteochondritis dissecans lesions. Given the prevalence of asymptomatic contralateral lesions and the required intervention, this study supports early bilateral radiologic knee evaluation.
Level of evidence:
IV, Retrospective Case series.
Introduction
Osteochondritis dissecans (OCD) is a focal, idiopathic alteration of the subchondral bone that can lead to secondary articular cartilage disruption.1 –4 Much controversy has surrounded the exact etiology of OCD, ranging from inflammation and ischemia to microtrauma and genetic predisposition.2,5 –7
Many have hypothesized that a series of repetitive microtrauma events may lead to subsequent stress reaction and stress fracture of the subchondral bone, which with inadequate healing, may lead to fragmentation and fragment separation.2,8 –10 This theory has been debated in the literature, with many patients presenting with knee OCD without a clear history of injury or high activity level or without any symptoms. 2 Hereditary factors have also been proposed for several decades, with a recent genome-wide association study suggesting specific candidate loci in juvenile OCD.7,11,12 In addition, in the last several years, both animal and human studies have further investigated and garnered evidence supporting diminished vascularity as an underlying component of OCD development.13 –15 While there is no known discreet disease etiology at this time, disease presentation and progression are likely multifactorial.
The incidence of knee OCD in the juvenile population has been estimated anywhere from 9.5 to 29 per 100,000, with a male predominance of 5:3.8,16,17 Isolated lesions occur considerably more frequently than multifocal lesions, with multifocal knee OCD ranging in prevalence from 15% to 30%.8,18,19 While multifocal OCD involves more than one lesion in either the ipsilateral or contralateral knee, the incidence of bilateral OCD continues to be examined in the literature.20,21
The prevalence of bilateral OCD in pediatric and adolescent patients presenting specifically with unilateral knee pain is not well established. Younger age has been identified as an independent factor in healing, highlighting the importance of early identification, evaluation, and potential treatment of asymptomatic lesions before physeal closure and skeletal maturity.2,4,8,18
The primary aim of this study is to determine the prevalence of bilateral OCD in pediatric and adolescent patients presenting with unilateral symptoms. The secondary goal is to compare the presenting OCD lesion characteristics and treatment, including required surgical intervention, between patients with unilateral OCD and patients with bilateral disease.
Materials and methods
Following Institutional Review Board (IRB) approval, an electronic medical record database at a large, metropolitan, tertiary care pediatric center was queried to identify patients 18 years old or younger diagnosed with OCD of the knee from 2003 to 2016.
Patients were included in the study only if they had a confirmed diagnosis of OCD of the knee and presented with unilateral knee pain. Contralateral knee imaging of the asymptomatic knee obtained within 1 year of initial presentation (routine practice for several physicians in the group) was required to detect the presence of asymptomatic contralateral knee lesions. Clinical charts were comprehensively reviewed to ensure that patients with contralateral knee pain at the first visit or a history of contralateral knee pain were excluded from the study. Other exclusion criteria included radiological imaging (XR or MRI) limited to one knee only and osteochondral defects/lesions and/or chondral defects/lesions not associated with osteochondritis dissecans (e.g. patients with cartilage injury from patellar dislocation). While 250 patients in total returned from our initial search, only 80 ultimately met the criteria for the study. Many patients were excluded for meeting more than one exclusion criterion, with at least 32 patients not having bilateral imaging, at least 28 patients having bilateral symptoms at presentation, and the remainder excluded due to having prior surgery, incorrect coding, OCD of a different joint (not the knee), age outside of our study parameters, date outside of our study parameters, and/or no available imaging of the symptomatic side.
Demographic information was collected for all subjects including age, sex, BMI, physeal status/skeletal maturity on imaging, and presenting lesion laterality. Lesion location in both the coronal and sagittal planes was recorded according to the Cahill and Berg classification system (Figure 1). 18 Lateral femoral condyle lesions were defined as those located in regions 1 and 2 in the coronal plane, while those located in regions 4 and 5 were considered medial femoral condyle lesions. Trochlear lesions were confined to region 3. For lesions that spanned multiple regions, the region that contained the majority of the lesion was documented. Patellar lesions were documented separately. OCD lesion dimensions (width, length, depth) were measured on both XR and MRI.
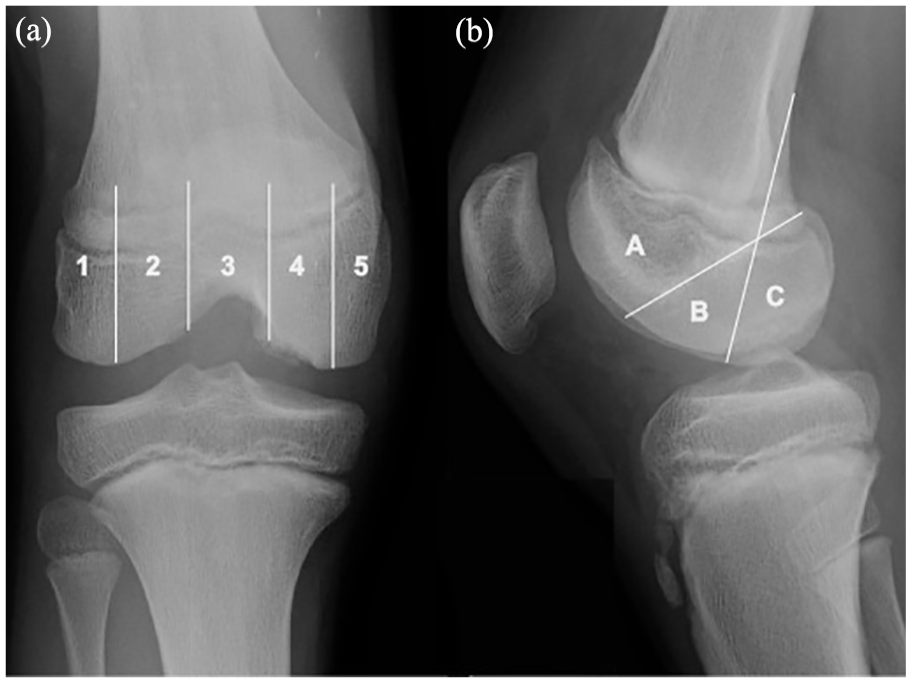
Anteroposterior (a) and lateral (b) radiographs of a skeletally immature male with an OCD lesion of the posteromedial knee. Utilizing the Cahill and Berg OCD classification system 18 overlying the radiograph, this example specifically demonstrates the patient’s OCD lesion primarily confined to region “4” on the AP view (a) and region “C” on the lateral view (b).
Lesion severity was determined using the Hefti classification system 19 and was performed independently by a pediatric orthopedic sports medicine fellow and a senior orthopedic surgery resident. Any discrepancy in Hefti stage classification was resolved by a pediatric sports medicine-trained attending surgeon (XXX). Hefti grades 1 and 2 were considered stable lesions and grades 3, 4, and 5 were considered unstable. Hefti grade 3 lesions were considered unstable because of the breach of the articular cartilage and subchondral plate. OCD treatment algorithms (both surgical and nonoperative) were recorded. Patients with unilateral OCD of the knee were then compared to those with bilateral OCD.
Measures of clinical, radiologic, and surgical characteristics were summarized using descriptive statistics. Comparison of epidemiologic factors, including age, sex, body mass index (BMI), laterality of symptoms, and skeletal maturity as well as ultimate treatment intervention between groups were conducted using Fisher’s exact tests for categorical variables, and independent-sample t tests or Wilcoxon rank sum tests for continuous variables. All tests were two-sided and a p value < 0.05 was considered statistically significant. In analyzing the Hefti classification data, following initial validity checks, one-way analysis of variance (ANOVA) tests were performed between the aggregated Hefti classifications. All statistical analyses and generation of figures were carried out using R v. 3.6.1 (R Foundation, Vienna, Austria).
Results
Patient demographics
Eighty patients, 63 males (79%) and 17 females (21%), with an average age of 13.1 ± 2.2 years old (range: 8–18), were included in the study. Forty-four (55%) patients presented with right-sided knee symptoms and 36 (45%) with left knee symptoms. Mean body mass index (BMI) was 21.1 ± 4.60, and the average length of follow-up was 2.6 years (Table 1).
Patient demographics.
Lesion characteristics of the primary knee
Analyzing the symptomatic OCD lesions for which patients presented to the clinic (i.e. “primary knee” lesions), 57 (71.2%) were located on the medial femoral condyle and 11 (13.8%) on the lateral femoral condyle. Twelve (15%) lesions were confined to the patella or trochlea. Excluding the trochlear and patellar lesions, 58 (85%) were located in region B, and 10 (15%) were located in region C of the Cahill and Berg Classification on lateral radiographs (Figure 1(b)). All primary knee lesion dimensions were measured on MRI and further classified based on Hefti grade (Figure 2). Twenty (25%) of these OCD lesions were deemed stable on MRI evaluation, per Hefti criteria.
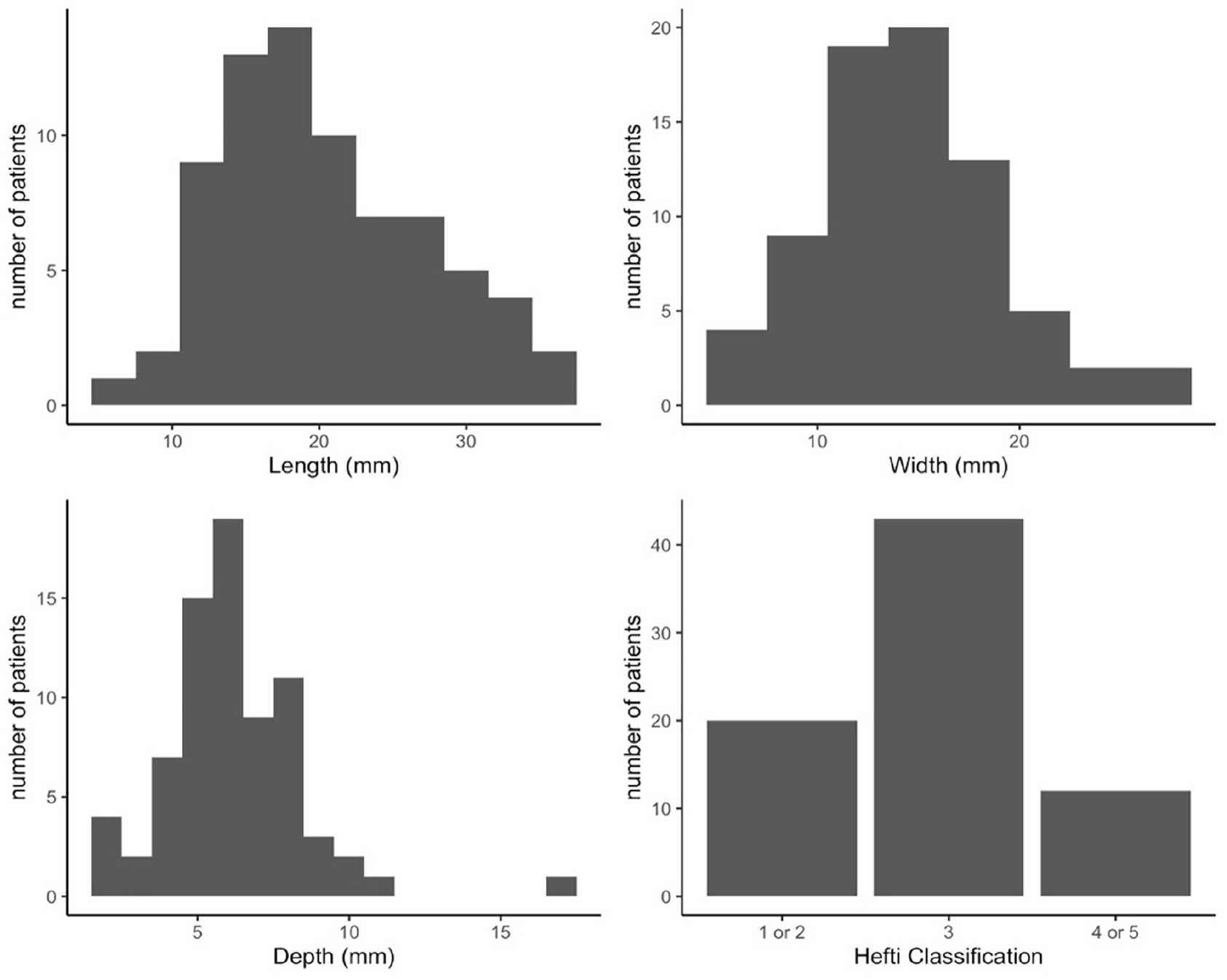
Graphical representation of
A volumetric analysis was performed to quantify an estimate of the overall size of OCD lesions by multiplying its measured length by width by depth. A log of this variable was taken to normalize the distribution. A positive association was found between OCD lesion volume and Hefti classification, with larger lesions associated with higher Hefti stages and unstable features (ANOVA p < 0.005, (Figure 3). Similarly, in examining OCD lesion depth alone, a positive association was found, with deeper lesions associated with higher Hefti staging (ANOVA p < 0.005, (Figure 4).
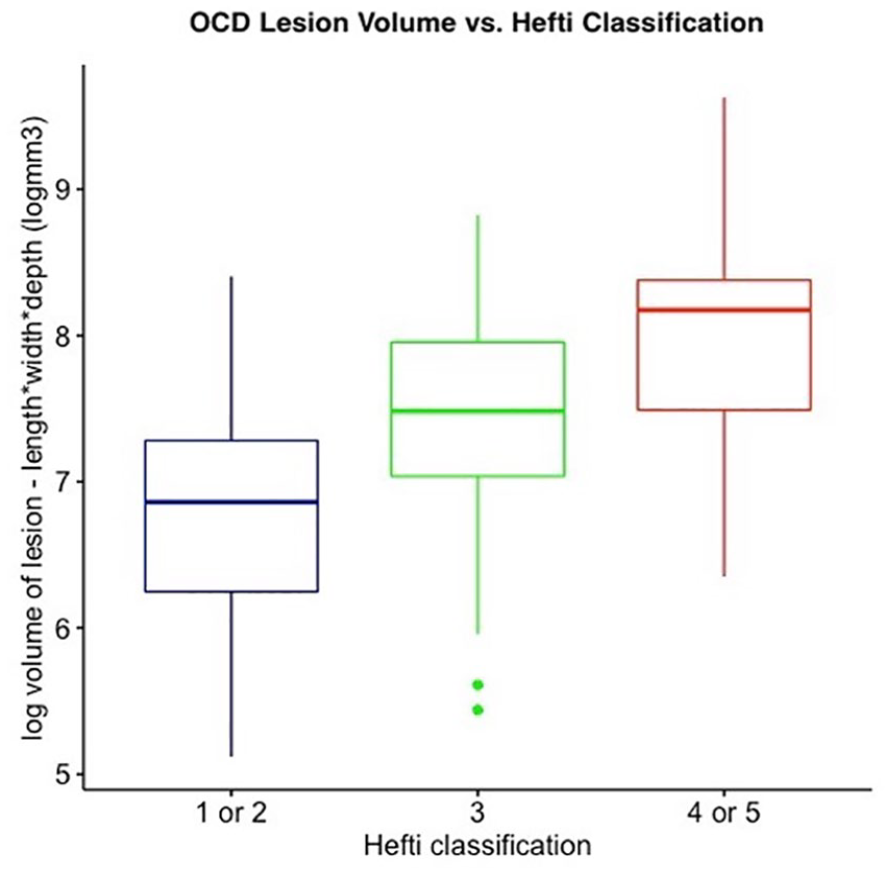
Box plot of log OCD lesion volume (length × width × depth, measured on MRI) versus Hefti classification of OCD lesion stability, depicting a positive association (ANOVA p < 0.005).
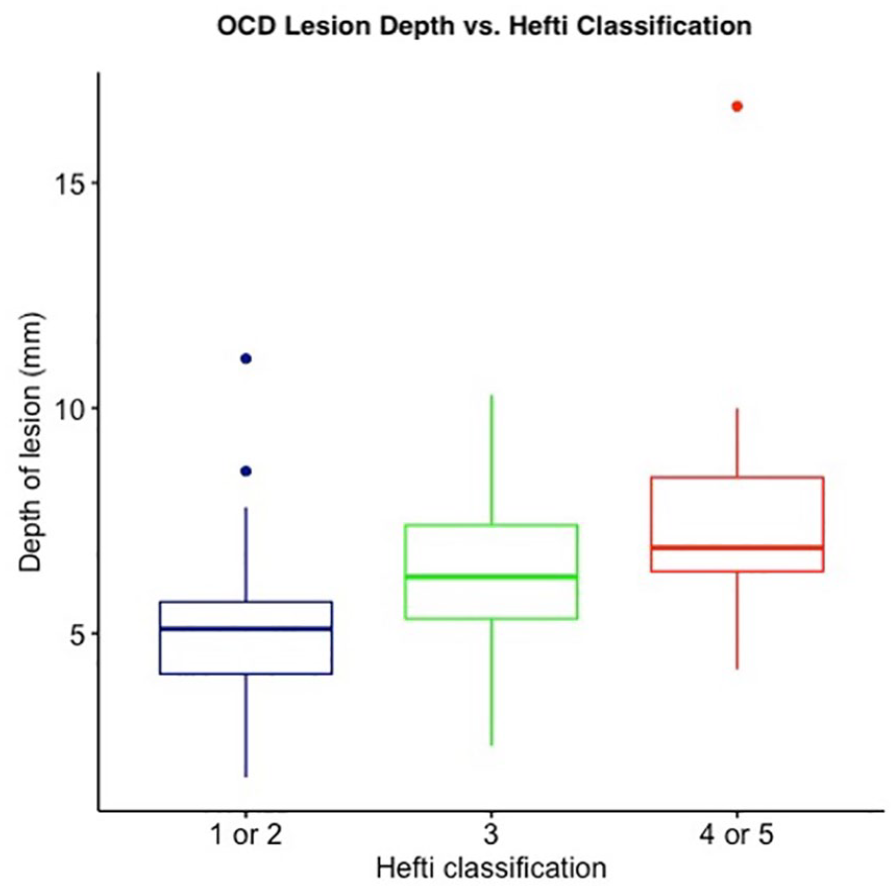
Box plot of OCD lesion depth (measured on MRI) versus Hefti classification of OCD lesion stability, depicting a positive association (ANOVA p < 0.005).
Unilateral versus bilateral groups
In the overall cohort of 80 patients presenting with unilateral OCD symptoms, 12 patients (15%) were found to have bilateral OCD on contralateral imaging. Five of the contralateral lesions (42%) were considered stable on MRI.
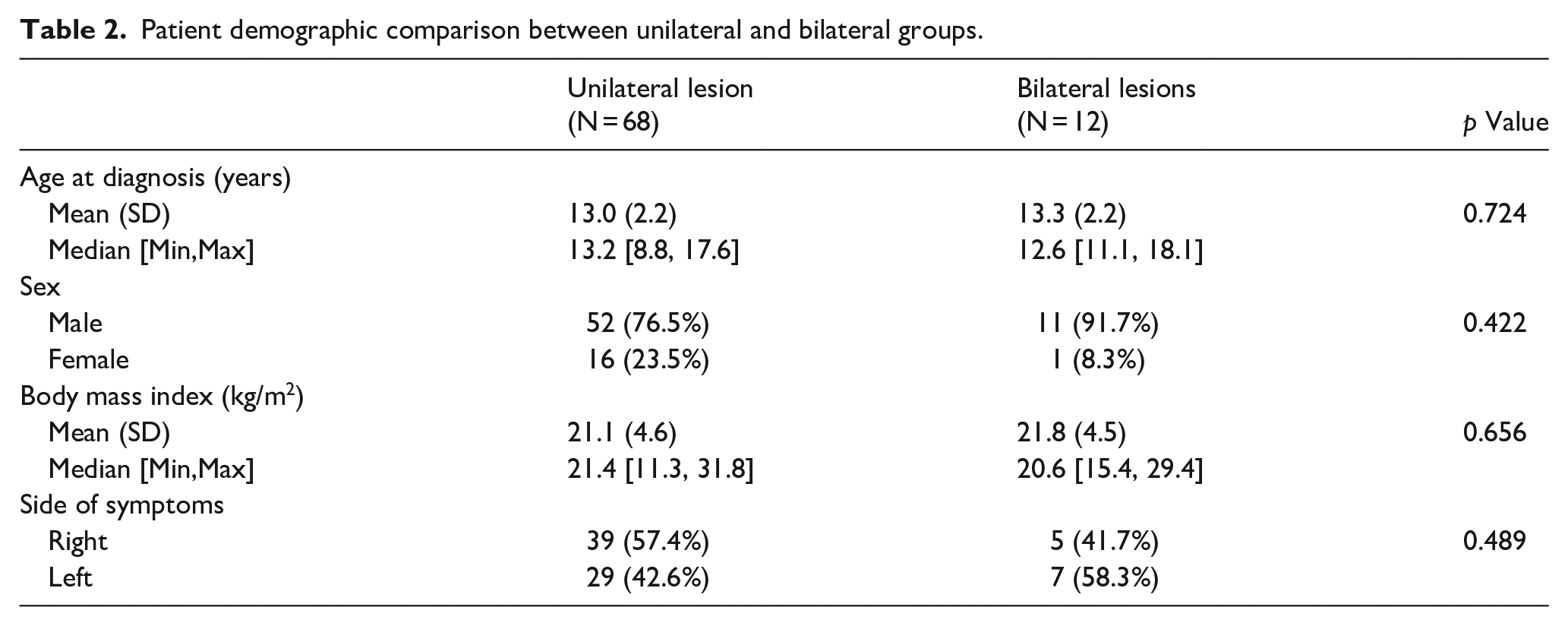
In a comparison between the unilateral and bilateral OCD groups, there was no significant difference in age of presentation, sex, BMI, or laterality of the symptomatic primary knee (Table 2).
Patient demographic comparison between unilateral and bilateral groups.
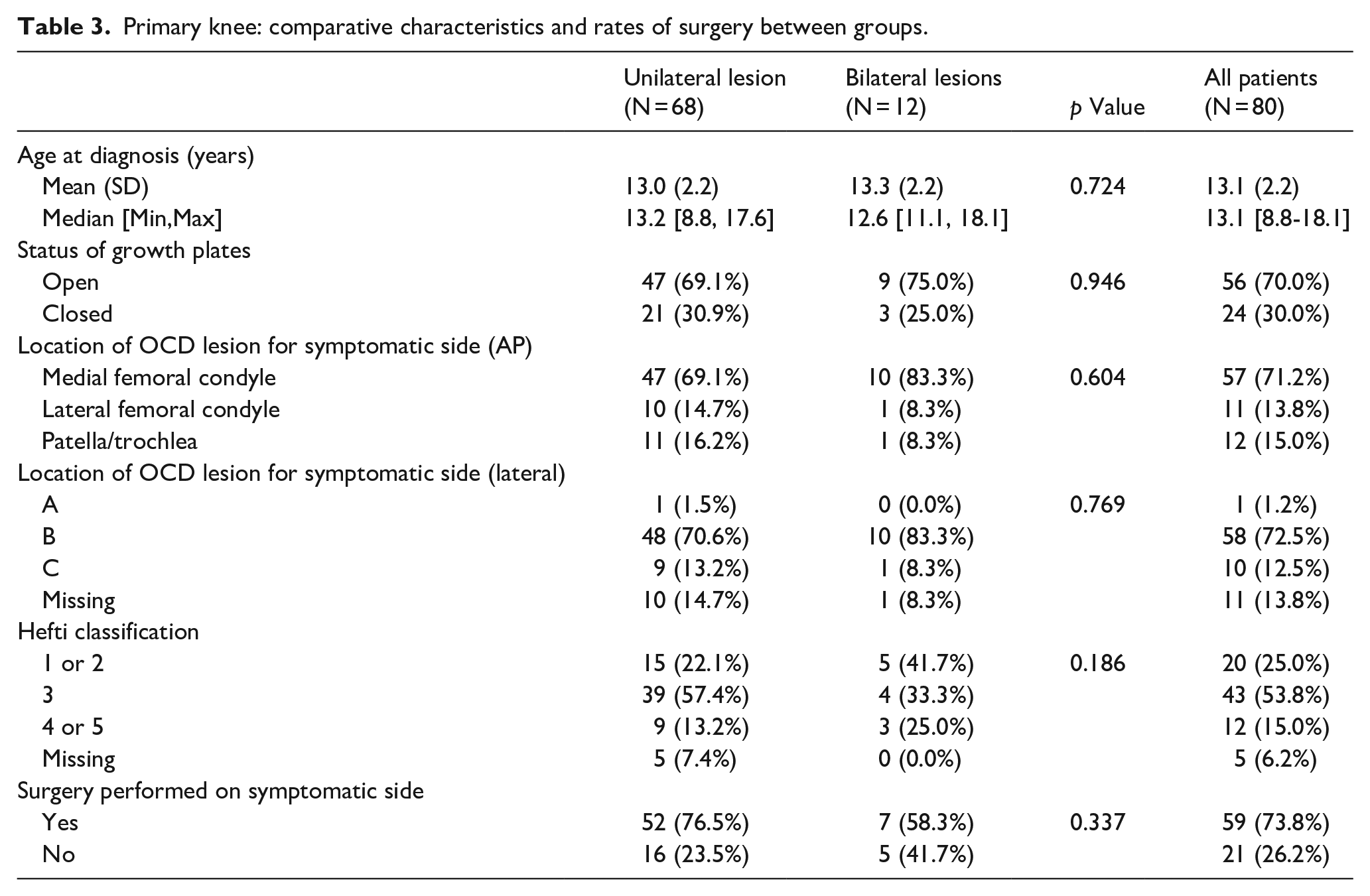
Furthermore, there was no significant difference in skeletal maturity between patients with bilateral versus unilateral OCD lesions. Nor were there any statistically significant differences in presenting lesion location or size. Comparison of the Hefti MRI classification of the primary knees between the two groups was also similar, and the rate of surgery performed on the symptomatic side demonstrated no statistically significant difference between the unilateral and bilateral cohorts (Table 3).
Primary knee: comparative characteristics and rates of surgery between groups.
Fifty-two patients (77%) with unilateral OCD underwent surgical intervention, while 9 (75%) of those with bilateral disease underwent surgery for at least one knee. More specifically, in patients with bilateral OCD, 67% ultimately underwent surgical intervention on the contralateral knee, which had been asymptomatic at presentation (Table 4).
Rates of surgery in patients with bilateral OCD.

Discussion
In patients presenting with strictly unilateral knee pain and diagnosed with an OCD lesion in the symptomatic knee, this study demonstrated a 15% prevalence of bilateral OCD lesions. That is to say that roughly one in seven patients who presented with unilateral knee pain had an asymptomatic OCD lesion on their contralateral side.
Obtaining bilateral knee imaging in those patients presenting with unilateral knee OCD is not uniform practice in many centers, contributing to the lack of research into the bilateral nature of the disease and the course of disease progression. 22 In a recent study, Cooper et al. reviewed a series of patients presenting for juvenile OCD, with some endorsing bilateral knee pain at presentation. They obtained contralateral x-rays in patients with an OCD lesion detected on the presenting side and found an incidence of 29% bilateral OCD of the knee, with 39% of the contralateral lesions being asymptomatic at presentation. 21 While prior studies such as this have examined the incidence of multifocal and bilateral knee OCD lesions, this study sought to determine the prevalence of bilateral OCD lesions in a patient population demonstrating no clinical signs or symptoms of a contralateral lesion.8,18,19,21
Interestingly, in comparing the demographic information between patients diagnosed with unilateral versus bilateral lesions in this study, there was no statistically significant difference in age of presentation or sex, which contrasts the study performed by Cooper et al. 21 identifying a younger age at presentation and female sex as risk factors for bilateral disease. Furthermore, our study demonstrated no statistically significant difference between skeletal maturity, measured by physeal status about the knee, or lesion dimensions in patients presenting with unilateral versus bilateral disease. And, in examining the presenting symptomatic knee OCD lesion for both the unilateral group and the bilateral group, there was no statistically significant difference between location or Hefti classifications. In other words, neither the location nor the stability of a unilateral lesion classified per the Hefti staging system necessarily makes a contralateral OCD lesion more likely.
There are several potential benefits to identifying and treating OCD lesions at a younger age and stage. 23 Wall et al. 24 demonstrated that in skeletally immature individuals with stable OCD lesions, 6 months of non-operative intervention resulted in progressive healing in about two-thirds of their study population. Imaging of the contralateral knee in patients presenting with unilateral OCD can potentially detect these lesions, prompting earlier intervention. In cases where surgery is indicated, other studies have suggested improved outcomes when surgical intervention occurs at an earlier age, demonstrating another potential benefit of earlier lesion identification. 25
In the literature, while surgical intervention for some OCD lesions has resulted in good functional outcomes, larger lesion size has been associated with lower nonoperative success and poorer outcomes.16,24,26 –28 Interestingly, this study detected a positive association between lesion size and Hefti classification. Specifically, examining overall lesion volume and lesion depth alone versus Hefti MRI grade demonstrated that larger and deeper OCD lesions tend to be more unstable. While somewhat intuitive, this knowledge can both help shape clinic conversations with patients and demonstrates additional utility in detecting lesions early.
In the subgroup analysis of the patients with bilateral OCD lesions, looking at the asymptomatic (i.e. incidentally found) OCD lesions on the contralateral side with MRI available for review (all but two patients), 50% presented as stable lesions, while 50% presented as Hefti grades 3 or 4. Ultimately, 58% of patients in the bilateral group underwent surgical intervention on the side of initial presentation, while 67% underwent surgery on the contralateral (initially asymptomatic). Overall, 75% underwent surgery on at least one knee, which was similar to the 77% surgical rate in the unilateral group. Interestingly, patients discovered to have bilateral OCDs may not be at increased risk of surgery compared to those with unilateral disease, based on the findings in this cohort.
There are several strengths as well as limitations to this study. Aside from the inherent limitations of a retrospective chart review in terms of data collection, there were unfortunately some patients excluded from the study secondary to imaging not available in the electronic medical record system. The authors felt it prudent to be able to evaluate all necessary imaging firsthand as opposed to basing inclusion in the study off of radiology reports in an effort to be as thorough and comprehensive as possible in presenting the data. Furthermore, especially in the younger patients presenting with reported OCD lesions, it is essential to be able to discern true OCD lesions from potential ossification variants. Gebarski and Hernandez 29 described several features favoring ossification variants over OCD including posterior femoral condyle location with intact overlying cartilage, lack of bone marrow edema, accessory ossification centers, and a few others. 21 Nonetheless, if there was any question regarding ossification variant (e.g. due to young patient age and/or bilateral lesions), the case in question was reviewed by one of the senior authors as well as a musculoskeletal-trained attending radiologist to determine inclusion or exclusion.
In addition, given one of the major requirements of the study was the necessity of contralateral knee imaging within a year of presentation, it is important to acknowledge the potential for selection bias. While many of the subjects included in the study were patients of treating physicians who routinely order bilateral knee imaging, it is possible that some were patients of treating physicians who chose to order contralateral imaging given a particularly large presenting lesion or severe symptoms, for example. Nonetheless, all patients included with bilateral imaging were completely asymptomatic on the contralateral side.
A related limitation of the study involved the small sample size in terms of the comparison between the unilateral and bilateral groups. While this was not the primary focus of the study, the analysis between groups was limited by this factor. With ultrasound evaluation gaining increasing popularity in clinical orthopedics in general, and recent studies beginning to investigate its potential role and validity in OCD detection, future studies may be able to take advantage of this imaging modality, capturing more patients during clinic visits.30,31
One of the greatest strengths of this study was its internal validity, established by the stringent inclusion criteria, limiting the patient population to those that presented with unilateral knee pain only. Although the data collection period was quite lengthy, 10+ years, if there was any ambiguity regarding presenting symptoms on the contralateral side, or a history of contralateral knee pain, these patients were excluded, ultimately reducing the final patient cohort. Future studies over longer periods of time should endeavor to include large sample sizes, which may generate more robust subgroup analyses of patients with bilateral OCD lesions. Ideally, as more treating physicians enhance protocols to include bilateral knee imaging in all patients with unilateral OCD lesions, the study population in later studies will have more included patients.
Conclusion
Given the prevalence of asymptomatic contralateral lesions and their subsequent intervention, the current study underscores the importance of obtaining bilateral radiographic imaging as a universal screening measure for adolescent and pediatric knee OCD, even in those presenting with no symptoms on the contralateral knee.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521231193711 – Supplemental material for Bilateral osteochondritis dissecans of the knee in pediatric and adolescent patients presenting with unilateral symptoms: An epidemiological and radiographic analysis
Supplemental material, sj-pdf-1-cho-10.1177_18632521231193711 for Bilateral osteochondritis dissecans of the knee in pediatric and adolescent patients presenting with unilateral symptoms: An epidemiological and radiographic analysis by Joseph L Yellin, Robert G Tysklind, Zaamin B Hussain, Evan T Zheng, Benton E Heyworth and Mininder S Kocher in Journal of Children’s Orthopaedics
Footnotes
Acknowledgements
There are no further acknowledgments.
Author contributions
Joseph L. Yellin—Conceptualization, methodology, data curation, resources, writing—original draft and review and editing. Robert G. Tysklind—conceptualization, methodology, data curation, resources, writing—original draft and review and editing. Zaamin B. Hussain—methodology, data curation, formal analysis, visualization, writing—original draft. Evan T. Zheng—methodology, data curation, formal analysis, visualization, writing—original draft. Benton E. Heyworth—conceptualization, methodology, writing—drafts, review and editing, supervision. Mininder S. Kocher—conceptualization, methodology, writing—drafts, review, editing, supervision, and project administration.
Compliance with ethical standards
Ethics approval was received by the Boston Children’s Hospital Institutional Review Board (IRB approval number: IRB-P00030609). As a retrospective study, informed consent was not provided.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: ICJME forms for each author were uploaded.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.