
Abstract
Background:
Thiel cadavers have been reported to have lifelike flexibility and mechanical properties, but whether they are useful for measurement of the ulnohumeral joint space (JS) is unclear. The contributions of the third and fourth digits and the second and fifth digits of the flexor digitorum superficialis (FDS) to elbow valgus stability are also unknown.
Purpose:
To (1) clarify whether Thiel cadavers can be used for JS measurement on ultrasound and (2) identify the contributions to valgus stability of the third and fourth digits and the second and fifth digits of the FDS.
Study Design:
Descriptive laboratory study.
Methods:
In experiment 1 (12 elbows from human volunteers and 12 elbows from Thiel cadavers), valgus stress was increased gradually from 0 to 30 to 60 N, and the JS was compared on ultrasound between groups at each load. In experiment 2 (13 elbows from Thiel cadavers), specimens were divided into 2 groups, and the JS was measured for group 1 with the FDS intact, with tendinous insertions of the third and fourth digits cut (3/4-cut state), and with tendinous insertions of all fingers cut (all-cut state); and for group 2 at intact FDS, with tendinous insertions of the second and fifth digits cut (2/5-cut state), and at all-cut.
Results:
In experiment 1, the rate of change of the JS increased significantly with elbow valgus stress in both humans and Thiel cadavers, with no significant difference between groups. In experiment 2, the JS was significantly greater in the 3/4- and 2/5-cut states compared with the intact state at both 30 N (Δ3/4-cut vs intact = 0.23 mm [P = .01]; Δ2/5-cut vs intact = 0.32 mm [P = .02]) and 60 N (Δ3/4-cut vs intact = 0.33 mm [P = .002]; Δ2/5-cut vs intact = 0.37 mm [P = .04]). There was no significant difference in JS measurements between the 3/4- and 2/5-cut states at any load.
Conclusion:
Thiel cadavers showed JS changes similar to those of humans when valgus stress was applied. The third and fourth digits and the second and fifth digits of the FDS were involved in valgus stability, and there was no difference in their respective contributions.
Clinical Relevance:
This study may help in identifying function of the FDS based on structure.
Ulnar collateral ligament (UCL) injury is one of the most frequent sports injuries in throwing athletes. 4 UCL injury is thought to occur as a result of repeated elbow valgus stress. 15 In anatomical studies, 5,8,21,23 biomechanical studies, 1,9,20,24,30 and studies using ultrasonography, 13,25 the forearm flexors have been found to be important for reducing elbow valgus stress on the UCL. In particular, the flexor digitorum superficialis (FDS) muscle has been reported to be the most important of the forearm flexors for reducing elbow valgus stress on the UCL. 13,25,30
With regard to the contribution of the FDS to elbow valgus stability, Hoshika et al 13 measured the ulnohumeral joint space (JS) when elbow valgus stress was applied to humans; in their study, the second, third, and fourth digits of the FDS were contracted individually. The authors reported that all digits were involved in elbow valgus stability, especially the second and third digits. Furthermore, with regard to the anatomy of the FDS, it has been reported that the third and fourth digits originate from the radius, the anterior common tendon (ACT), and the posterior common tendon (PCT) in all cases, and in most cases the second and fifth digits originate from the ACT, the PCT, the anterior bundle of the UCL, and other soft tissues of the elbow. 21 From the anatomical findings, it is presumed that the third and fourth digits of the FDS are involved in ulnohumeral joint stability via the ACT and PCT, and the second and fifth digits of the FDS are involved in ulnohumeral joint stability via the ACT, PCT, and the anterior bundle of the UCL. However, differences in their contributions to elbow valgus stability have not been examined.
With regard to the examination of elbow valgus stability, previous studies have measured changes in the elbow valgus angle and the JS when the soft tissue of the elbow joint was removed in fresh cadavers. 2,24,30 Fresh cadavers have the disadvantage of high infection risk, limited supply, and short preservation periods. 18 On the other hand, Thiel cadavers have been reported to have low infection risk and long preservation periods. 11,18,29 In addition, the preparation of Thiel cadavers has been reported to result in a fixation method that can maintain lifelike flexibility and mechanical properties 11,16,18,22 and to allow reliable ultrasound imaging. 16,22 However, it has not been demonstrated whether Thiel cadavers are considered appropriate for JS measurement. In addition, ligaments and tendons have viscoelastic properties such as cyclic creep with increased strain when repeated stress is applied, as in the fatigue test. 6,10 Therefore, JS stress in Thiel cadavers should also be affected by repeated elbow valgus stress, but this has not been reported.
This study consisted of 2 experiments. The purpose of experiment 1 was to clarify whether the JS of human volunteers and of Thiel cadavers show similar changes with increasing elbow valgus stress as well as repeated elbow valgus stress. The purpose of experiment 2 was to clarify the contributions of the third and fourth digits and the second and fifth digits of the FDS to elbow valgus stability using the Thiel cadaver. It was hypothesized that in experiment 1, JS would show similar changes in human volunteers and Thiel cadavers and that in experiment 2, both the third and fourth digits and the second and fifth digits would be involved in elbow valgus stress.
Methods
Participants
This study was performed in accordance with the Declaration of Helsinki after approval by the ethics committee of our institution. In experiment 1, we evaluated 12 elbows from 6 healthy male adult volunteers (mean age, 21.8 ± 1.2 years) and 12 elbows from 6 Japanese Thiel cadavers (mean age at death, 87.8 ± 5.8 years; 4 male, 2 female). In experiment 2, we evaluated 13 elbows from 7 Japanese Thiel cadavers (mean age at death, 88.8 ± 6.4 years; 7 sides from men, 6 sides from women; 7 right sides, 6 left sides). All Thiel cadavers were obtained from the anatomy program of our university. Human volunteers with a history of orthopaedic disease in the elbow joint and those with elbow joint pain at the time of measurement were excluded, and Thiel cadavers with osteophytes or a surgical history were excluded.
Ulnohumeral JS Measurement
All JS measurements were performed by a physical therapist (K.M.) experienced in ultrasound. The human volunteers sat in a chair with the shoulder abducted and in external rotation of 90°, with the elbow flexed to 30° and forearm supination in a Telos stress device (Aimedic MMT) (Figure 1A). The Thiel cadavers were placed in the supine position, with the shoulder abducted and in external rotation of 90°, with the elbow flexed to 30° and forearm supination in the Telos device (Figure 1B). The wrist joint was fixed in the middle position of palmar-dorsal flexion, and the fingers were fixed in the extended position.
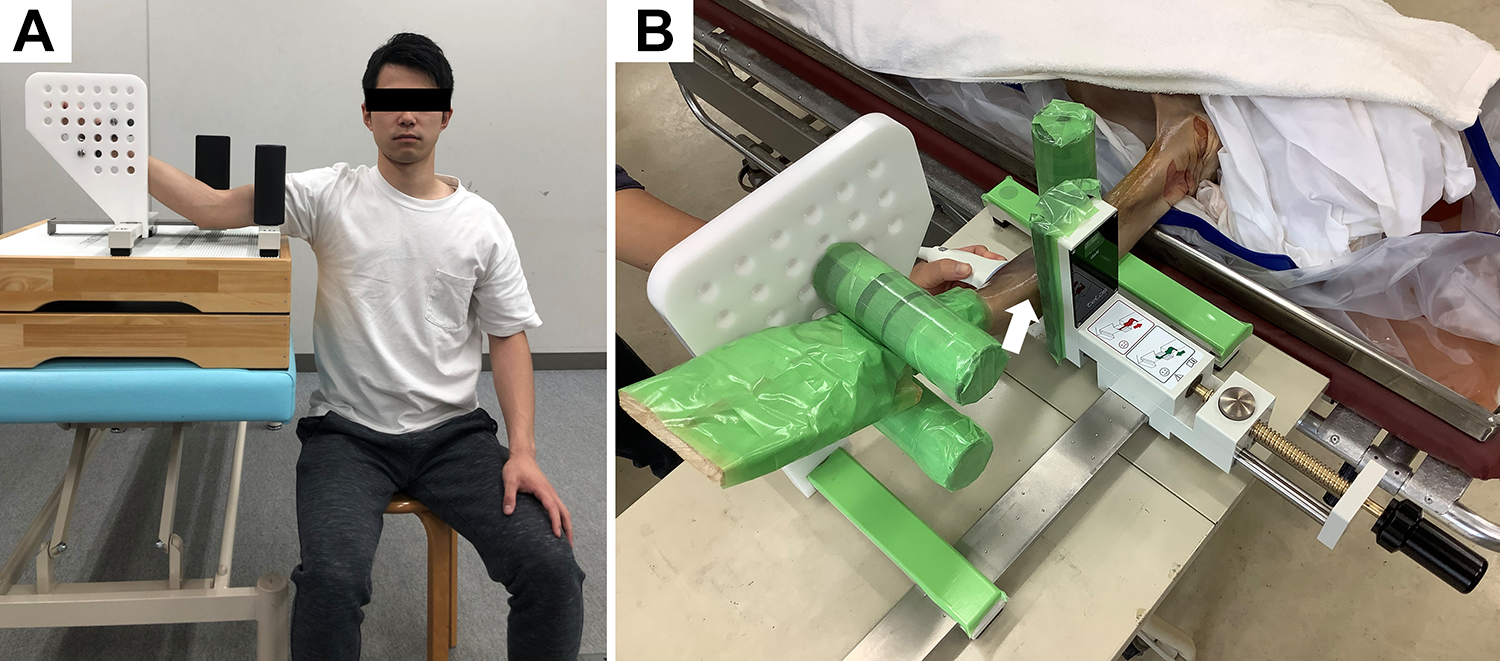
Measurement positions for ultrasound imaging. (A) The volunteer sat in a chair, with the shoulder in abduction and external rotation of 90°, with elbow flexion of 30° and forearm supination in the Telos stress device. (B) The Thiel cadaver was placed in the supine position with the shoulder in abduction and external rotation of 90° and the elbow at 30° of flexion and forearm supination in the Telos stress device. The arrow indicates the elbow joint.
JS measurement was performed using ultrasonography (LOGIQ eV2; GE Healthcare) with a 12-MHz linear probe. As per a previous study by Ciccotti et al, 3 the probe was placed on the medial side of the elbow joint, and the anterior bundle of the UCL was visualized with the trochlea of the humerus and the sublime tubercle of the ulna as landmarks. Using the calipers of the ultrasonography device, the JS was measured as the distance between the distal-medial corner of the trochlea of the humerus and the proximal edge of the sublime tubercle of the ulna (Figure 2).

Ultrasound measurement of the ulnohumeral joint space (JS) in (A) a human volunteer and (B) a cadaveric specimen. Using the calipers of the ultrasound device, the JS was measured as the distance between the distal-medial corner of the trochlea of the humerus and the proximal edge of the sublime tubercle of the ulna (asterisks). MEC, medial epicondyle of the humerus; ST, sublime tubercle of the ulna; TR, trochlea of the humerus.
Experimental Procedures
Experiment 1
For the measurement protocol, the Telos device was first set to 0 N, and 3 ultrasound images of the medial part of the elbow were taken. The load was then increased gradually at 10 N/s, and when 30 N and 60 N were reached, 3 ultrasound images were taken within 10-second intervals (Figure 3). The average value of the JS from the 3 images at each load was used. The same protocol was used for the cadaveric measurements, but in addition, loading was repeated 3 times to examine the effect of repeated elbow valgus stress on the JS. The measurement interval between the 3 consecutive measurements was 15 minutes (Figure 3).
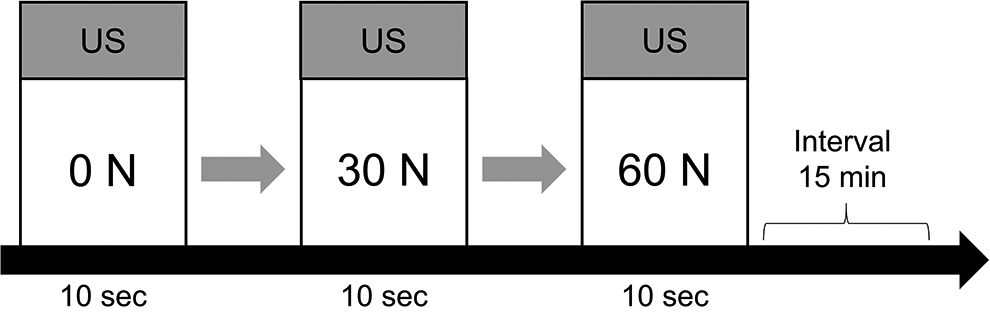
Interval measurement protocol of the ulnohumeral joint space (JS). First, the Telos device was set to 0 N, and 3 ultrasound (US) images of the medial part of the elbow were taken. The load was then increased gradually at 10 N/s, and, when 30 and 60 N were reached, 3 US images were taken within 10 seconds at each point. The mean JS value from the 3 images at each load was used.
We examined the intersession reliability of the JS measurements in the human participants by retesting after an interval of 2 to 7 days. In the cadaveric specimens, the values of the first and second of the 3 consecutive measurements were used to test intersession reliability.
Experiment 2
The skin of the specimens was incised, 3 cm long by 4 cm wide, at the wrist joint, subcutaneous tissues were removed, and the tendinous insertions of the FDS were dissected carefully. The intact state was defined as the state when the tendinous insertions of the FDS were dissected.
The 13 elbows were divided into 2 groups. In group 1 (n = 7; 4 right and 3 left elbows), the JS was measured in the order of intact FDS, with the tendinous insertions of the third and fourth digits cut (3/4-cut state), and with the tendinous insertions of the third and fourth digits and the second and fifth digits cut (all-cut state). In group 2 (n = 6; 3 right and 3 left elbows), the JS was measured in the order of intact FDS, with the tendinous insertions of the second and fifth digits cut (2/5-cut state) and the all-cut state. The measurement protocol for each state was performed as in experiment 1, and the measurement interval under each condition was 15 minutes.
Statistical Analysis
Experiment 1
Intersession JS measurement reliability was assessed using the intraclass correlation coefficient (ICC), in which the ICC values were interpreted according to the criteria of Landis and Koch 17 : <0.00 = poor reliability; 0.00-0.20 = slight; 0.21-0.40 = fair; 0.41-0.60 = moderate; 0.61-0.80 = substantial; and 0.81-1.00 = almost perfect. The minimum detectable difference at the 95% CI (MDD95) was calculated using the following equation 27 : MDD95 = z × standard error of measurement × √2, where z is 1.96 and the standard error of measurement is SD√(1−ICC). The MDD expresses measurement error in the same unit as the original value, which facilitates clinical interpretation. 26 If the difference between 2 measurements is within the range of the MDD95, it is within the measurement error by 95%.
The rate of change of the JS was calculated by normalizing the measured values at 30 and 60 N with the value at 0 N. To examine whether the JS showed similar changes with increased elbow valgus stress regardless of patient type (humans vs cadavers), a split-plot analysis of variance (ANOVA; patient type × load size) was performed for the measured values and the rate of change of the JS. In addition, a post hoc analysis of load size was performed using 1-way repeated-measures ANOVA with Bonferroni correction or the paired t test. The Student t test was used to analyze patient type. To examine the effect of repeated elbow valgus stress on the JS of the Thiel cadavers, a 2-way repeated-measures ANOVA (measurement session × load size) was performed. In addition, a post hoc analysis of load size was performed using 1-way repeated-measures ANOVA with Bonferroni correction. For all analyses, the level of significance was set at P < .05.
Experiment 2
The measured values of the JS were used for statistical analysis. To examine the effect of group, a Student t test was performed to compare the JS between groups 1 and 2 in the intact and all-cut states. To examine whether the third and fourth digits and the second and fifth digits of the FDS were involved in elbow valgus stability, the paired t test was performed for the JS between the intact state and the 3/4-cut state in group 1 and between the intact state and the 2/5-cut state in group 2. To compare elbow valgus stability related to the third and fourth digits with that related to the second and fifth digits, the Student t test was performed to compare the JS of the 3/4-cut and 2/5-cut states. For all analyses, the level of significance was set at P < .05.
Results
Experiment 1
JS Measurement Reliability and MDD95
The ICC (1,3) for the intersession JS measurements was 0.87 to 0.98, indicating almost-perfect reliability (Table 1). 17
Intersession JS Measurement Reliability and MDD95 a

a Data are reported as mean ± SD. ICC, intraclass correlation coefficient; JS, joint space; MDD95, minimal detectable difference at the 95% CI.
JS Measurement in Humans and Cadavers
Table 2 lists the JS measurements and rates of change by load size and patient type. Split-plot ANOVA for JS measurements showed no interaction effect [F (2, 34) = 0.63; P = .49; partial η2 = 0.02]. There was a main effect of patient type [F (1, 22) = 6.12; P = .02; partial η2 = 0.21] and of load size [F (2, 34) = 81.58; P < .001; partial η2 = 0.78]. Post hoc analysis showed that the JS was significantly greater in human volunteers than in Thiel cadavers at 0, 30, and 60 N (P = .01, .02, and .04, respectively). In addition, the JS was significantly greater at 30 versus 0 N and at 60 versus 0 and 30 N in both humans and cadavers (humans: P < .001, <.001, and <.05, respectively; cadavers: P < .01, <.001, and <.001, respectively).
JS Measurements and Rates of Change in Human Volunteers and Thiel Cadavers a

a Data are reported as mean ± SD. Rate of change was calculated by normalizing the JS values at 30 N and 60 N with that at 0 N. JS, joint space.
bP < .05 vs Thiel cadavers.
cP < .001 vs 0 N.
dP < .05 vs 30 N.
eP < .01 vs 0 N.
fP < .001 vs 30 N.
gP < .01 vs 30 N.
Split-plot ANOVA for the rate of change showed no interaction effect [F (1, 22) = 2.70; P = .11; partial η 2 = 0.10], and no main effect of patient type [F (1, 22) = 1.01; P = .32; partial η 2 = 0.04]. There was a main effect of load size [F (1, 22) = 38.68; P < .001; partial η 2 = 0.63]. Post hoc analysis showed that the change in JS was significantly greater at 60 versus 30 N in both humans (P = .008) and cadavers (P < .001).
Effect of Repeated Elbow Valgus Stress on Cadaveric JS
Table 3 shows the JS measurements in Thiel cadavers after repeated elbow valgus stress. Two-way repeated-measures ANOVA showed no interaction effect [F (4, 44) = 0.29; P = .88; partial η2 = 0.02] and no main effect of measurement session [F (1, 22) = 1.43; P = .25; partial η2 = 0.11]. There was a main effect of load size [F (2, 22) = 45.04; P < .001; partial η2 = 0.80]. Post hoc analysis showed that the JS was significantly greater at 30 versus 0 N and at 60 versus 0 and 30 N (first session: P = .002, <.001, and <.001, respectively; second session: P = .002, <.001, and .005, respectively; third session: P = .002, <.001, and <.001, respectively).
Effect of Repeated Elbow Valgus Stress on the JS of Thiel Cadavers a
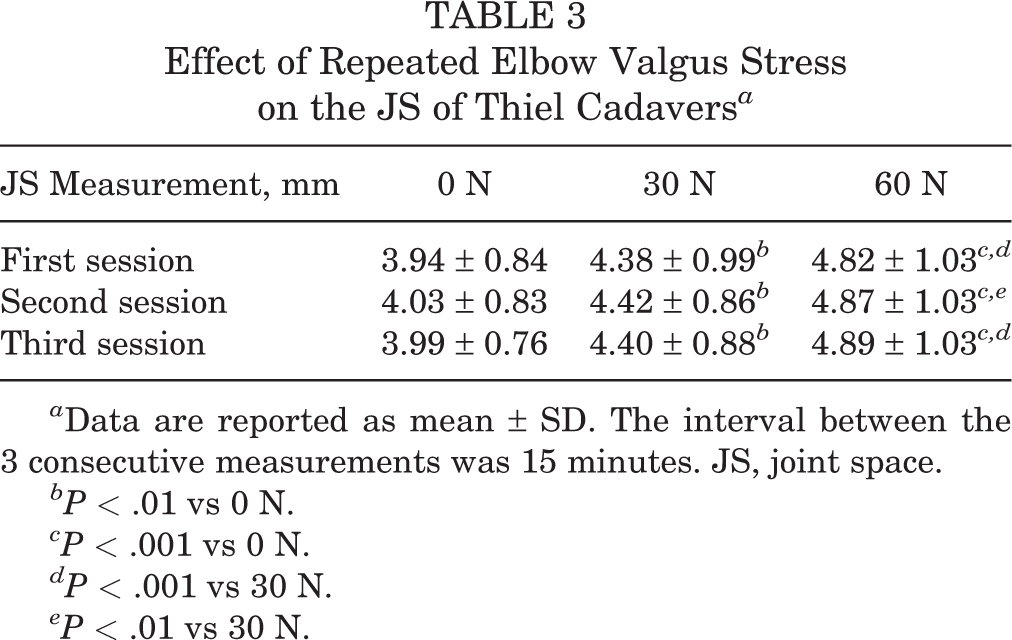
a Data are reported as mean ± SD. The interval between the 3 consecutive measurements was 15 minutes. JS, joint space.
bP < .01 vs 0 N.
cP < .001 vs 0 N.
dP < .001 vs 30 N.
eP < .01 vs 30 N.
Experiment 2
There were no significant between-group differences in the JS at 0, 30, or 60 N in either the intact (Figure 4A) or the all-cut (Figure 4B) state. The JS was significantly greater in the 3/4-cut and 2/5-cut states than in the intact state at both 30 N (Δ3/4-cut vs intact = 0.23 mm [P = .01]; Δ2/5-cut vs intact = 0.32 mm [P = .02]) and 60 N (Δ3/4-cut vs intact = 0.33 mm [P = .002]; Δ2/5-cut vs intact = 0.37 mm [P = .04]) (Figures 5A and 5B). There were no significant differences in the JS between the 3/4-cut state and 2/5-cut state at 0, 30, or 60 N (Figure 5C).

Comparison of joint space between groups 1 and 2 in the (A) intact state and (B) all-cut state, in which the tendinous insertions of the third and fourth digits and the second and fifth digits of the flexor digitorum superficialis (FDS) were cut.

Changes in the joint space made by cutting the tendinous insertions of the FDS. Comparison between (A) intact versus third and fourth FDS digits cut (3/4 cut), (B) intact versus second and fifth FDS digits cut (2/5 cut), and (C) 3/4-cut versus 2/5-cut. Significant difference: *P < .05, paired t test; † P < .01, paired t test. FDS, flexor digitorum superficialis.
Discussion
Our experiments demonstrated similar JS changes with increasing elbow valgus stress between human volunteers and cadavers treated with the Thiel method. We also found that the third and fourth digits and the second and fifth digits of the FDS contributed similarly to the stability of the elbow undergoing valgus stress. To the best of our knowledge, no studies have examined whether JS measurements in Thiel cadavers is useful, and none have examined the contributions of the third and fourth digits and the second and fifth digits of the FDS to elbow valgus stability.
Based on the results of experiment 1, the measured value and rate of change of the JS increased significantly with elbow valgus stress in both humans and cadaveric specimens. The measured values of the JS were significantly greater in the humans than the cadavers, but there was no significant difference in the rate of change between the groups. Considering these results, Thiel cadavers appear to be as useful as fresh cadavers for evaluating elbow valgus stability. 2,12 In addition, there was no significant difference in the JS values of cadaveric specimens between measurement sessions. Therefore, repeated elbow valgus stress in Thiel cadavers appears unlikely to have affected the JS in the present study.
Based on the results of experiment 2, there were no significant differences in the JS between groups 1 and 2 in the intact and all-cut states. Therefore, there appears to be no effect of individual specimens between groups. At 0 N, there were no significant differences in the JS between either the 3/4-cut and intact states or the 2/5-cut and intact states. On the other hand, at 30 and 60 N, the JS was significantly greater in the 3/4- and 2/5-cut states than in the intact state. Therefore, the third and fourth digits and the second and fifth digits of the FDS may be involved in elbow valgus stability. In addition, there were no significant differences in the JS between the 3/4- and 2/5-cut states at 0, 30, or 60 N. The muscle force was reported previously to be proportional to physiological cross-sectional area, 19 and a previous study suggested that there may be no difference between the physiological cross-sectional area of the third and fourth digits and the second and fifth digits of the FDS. 21 Considering these results, there appears to be no difference in the contribution to elbow valgus stability between the third and fourth digits and the second and fifth digits of the FDS.
For stabilization of the medial side of the elbow, the pronator teres muscle, the FDS, the flexor carpi ulnaris muscle, and the brachialis muscle are thought to work together to transmit the muscle power to the ulnohumeral joint via the ACT and PCT. 14 In addition, it has been suggested that the contraction of all fingers can be involved in ulnohumeral joint stability via the ACT and PCT, because all digital muscle fibers of the FDS originate from the ACT and PCT. 21 A previous study reported that injury care programs should incorporate FDS exercises of these fingers because they, particularly the index and middle fingers, contribute the most to stabilization against valgus stress. 13 However, considering the origin structure of the FDS 21 and the results of the present study, from the viewpoint of transmitting muscle force to the ACT and PCT, it appears necessary to perform exercises for all digits of the FDS in a well-balanced manner, rather than specific finger exercises.
This study has several limitations. First, the dominant hand of the donors was unknown, and whether donors had been involved in overhead sports during their lifetime was also unknown. A previous study reported that the difference in the JS between valgus stress and no valgus stress was significantly higher in the dominant arm than in the nondominant arm. 28 A previous study also reported that the JS of professional pitchers was significantly greater in the dominant arm than in the nondominant arm. 3 In the present study, the numbers of left and right samples were balanced as much as possible to minimize these effects. Therefore, the effects of the dominant arm and involvement in overhead sports were thought to have been minimized. Second, the measurement position was a limitation. Initially, the plan was to take measurements of both the Thiel cadavers and the human participants in the seated position. However, because it was not possible to fix the upper limb in the cadavers, measurements were performed in the supine position. Although the measurement positions were different, we believe that the effect was small because the JS is determined by the positional relationship between the upper arm and forearm. Third, it has been reported that the mechanical properties of Thiel cadavers are different to those of living humans, depending on the part measured. 7 Therefore, it will be necessary to compare various parameters in different joints between Thiel cadavers and living humans.
Conclusion
The results of this study indicate that Thiel cadavers show JS changes similar to those of humans when elbow valgus stress is applied. Results also indicate that the third and fourth digits and the second and fifth digits of the FDS both contribute to elbow valgus stability, and that there may be no difference in the amount of their respective contributions.
Footnotes
Acknowledgment
The authors acknowledge and thank those anonymous individuals who generously donated their bodies so that this study could be performed. They also thank technical staff members Kenichi Soma and Kenjiro Ito for helping with cadaveric management.
Final revision submitted February 12, 2021; accepted February 28, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: this study was supported by the Japan Society for the Promotion of Science (KAKENHI grant No. JP19K11358) and a Grant-in-Aid program from Niigata University of Health and Welfare. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Niigata University of Health and Welfare (study No. 18430).