
Abstract
Background:
There is a lack of consensus to guide patient return to sport (RTS) after elbow ulnar collateral ligament surgery (eUCLS).
Purpose:
To describe the reported RTS criteria after eUCLS in the athletic population.
Study Design:
Scoping review; Level of evidence, 4.
Methods:
This scoping review was performed by adhering to the PRISMA-ScR (Preferred Reporting Items for Systematic Reviews and Meta-Analyses–Scoping Review) guidelines. We searched 5 electronic databases (MEDLINE, Scopus, SPORTDiscus, Embase, Google Scholar Advanced) and the gray literature for English-language studies that reported at least 1 RTS criterion in athletes after eUCLS. Data were extracted and summarized as frequencies or arithmetic mean and standard deviation.
Results:
Included were 14 studies and 1335 athletes with a mean age of 21.4 ± 1.1 years. Time from surgery (range, 6-16 months) was the most common RTS criterion used, and it was reported by all 14 of the included articles. RTS criteria reported less often were pain (3/14; 21%), successful completion of a throwing program (3/14; 21%), muscle strength of the forearm muscles (1/14; 7%), and “normal” range of motion and muscle strength of the elbow and shoulder joints on the operated upper extremity (1/14; 7%). All studies used 1 to 5 of the above RTS criteria.
Conclusion:
Only 14 studies reported 1 or more RTS criteria after eUCLS in athletes, and time was the most common RTS criterion used. Our results highlight the need for a coordinated effort among surgeons, physical therapists, and athletic trainers in order to establish evidence-based RTS criteria after eUCLS in athletes so athletes can safely to sport and prolong their athletic careers.
The elbow ulnar collateral ligament (eUCL) is the primary restraint to valgus force of the elbow joint. Injuries to the eUCL most commonly result from recurring strain of the ligament during repetitive throwing. 8 These injuries are among the most commonly diagnosed in overhead throwing athletes, and surgical management is on the rise as a result. 18,22 Return to sport (RTS) after eUCL surgery (eUCLS) is extremely important both to athletes and to the organizations for which they play. The athletes who undergo surgical intervention often play at a high level and are extremely motivated to advance their recovery. RTS criteria to expedite the process of returning to play in an evidence-based fashion are a crucial element of the rehabilitation timeline.
Although multiple studies have evaluated the quality of return to play in athletes after surgical intervention, those studies have focused on postoperative statistics and qualitative measures related to the performance of the athlete rather than clarifying specific criteria for the athlete to return to full participation. 19,25 The outcomes of eUCLS and repair are excellent in many studies across multiple techniques. 10,16,20,24 The literature provides a paucity of data regarding actual RTS criteria despite successful reports on postoperative rehabilitation. 31
The primary goal of this scoping review was to describe the reported RTS criteria after both reconstructive and repair procedures for the management of eUCL injuries. Secondarily, we aimed to review those criteria in a succinct manner to determine whether standardization of the criteria was necessary and to identify areas of future research.
Methods
A preliminary search revealed significant heterogeneity among the studies reporting ≥1 RTS criteria after eUCLS in athletes; therefore, a scoping review was preferred over a systematic review. We adhered to the PRISMA-ScR (Preferred Reporting Items for Systematic Reviews and Meta-Analyses–Scoping Review) guidelines (http://www.prisma-statement.org/Extensions/ScopingReviews).
Study Identification and Criteria
We searched 5 electronic databases (MEDLINE, Scopus, SPORTDiscus, Embase, Google Scholar Advanced) and the gray literature, from inception to August 2020, for clinical studies reporting at least 1 RTS criterion after eUCLS in athletes. The following search terms were used in multiple combinations to retrieve potentially eligible articles from each database: elbow, athletes, instability, ulnar collateral ligament, medial collateral ligament, repair, reconstruction, Tommy John, surgery, surgical, therapy, treatment, management, outcomes, results, return to sport, return to sport rate, sport, sports, rehabilitation, physical therapy, criteria, criterion, milestone, milestones.
The database searches were performed in consultation with a librarian. Regarding the gray literature search, the advanced search function on Google was used to look for relevant articles. Finally, we searched the reference lists of the most relevant identified studies, including original research articles but also simple, scoping, or systematic review articles. The search was restricted to peer-reviewed articles published in the English language, without a limitation in the year of publication.
Study Criteria and Definitions
Inclusion in this review was based on the following 5 criteria:
Study design: Included were (1) prospective or retrospective studies that included a population of ≥6 athletes (all ages and levels of competition) who underwent eUCLS and that reported 1 or more criteria that were used to clear the athletes for RTS and (2) articles published in the English language in peer-reviewed journals. Exclusion criteria were as follows: (1) studies reporting the rate of RTS after eUCLS in athletes without mentioning at least 1 RTS criterion; (2) studies reporting the criteria to return to occupational activities after eUCLS in patients who were not classified as athletes; (3) studies not reported in the English language; (4) non–peer reviewed articles; and (5) case studies and case series with a sample size of <6.
Participants: Studies that described any participant as an “athlete,” regardless of age or level of competition (recreational, high school, collegiate, professional). Studies including a mixed patient population (athletes and nonathletes) were excluded if the results in the athletic subgroup were not clearly stated (ie, were not reported separately from the nonathletes). Studies that did not describe any participants as athletes were excluded.
Procedures: Studies in which all athletes underwent eUCLS (any type of eUCL repair or reconstruction surgery) with or without concomitant procedures. If additional procedures were performed at the time of eUCLS, studies were excluded if eUCLS was not reported as the primary surgical procedure. Studies including patients who had surgery for acute and/or chronic injuries to the UCL were considered eligible.
RTS rate: Studies that reported the percentage of athletes or elbows that returned to sport (regardless of the level of competition), based on the definition provided by each of the included studies.
Outcomes: Studies that reported at least 1 RTS criterion.
Study Selection Process
Potentially eligible articles from all databases were collected in EndNote X9.1 software (Clarivate Analytics). Relevant titles and abstracts were evaluated against the eligibility criteria by 2 independent reviewers (R.G., N.F.). When disagreement occurred, the study proceeded to full-text review. Full-text review was completed by 2 independent raters (I.K.B., R.G.). Where consensus was not reached, the senior author (F.A.P.) was consulted.
Data Extraction
Prearranged tables to record extracted data were developed on Excel (Microsoft). Data recorded for each of the included studies included the authors, year of publication, number of elbows or patients analyzed (who had follow-up), number of elbows or patients who returned to sport, patient age, type of procedure performed, RTS rate, mean RTS time (in months), and reported RTS criteria. The data elements were discussed between 2 reviewers (R.G., I.K.B.), and any disagreements were resolved by consulting a third reviewer (F.A.P.).
Results
Study Identification
The study flowchart (Figure 1) details the results from the study search and screening process. A total of 14 studies ∥ (Table 1) were eligible for inclusion in this scoping review. The majority of studies (11/14) included athletes who underwent eUCL reconstruction, 2 studies 2,11 (2/14; 14%) included a mixed population of athletes who underwent UCL reconstruction or UCL repair, and 1 study 29 (1/14; 7%) included athletes who underwent UCL repair (Table 1).

Study flowchart. RTS, return to sport.
Characteristics and RTS Criteria of the Included Studies a

a NR, not reported; ROM, range of motion; RTS, return to sport; UCL, ulnar collateral ligament.
Study Population
This review included 1335 athletes with a mean age of 21.4 ± 1.1 years (range, 17.2-32.7 years). The sport the athletes played and the sex of the athletes were not reported in many of the included articles. Of the athletes, 1253 (94%) underwent UCL reconstruction and 82 (6%) underwent UCL repair. The RTS rate was 85% (1134/1335 athletes). The mean RTS time was reported in 12 of 14 studies (86%); the mean RTS time for all of the studies combined was 10.7 ± 2.6 months (range, 6-15 months).
RTS Criteria
The number of RTS criteria used in each of the included articles ranged from 1 to 5 (Table 1). Time from surgery (range, 6-16 months) was the most common RTS criterion used, and it was reported by all 14 of the included studies (100%), followed by absence of pain (3/14 studies; 21%), 2,11,28 successful completion of a throwing program (3/14; 21%), 1,4,11 normal range of motion (ROM) and muscle strength in the shoulder and elbow of the operated upper extremity (1/14; 7%), 11 and normal strength of the forearm muscles (1/14; 7%). 11 Figure 2 presents the frequency of each RTS criterion reported among the included studies. The 5 criteria are further described below.
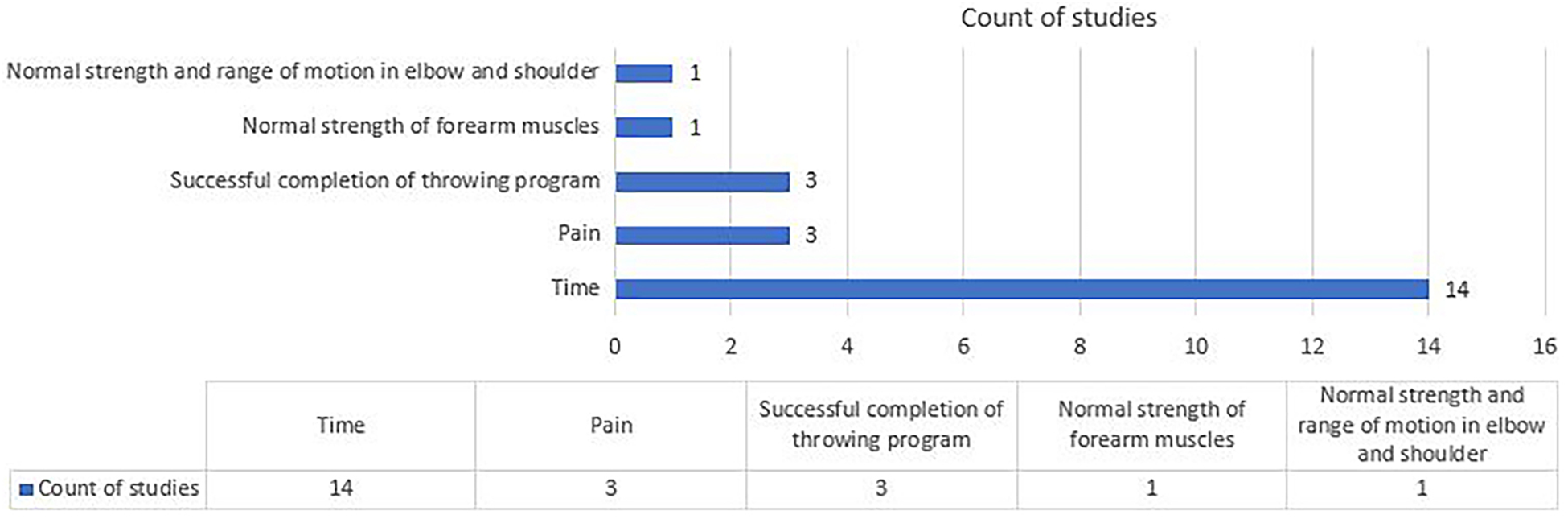
Distribution of the reported return-to-sport criteria after surgery of the elbow ulnar collateral ligament among the included studies.
(1) Time
Time was the most commonly reported RTS criterion (14/14 studies; 100%) in athletes undergoing eUCLS. Time alone was used as the RTS criterion in 9 of the 14 studies (64%) 5,7,12,17,21,26,27,29,30 (Table 1). The time interval used as the RTS criterion among the included studies was highly variable (Figure 3). A total of 5 studies (5/14; 76%) 4,12,17,28,29 used a time range within which the athletes were allowed to return after eUCLS, whereas 9 studies (9/14; 64%) reported the minimum amount of time required before the athletes returned to their sport (Table 1). In the last category of studies, 12 months was the most commonly reported value (used in 4 studies). 1,5,11,30 We observed shorter RTS time in articles reporting the outcomes of UCL repair compared with UCL reconstruction, but in general the indications were often different for the 2 procedures.

Reported time required between surgery and return to sport (RTS), which was used as an RTS criterion in athletes undergoing surgery to the elbow ulnar collateral ligament.
(2) Pain
Complete absence of pain at rest and during sport activity was used as an RTS criterion after eUCLS in 3 studies (21%). 2,11,28
(3) Successful Completion of a Throwing Program
A total of 3 of the included articles reported successful completion of a throwing program as an RTS criterion after eUCLS. One of these studies 11 defined this criterion as “normal throwing balance, rhythm, and coordination,” but no definition was provided in the other 2 articles. 1,4
(4) Normal Strength of Forearm Muscles
Normal strength of the forearm muscles was reported as a criterion by 1 study, without further details.
(5) Normal Strength and ROM of the Operated Elbow and Ipsilateral Shoulder Joints
This was reported as an RTS criterion by 1 study, without detailed description of the muscle strength or ROM cutoff values and without comparison with the contralateral side or preinjury values.
Discussion
Time from surgery was the most commonly reported RTS criterion after eUCLS in athletes, and it was used in all of the included articles (14/14 studies; 100%). There was no consensus among the various studies as to how much time was adequate for rehabilitation before returning to play, with time frames ranging from 4 to 16 months; a minimum of 12 months between surgery and RTS was used as the criterion in 4 studies. Less commonly used RTS criteria after eUCLS included pain (3/14 studies; 21%), completion of a graduated throwing program (3/14 studies; 21%), normal strength of the forearm muscles (1/14 studies; 7%), and normal ROM and strength of the elbow and shoulder (1/14 studies; 7%).
Although various rehabilitation protocols were described in some of the technical and outcome studies that were reviewed for this study, actual RTS criteria remain critically underreported. 13,15 Time was the most commonly reported criterion, possibly due to the surgeons’ estimated time for adequate tissue healing based on their personal experience; specifically, all of the included studies reported a minimum time and/or a range of time elapsed between surgery and RTS. Although time was the most commonly reported criterion, it seemed that other factors played a role in the decision to return the athletes to sport, and these factors should be reported in greater detail in future studies. This could subsequently help to classify the different RTS criteria based on their clinical significance and the “weight” that each holds in making RTS decisions.
In a previous scoping review that examined RTS criteria after anterior cruciate ligament reconstruction (ACLR), time was the predominant criterion for RTS, used in 85% (178/ 209) of the included studies. 6 Wilk et al 31 described a detailed, evidence-based postoperative rehabilitation program for the surgically treated UCL. Interestingly, 3 of the 14 articles included in the current scoping review originated from the same institution. 2,7,28 These articles highlighted specific milestones in order to progress through phases 1 to 4 of the postoperative rehabilitation and return to full sport, but whether these are being widely adopted is not clear in the literature. 31,32 Some of these milestones include progression to phase 2 when the patient exhibits full elbow ROM, minimal pain, and good (4/5) muscle strength testing on the operated extremity and progression to phase 3 when the patient exhibits full, nonpainful ROM, absence of pain or tenderness, and strength that is 70% of the contralateral extremity. 31 These protocols are not being reported along with the technique and outcomes, regardless of whether these assumed criteria are based on the literature, expert opinion, or surgeon preference.
Ciccotti et al 9 performed a systematic review looking specifically at RTS criteria for individuals who had previously undergone anterior shoulder stabilization surgery, and the investigators reported time as the most prevalent (89%) criterion used. This finding was followed by much lower percentages of studies reporting on strength (18.9%), ROM (13.8%), pain, stability, proprioception, and postoperative radiographs. Those studies that used criteria based on strength and ROM did not describe specific objective measurements for those outcomes but generally used “equal to” or “a percentage of” the contralateral side. Similarly, no study in our review gave specific ROM or strength measurement guidelines for returning to play. In addition, none of the included studies defined “normal” ROM or strength in relation to the preinjury measurements on the operated upper extremity or the measurements on the contralateral upper extremity.
Interestingly, only 2 studies 1,4 reported the successful completion of a throwing program as an RTS criterion. One possible explanation of this phenomenon could be that the included athletes in each study followed different rehabilitation programs and the completion of a throwing program was based on the preference of the physical therapist. In addition, some of the included studies may have used a throwing program as an RTS criterion in their protocol but did not report this in the published article. The lack of detailed description of the RTS criteria was a limitation in all of the included articles. Therefore, future surgical case series reporting the outcomes of elbow stabilization surgery in athletes should provide the RTS protocol in detail in order to truly validate the effectiveness of the performed procedure and to establish the use of specific RTS criteria.
Even though RTS criteria are difficult to assess in the upper extremity based on the current literature, the RTS criteria for anterior ACLR have been well described. 6 There has been a shift in the literature from longitudinal time-based RTS criteria to specific measurable check points for the individual to attain before clearance for progressive return to full activity. 3,14 In a recent scoping review looking at the RTS criteria after ACLR, the most common criterion reported was time, which was again consistent with the results of the current review. 6 However, those authors found a much higher percentage of studies reporting muscle strength as an RTS criterion (41% compared with only 14% in our study).
In a scoping review of ACLR by Burgi et al, 6 40% of the studies that included strength testing specifically reported isokinetic evaluations of the operative extremity using the limb symmetry index, with a minimum of 85% needed for RTS clearance. This is in contrast to the results of the current review, where we found that objective data on upper extremity strength were not reported. Similar to the current review, Burgi et al found that there is no single battery of tests reported in the literature regarding return to play after ACLR. A far higher number of objective measures are reported in the ACLR literature versus the literature on UCL surgery with regard to RTS criteria; however, not all of these objective measures for ACLR have been shown to correlate with RTS. 6
The purpose of this scoping review was to evaluate the reporting of RTS criteria after UCL repair or reconstruction in the athlete population. Very few studies reported specific RTS criteria and even fewer noted any functional testing. This review highlights the need for evidence-based and validated RTS criteria, specifically for athletes whose careers depend on their ability to return to throwing sports. Even though all 14 included articles reported RTS criteria, none of them provided information regarding outcome differences between different criteria or a validated time period of rehabilitation before athletes can return to play. A standardized RTS program for the throwing athlete after UCL surgery could accelerate recovery and potentially improve overall safe return to play at the preinjury level of physical activity.
This study was limited by several factors. Although scoping reviews are comprehensive, there is always a risk of missing studies. Our search focused on surgical outcome studies that reported specific RTS criteria in athletes undergoing eUCLS. Although numerous papers have described various postoperative rehabilitation protocols and milestones for RTS after eUCLS, data related to their implementation in clinical practice are lacking. 23,31,32 Thus, we excluded articles failing to report data in this category, which resulted in a small number of studies being analyzed in the current review. Although our results highlight the lack of RTS criteria after eUCLS in athletes, we were unable to determine whether these criteria were not used in practice or whether they were simply underreported in surgical case series. Last, although some of the included studies originated from the same institution, there were differences in the reported surgical techniques and/or RTS criteria. 2,5,7,12,21,28 Differences in UCL reconstruction techniques were not assessed among the different studies that reported different RTS criteria.
Future research should focus on establishing a connection between the existing evidence on postoperative UCL rehabilitation protocols and RTS criteria and the use of this evidence in clinical practice and surgical outcome research in orthopaedics. There is a need to validate specific RTS criteria after eUCLS in athletes so that clinicians can return the athletes to sport safely while minimizing their absence from sport participation. The last is particularly important in high-level athletes in order to prevent the socioeconomic effects associated with eUCL injuries that require surgical intervention.
Conclusion
Only 14 studies reported 1 or more RTS criteria after eUCLS in athletes, and time was the most common RTS criterion used. Our results highlight the need for a coordinated effort among surgeons, physical therapists, and athletic trainers to establish evidence-based RTS criteria after eUCLS in athletes to promote a safe and effective return to sport.
Footnotes
Notes
Final revision submitted February 1, 2021; accepted February 24, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: A.E.W. has received educational support from Arthrex, nonconsulting fees from Arthrex, and hospitality payments from Stryker. S.C.G. has received educational support from Arthrex, consulting fees from Zimmer Biomet, and nonconsulting fees from Arthrex. F.A.P. has received consulting fees from Zimmer Biomet, Flexion Therapeutics, Exactech, and Stryker; honoraria from Fidia Pharma and Musculoskeletal Transplant Foundation; and education payments from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.