
Abstract
Background:
No previous systematic review to our knowledge has examined the reasons that athletes fail to return to sport (RTS) after ulnar collateral ligament (UCL) surgery.
Purpose:
To report the rate of failure to RTS after UCL surgery and identify reasons that preclude an athlete’s ability to successfully RTS.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
This study was conducted in accordance with PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. We searched the PubMed, Scopus, and SPORTDiscus databases for studies on athletes who underwent either UCL reconstruction or repair that reported RTS rates and identified reasons for failure to RTS. Data were collected on the number of athletes included, average age, sport played, operative technique, average follow-up, rate of failure to RTS, and reasons for failure to return. A random-effects model was used to conduct the meta-analysis.
Results:
Included were 26 studies reporting on 1019 athletes. Primary or revision UCL reconstruction was performed in 913 patients (89.6%), while the remaining 106 patients (10.4%) underwent UCL repair. The pooled rate of failure to RTS after UCL reconstruction or repair was calculated to be 11.4% (95% CI, 8.4-14.7). A significantly higher estimated proportion of athletes failed to return because of elbow-related reasons compared with non–elbow-related reasons (55.3% vs 40.6%; P = .0352). Persistent pain (29/103; 28.2%) was the most common reason for failure to return, followed by elbow limitations and other unspecified elbow problems (19/103; 18.4%). There was moderate evidence for publication bias and study heterogeneity across the included studies.
Conclusion:
This meta-analysis estimated the rate of failure to RTS after UCL surgery as 11.4%, with the majority of athletes unable to return because of elbow pain. Future studies reporting outcomes and providing details as to why athletes are unable to RTS can better inform sport surgeons on factors precluding RTS and can guide clinical practice to better help athletes achieve their postoperative goals.
The elbow ulnar collateral ligament (UCL), also referred to as the medial UCL, is composed of 3 separate connective tissue bundles and functions as a stabilizer of the elbow joint. 19,51 Repetitive valgus stress, especially among overhead athletes during throwing maneuvers, can result in microtrauma and eventual failure of the ligament. 5,20,27,37 First described in javelin throwers by Waris 54 in 1946, UCL injuries have since been reported in a variety of athletes, including wrestlers, football quarterbacks, tennis players, gymnasts, and, most prominently, baseball players. 7,28,38
UCL reconstruction was first introduced by Jobe et al 27 in 1986 as a solution to a previously career-ending injury. 54 This procedure has been since modified and widely integrated in modern orthopaedic practice. The prevalence of UCL reconstruction in professional baseball players has increased from 10% in the 2012-2013 season to 13% in the 2018 season. 10,32 This trend has also been reported in nonprofessional athletes. The volume of UCL reconstructions in New York State increased 193% over a 9-year period (2002-2011), and both the incidence and the total number of procedures in 15- to 19-year-olds significantly increased between the years 2007 and 2011. 25 Projections through 2025 estimate that the incidence of UCL reconstructions in younger cohorts will continue to increase. 33
The success of UCL reconstruction is often judged by the rate at which athletes can successfully return to sport (RTS) postoperatively. In the first reported cohort of patients undergoing UCL reconstruction by Jobe et al, 27 60.5% of athletes were able to resume competitive play after injury. With modification of the original surgical technique and implementation of comprehensive postoperative rehabilitation programs, the rate to RTS is now reported to be between 79% and 96%. 8,11,13,15,28,56,57 More recently, elbow UCL repair with internal bracing has emerged as a viable alternative to reconstruction with demonstrated RTS rates as high as 92%. 17 Several systematic reviews and meta-analyses have reported the incidence of RTS after UCL injury. Erickson et al 18 reported on 20 studies with an 86.2% pooled RTS rate. Thomas et al 50 reported that among baseball players, return-to-play rates after UCL reconstruction varied by position. They found that catchers return to play less frequently than pitchers, infielders, or outfielders, and that pitching workloads decrease after UCL reconstruction. 50 However, to the best of our knowledge, no previous systematic review has characterized the reasons for why athletes fail to RTS after UCL reconstruction.
The purpose of this meta-analysis was to report the rate of athletes who fail to RTS after either UCL reconstruction or repair and to determine the reported reasons for failure to return. We hypothesized that a small percentage of athletes would fail to RTS after elbow UCL reconstruction or repair and that the number of athletes who do not return for elbow-related reasons would be similar to those who do not return for non–elbow-related reasons.
Methods
Search Strategy
This meta-analysis was performed using the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement as a guide. 52 A comprehensive search was conducted from the United States National Library of Medicine PubMed/MEDLINE, Scopus, and SPORTDiscus databases using multiple combinations of the following search terms: “athletes,” “elbow,” “ulnar collateral ligament,” “UCL,” “eUCL,” “reconstruction,” “repair,” “return to sport,” “outcome,” “outcomes,” “sport,” and “failure to return to sport.” The search was conducted from database inception until June 2021.
Study Selection
All articles were screened by title and abstract by 2 authors (I.K.B., A.F.) independently according to our prespecified inclusion and exclusion criteria outlined in Table 1. Discrepancies were resolved by a third author (F.A.P.). The included articles were then screened by full-text review by 2 authors (A.H., A.F.), with discrepancies resolved by the same third author. We included studies only where the rate of failure to RTS was clearly discernible, and additional commentary or data were given as to the specific reasons for why athletes failed to RTS after UCL surgery. RTS was defined as return to any intensity of play (same level or reduced), and failure to RTS was defined as athletes who definitively were unable to play at any level. Studies involving exclusively nonathletes were excluded. Additionally, we only included studies in which the article was available in the English language and those that had undergone peer review. We identified 26 studies that reported both RTS rates and reasons for failure to return after elbow UCL reconstruction or repair with the PRISMA flowchart illustrated in Figure 1. Duplicate studies were identified and removed before the screening process.
Study Inclusion and Exclusion Criteria a
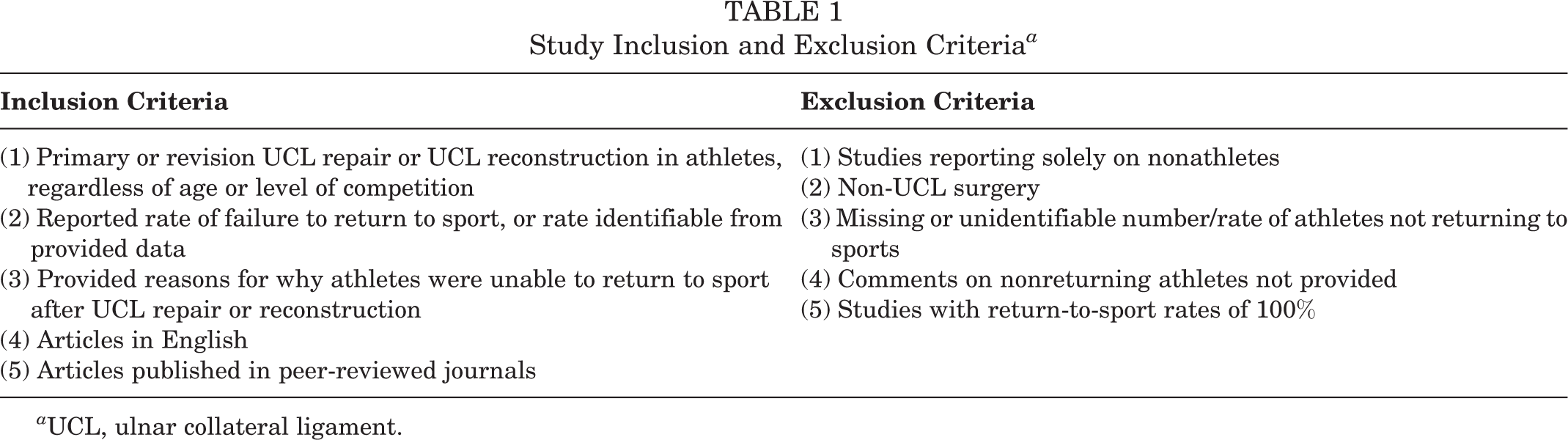
a UCL, ulnar collateral ligament.
Studies that met all the inclusion criteria were considered for inclusion in the meta-analysis; studies that met any of the exclusion criteria were excluded from the meta-analysis.

PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flowchart of study inclusion.
Data Aggregation and Outcomes
Data were aggregated using Microsoft Excel 2017 (Microsoft Corp) to collect the following variables from each of the included studies: age of athletes, sex, type of sport, procedure type, mean follow-up time, number of athletes who failed to RTS, reasons for failure to RTS, number or rate of athletes who did not return because of an issue with the elbow, and number or rate of athletes who did not return for reasons unrelated to the elbow. Weighted means were calculated for age of athletes and postoperative follow-up time across all studies reporting on these variables.
Quality Assessment and Statistical Analysis
Each study included was evaluated using the Methodological Index for Non-Randomized Studies (MINORS) criteria to ensure adequate study quality before incorporation in the final quantitative analysis, with a maximum possible score of 24 for comparative studies and 16 for noncomparative studies. 48 The level of evidence was determined based on criteria established by the American Academy of Orthopaedic Surgeons. 47 The degree of study heterogeneity was reported using the I 2 statistic. A random-effects model was implemented for this study, regardless of the degree of heterogeneity observed between individual studies included in the analysis. A meta-analysis of pooled proportions with 95% CIs was conducted, and publication bias was assessed through generation of a funnel plot. All statistical analysis was performed using MedCalc software (Version 19.1.3; MedCalc Software Ltd).
Results
Study Population and Surgical Technique
Overall, 26 studies with 1019 athletes who underwent elbow UCL reconstruction or repair were included in the final analysis. ‡ Of the 1019 athletes, 103 (10.1%) failed to RTS postoperatively. The mean patient age was calculated to be 21.38 ± 2.91 years, and the weighted mean follow-up time was calculated to be 41.69 ± 17.04 months. Only 6 studies 4,8,28,29,38,44 included female athletes, resulting in 57 female athletes (5.6%) and 711 male athletes (69.8%). The sex was not specified in the remaining 251 athletes. Baseball was the most frequently cited sport played by athletes (895/1019; 87.8%) undergoing elbow UCL repair or reconstruction. Of the 1019 patients reported in this meta-analysis, only 107 (10.5%) underwent elbow UCL repair, while 913 (89.6%) underwent either primary or revision UCL reconstruction.
Literature Quality Assessment
Moderate data asymmetry and publication bias were revealed through interpretation of the generated funnel plot (Figure 2). A moderate degree of study heterogeneity was observed (I 2 = 057.97%; 95% CI, 35.07-72.70; P = .0001). The majority of studies were of level 4 evidence (23/26, 88.5%), with 2 (7.7%) of level 3 evidence 43,49 and 1 (3.8%) of level 2 evidence. 16 The average MINORS score across all studies was 11.9 ± 1.4, indicating a fair quality of evidence.

Funnel plot revealing moderate asymmetry and potential evidence of publication bias.
Failure to RTS
A total of 103 athletes failed to RTS after UCL reconstruction or repair. A pooled failure to RTS rate was calculated to be 11.4% (95% CI, 8.4-14.7) (Figure 3). When comparing reported reasons for failure to return, a significantly greater percentage of athletes reported reasons related to elbow compared with non–elbow-related reasons (55.3% vs 40.6%; P = .0352). The most commonly cited elbow-related reason was persistent pain, which was reported in 29 patients (29/57; 50.9%), followed by elbow problems and limitations in 19 athletes (19/57; 33.3%). Reinjury to the arm or elbow was the cause of failure to return in 6 patients (10.5%). Non–elbow-related reasons accounted for 42 patients failing to RTS, most commonly because of graduation or loss of interest in the sport (17/42; 40.5%), followed by career change or retirement (9/42; 21.4%). Reasons for failure to return were completely unspecified in 4 athletes (3.9%). An exhaustive list of all cited reasons for failure to RTS after elbow UCL surgery is given in Figure 4.

Estimated rate of failure to return to sport among athletes undergoing ulnar collateral ligament surgery. The individual rate of failure to return to sport is represented by the proportion value. All studies were weighted according to a random-effects model, with the size of each square correlating with the weight given to that study in the analysis.

Reported reasons associated with failure to return to sport after elbow ulnar collateral ligament reconstruction or repair.
Discussion
In the 26 studies reviewed, overall failure to RTS was estimated to be 11.4%. The specific reasons for failure to RTS could be delineated by elbow-related reasons and non–elbow-related reasons, with a significantly higher percentage of athletes citing elbow-related reasons as the cause of failure to RTS after UCL elbow repair or reconstruction (55.3% vs 40.6%, P = .0325). The most common among elbow-related reasons was persistent pain (29/57; 50.9%) despite surgical repair/reconstruction, followed by nonspecific elbow limitations (19/57; 33.3%), with reinjury after reconstruction constituting a minority of reasons for failure to RTS (6/57; 10.5%). Non–elbow-related reasons, conversely, were most commonly because of graduation or loss of interest in the sport played (17/42; 40.5%).
Several reviews and meta-analyses exist in the literature that report on the incidence of RTS after UCL injury. 9,12,22,23,42,50 The available published data, however, often fail to specifically delineate the reasons for inability to RTS after UCL injury requiring reconstruction. This meta-analysis thus serves to supplement the literature with respect to why athletes undergoing elbow UCL reconstruction ultimately fail to return to their prior level of play.
Not surprisingly, the overwhelming majority of reported UCL injuries in the literature are in overhead-throwing athletes, with more than 92% of injuries in our study occurring in baseball players. § Cited studies demonstrate similar demographic makeups, including 95% baseball players, with an 89% majority representing pitchers. 7,39 This homogeneity would seem to make the analysis of RTS simpler; however, such analysis requires considering factors that include the use of established rehabilitation protocols postoperatively, the level of return to play (recreation, Minor League, Major League, etc), and pre- versus postinjury level of performance. The current literature is unfortunately quite heterogeneous in this regard, with few studies reporting on all these factors jointly. Regardless, the consensus in at least 2 large meta-analyses is that roughly 82% to 83% of postsurgical outcomes are excellent, with at least 86% of patients returning to some level of play. 18,53 This figure for RTS parallels that of the large single series study by Cain et al 7 that reports an 83% RTS at the same level or higher and corroborates the 88.6% rate of RTS found in our meta-analysis. Thus, when considering failure to RTS, part of the discrepancy in reported reasoning can likely be attributed to the fact that the majority of patients not only tolerate the procedure well but also are often satisfied with the results and overwhelmingly return to some level of play. 7,39
In our study, 55.3% of patients failed to RTS because of elbow-related reasons, with most of them citing persistent pain as the primary reason. A recent meta-analysis observed reported reasons for failure to RTS in athletes undergoing hip arthroscopy for femoroacetabular impingement syndrome (FAIS). 55 Similar to our findings, this study reported that a significantly greater percentage of athletes failed to RTS after hip arthroscopy because of hip-related reasons than non–hip-related reasons. Additionally, the authors reported that the most common injury-related reason for failure to return was persistent pain. 55 Although the nature and rehabilitation process of elbow UCL and FAIS injuries differ, injury-related postoperative problems were the most commonly cited reasons for failure to RTS. 55 Regarding postoperative rehabilitation after UCL injuries, available studies demonstrate significant diversity among rehabilitation protocols without the existence of a single, validated postoperative pathway for optimal return to play. 7,18,21,30,34,53 The average time to RTS in these studies varies from as little as 11.6 months to as many as 20.1 months. Given that there is no defined minimal amount of time required for rehabilitation before RTS, it is difficult to know whether persistent pain and elbow limitations postoperatively are because of the nature of the surgery or the duration and quality of the postoperative rehabilitation process. Further studies would be necessary to validate rehabilitation protocols and optimize time out from sport to understand how these factors contribute to athletes ultimately failing to return to play.
With regard to decline in postoperative level of performance when compared with preinjury level of play, the existing literature does not appear to support a decline in performance as a cause for failure to RTS, with the pitchers specifically demonstrating lower earned run averages and hits per inning pitched than before surgery. 18,34 Although additional studies have found a statistically significant reduction in pitch velocity postoperatively, on average 2.9 mph, the decline in velocity does not appear to be more significant than age-matched, uninjured controls and would not appear to contribute to a player failing to return to play. 26,31,34
Interestingly, non–elbow-related reasons for failure to RTS appear to make up slightly less than half of all reasons for sport retirement in our study. In the study by Osbahr et al, 39 after 10 years of follow-up, more than 86% of athletes who retired from play cited reasons other than elbow pain or persistent elbow problems for their ultimate decision to give up the game. Although our study cites psychosocial reasons such as graduation or loss of interest as the primary non–elbow-related reasons for failure to RTS, Osbahr et al reported subsequent shoulder problems as the predominant reason for retirement. They also noted a career longevity of only 3.6 years postoperatively, a figure corroborated by Erickson et al, 18 who cited a 3.9-year average career length in either major or minor leaguers after UCL reconstruction. Although there is most certainly unaccounted-for variability in this reasoning process based on athlete level among high schoolers, collegiate athletes, and minor and major leaguers, these studies demonstrate that anywhere from 40% to 80% of failure to return to play likely has very little to do with the direct postoperative effects of UCL reconstruction on the elbow.
Limitations
This meta-analysis has a few limitations worth consideration. While every effort was made to develop a comprehensive search strategy, there is always a chance that relevant studies meeting the inclusion criteria may have been missed in the search and screening process. The current body of literature on this topic consists primarily of retrospective case series, with most of the studies included in this analysis being of level 3 and 4 evidence, which is not ideal. Additionally, our analysis combined elbow UCL repair, primary reconstruction, and revision, potentially biasing our results, as patients with complications necessitating revision reconstruction expected to have worse outcomes in regard to RTS and were potentially more likely to have reasons for failure to RTS related to the elbow than those undergoing either primary reconstruction or repair. Additionally, it is difficult to ascertain the degree to which our results were skewed because of adherence to postoperative rehabilitation protocols, perceived pain related to postoperative decline in level of performance, or additional psychosocial factors. Still, these results illustrate that long-term pain control is an area of clinical care that can be optimized, especially among athletes looking to return to a preinjury level of play. Finally, heterogeneity between included studies and the publication bias may have affected our results.
Conclusion
This meta-analysis estimated the rate of failure to RTS after elbow UCL surgery as 11.4%, with the majority of athletes unable to return because of reasons related to the elbow, with persistent pain being the most common reason cited. Future studies reporting outcomes and providing details as to why athletes are unable to RTS can better inform sport surgeons on factors precluding RTS and can guide clinical practice to better help athletes achieve their postoperative goals.
Footnotes
Notes
Final revision submitted May 24, 2022; accepted August 2, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: A.E.W. has received nonconsulting fees from Arthrex and hospitality payments from Stryker. F.A.P. has received consulting fees from Exactech, Flexion Therapeutics, Medical Device Business Services, and Stryker; hospitality payments from Arthrex; and honoraria from Musculoskeletal Transplant Foundation. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.