
Abstract
Background:
Medial ulnar collateral ligament (UCL) injuries are functionally debilitating for throwing and overhead athletes. While autograft remains the most common graft for UCL reconstruction (UCLR), allograft offers advantages, including reduced donor-site morbidity and reduced surgical time. However, clinical outcome data on allograft use, particularly in overhead athletes, remain limited.
Hypothesis:
It was hypothesized that overhead athletes undergoing UCLR with hamstring allograft would demonstrate high return to sport (RTS) rates, favorable functional and patient-reported outcomes, and low complication rates.
Study Design:
Case series; Level of evidence, 4.
Methods:
This retrospective case series evaluated 25 overhead athletes who underwent UCLR using hamstring allograft between 2017 and 2022 at a single, high-volume orthopaedic practice. Patient-reported outcome measures were collected at baseline and at a minimum 1-year follow-up, including the 12-Item Short Form Health Survey, Veterans RAND 12-Item Health Survey, Patient-Reported Outcomes Measurement Information System Upper Extremity (PROMIS UE), Quick Disabilities of the Arm, Shoulder and Hand (QuickDASH) score, Mayo Elbow Performance Score (MEPS), and visual analog scale (VAS) for pain. Functional outcomes (grip strength and range of motion [ROM]), RTS, and complications were assessed at a minimum of 1-year follow-up.
Results:
The cohort's mean age was 21 years, and 80% were men. Overall, RTS (48% highschool, 48% collegiate, 4% professional)was achieved in 92% of patients, with 83% returning to their previous or higher level of sport. At final follow-up (mean, 13 ± 19 months), the mean postoperative PROMIS UE was 59.2, QuickDASH was 5.6, MEPS was 72.5, and VAS Pain was 4.7. ROM returned to preoperative levels or improved in all but one patient. Failure resulting in revision reconstruction occurred in 1 patient. Two patients underwent hardware removal, and 1 patient had continued subjective instability. No infections or graft rejections occurred.
Conclusion:
At 1-year follow-up, UCLR with hamstring allograft demonstrates high RTS rates and favorable functional and patient-reported outcomes in overhead athletes, with a low complication rate.
The medial ulnar collateral ligament (UCL) is the primary static stabilizer against valgus stress at the elbow, especially during activities that place high valgus loads on the elbow joint, such as those performed by throwing and overhead athletes.18,22 These types of activities introduce repetitive trauma that can cause microtears and weakening of the UCL, predisposing it to failure over time. 10 Failure of the UCL then limits the ability of throwing and overhead athletes to execute commonly performed motions in their respective sports. Thus, injuries to the UCL in throwing athletes can be devastating, providing a valuable opportunity to assess the outcomes of common treatment options for this type of injury.
Historically, the gold standard for treating UCL injuries in throwing and overhead athletes has been surgical reconstruction with a semitendinosus or palmaris longus autograft.5,15,25 Previous major league baseball data comparing palmaris longus and hamstring autografts demonstrated no significant difference in outcomes or subsequent injury rates after UCL reconstruction (UCLR). 11 However, the use of an allograft has also been reported. Proposed benefits of this graft option include less postoperative pain or paresthesia at the autograft harvest site, eliminating the need to harvest tissue from an uninjured extremity, and ensuring greater consistency in graft size and quality, particularly when patient anatomy does not provide a suitable autograft, as is commonly the case with the palmaris longus.23,25 Recent systematic review data have demonstrated favorable outcomes and return to sport (RTS) rates for overhead athletes undergoing UCLR with allograft. 23 However, only 5 studies were included in this review, with even fewer evaluating outcomes in overhead athletes. Specifically, the most recent study assessing outcomes after UCLR with an allograft in exclusively throwing and overhead athletes was published in 2013 and used various techniques. 24 Thus, there is a lack of updated and current literature on allograft utilization for UCLR for overhead and throwing athletes, with no recent available studies assessing patient-reported outcome measures (PROMs), clinical outcomes, and functional outcomes within the same sample population.
This study aimed to assess PROMs and clinical and functional outcomes in overhead athletes who underwent UCLR with an allograft. We hypothesized that the overhead athletes in this study would demonstrate a higher RTS rate than in their previous levels of competition, with low rates of adverse events postoperatively.
Methods
Study Design and Patient Selection
This study was a retrospective case series that received institutional review board (IRB) approval (Rush University Medical Center), with a corresponding waiver of consent due to its retrospective nature. A retrospective review of all patients who underwent UCLR with an allograft from 2017 to 2022 by 2 senior sports or hand-fellowship trained orthopaedic surgeons (N.N.V., M.S.C.) at a high-volume center. Indications for UCLR included complete or high-grade partial UCL tears with persistent medial elbow pain or valgus instability that failed at least 3 to 4 months of nonoperative management. All patients had magnetic resonance imaging (MRI) confirming UCL insufficiency or disruption, consistent with their clinical findings. In our practice, an allograft is selected for patients who wish to avoid donor-site morbidity, for those with inadequate or absent autograft options (eg, hypoplastic palmaris longus), or when minimizing graft-harvest morbidity is preferred. Allograft is also considered in athletes with previous lower-extremity injuries or when autograft harvest may interfere with sport-specific demands. Final graft choice is determined through shared decision-making after discussing the risks and benefits of autograft versus allograft with each patient. The inclusion criteria consisted of patients >18 years who underwent UCLR with hamstring allograft for underlying UCL insufficiency or disruption, with a minimum 1-year postoperative follow-up. All patients underwent anterior subcutaneous transposition of the ulnar nerve at surgery. Other concomitant procedures, such as excision of ulnar osteophytes and removal of loose bodies, were included. Indications for UCLR were based on symptom severity, symptom duration, hindrance of athletic activities, and failure of 3 to 4 months of nonoperative management with positive MRI findings.
Patients’ electronic medical records were retrospectively reviewed by 2 independent authors (L.D.M., J.O.E.) to collect descriptive data, preoperative diagnoses, and operative reports. Patient characteristics included age, sex, laterality of arm injury, level of sports played (high school, collegiate, amateur/professional), and position played (pitcher, position player) when applicable. The primary outcome was RTS, along with time to RTS and level of performance upon return. Secondary outcomes included grip strength measurements using a handheld dynamometer, and PROMs focused on activities of daily living—including the Short Form-12 (SF-12) and the Veterans Rand 12 Item Health Survey (VR-12). Other PROMs focusing on functional outcomes were collected at postoperative follow-up, including the Mayo Elbow Performance Score (MEPS), Patient-Reported Outcomes Measurement Information System Upper Extremity (PROMIS UE) score, Quick Disabilities of the Arm, Shoulder, and Hand (DASH) score, and visual analogue scale (VAS) pain score. Data on adverse events were also collected, including failure (as defined by the need for revision UCLR), nonrevision reoperation, and complications. PROMs and RTS surveys were distributed and stored using a secure electronic platform (Patient IQ).
Surgical Techniques
All surgical procedures were performed by the senior authors at a single institution (N.N.V., M.S.C.). A regional block was performed preoperatively as a routine. A standard medial approach to the elbow was performed. The medial antebrachial cutaneous nerve was identified and protected. The ulnar nerve was dissected and transposed anteriorly into a subcutaneous position in all cases to reduce the risk of postoperative ulnar neuropathy. The flexor-pronator mass was split or elevated to expose the UCL, which was incised in the midline to confirm valgus instability. Bone tunnels were created in the ulna and humerus using 5-mm drills at anatomic insertion sites. The semitendinosus allografts used for reconstructions were aseptically processed using a proprietary chemical cleansing protocol, non-irradiated specimens, and were stored frozen, sourced from a single certified tissue bank. Grafts were size-matched to each patient's native UCL, typically measuring 4.5 to 5 mm in diameter and 120 to 140 mm in length. A semitendinosus allograft was prepared with a running locked No. 2 FiberLoop suture (Arthrex) and passed through an ulnar bone tunnel using ligature passers. The graft was tensioned and docked proximally through 1 humeral tunnel with sutures tied over an EndoButto along the posteromedial humeral column (Smith & Nephew). The native ligament was repaired under the graft. The flexor-pronator origin and triceps fascia were closed, and the wound was closed in layers with a compressive dressing and internal splint.
Postoperative Rehabilitation
Postoperative care included initial immobilization in a posterior mold splint, followed by progression to a removable or hinged elbow brace for weeks 2 to 4. Physical therapy began after splint removal, focusing on the elbow range of motion (ROM) and grip strength. At 4 weeks, the brace was discontinued, and light strengthening exercises were initiated in the plane of the elbow. Throwing was reintroduced at 4 months via an interval program, progressing from 45 to 180 feet based on pain-free performance and proper mechanics. A mound program began after successful flat-ground throwing. Return to competition was permitted between 9 and 12 months, contingent on full strength recovery, absence of pain, and restoration of throwing mechanics.
Statistical Analysis
Descriptive analysis of continuous variables included means and standard deviations, while frequencies and percentages were used to report categorical variables. Chi-square tests were used to evaluate for differences among categorical variables. Significance was set at P < .05, a priori. Statistical comparisons were considered significant at P≤ .05. Statistical analyses were performed using RStudio software (Version 1.0.143; R Foundation for Statistical Computing).
Results
Patient Characteristics
A total of 25 overhead athletes were included in the final analysis. Patients were most commonly high school (48%) and collegiate (48%) athletes. The overall cohort consisted of 4 gymnasts/cheerleaders and 21 baseball players (n = 16 pitchers, n = 5 position players). All baseball players use their dominant arm. The mean age was 21 ± 6 years. Surgeries were performed between 2017 and 2022; however, many of the later cases had not yet reached longer-term follow-up at the time of chart review. In addition, several earlier cases were lost to follow-up after returning to sport. Consequently, the mean follow-up duration for the cohort was 13 ± 19 months (Table 1).
Patient Characteristics and Concomitant Procedures a
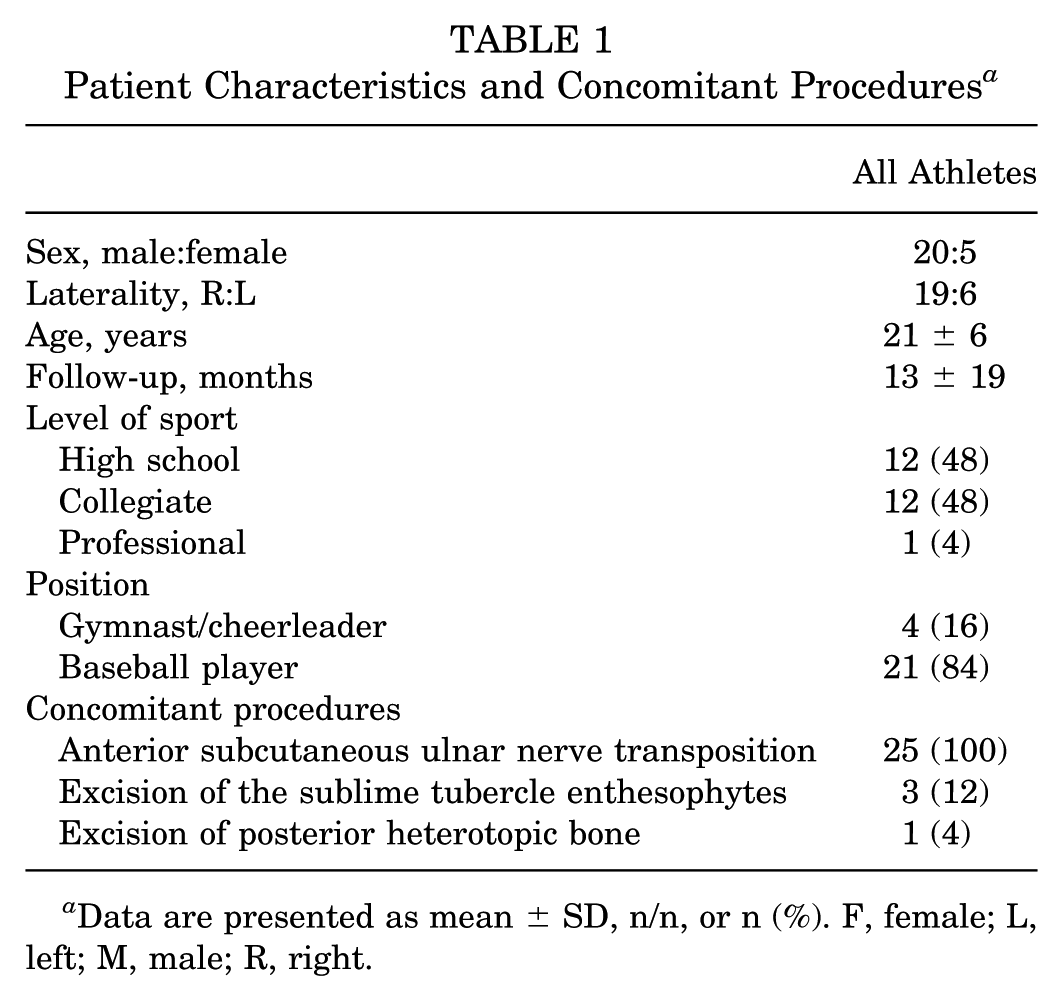
Data are presented as mean ± SD, n/n, or n (%). F, female; L, left; M, male; R, right.
In this series, concomitant procedures included anterior transposition of the ulnar nerve (100%), resection of sublime tubercle enthesophytes (3 of 25), and excision of posterior heterotopic bone from the olecranon fossa (1 of 25) (Table 1).
Return to Sport
At a mean time of 13 ± 19 months, 23 athletes (92%) were able to RTS at any level of play. Seven athletes (30%) returned to the same level as before, 12 athletes (52%) returned to a higher level, and 4 athletes (17%) returned to a lower level. Athletes categorized as returning to a lower level of play were those who resumed recreational or noncompetitive participation after completing their high school or collegiate athletic careers. The 2 athletes who did not RTS were a gymnast and a cheerleader. The gymnast did not return due to pain with activity. The cheerleader did not return due to graduating from the program. When evaluating RTS among baseball players based on primary position, 9 pitchers (56%) returned to a level higher than before, 4 at the same level (25%), and 3 athletes (19 %) at a lower level. For position players, 3 athletes (60%) returned to a higher level than before, 1 (20%) remained at the same level, and 1 (20%) returned to a lower level. Excluding the 2 gymnasts/cheerleaders who did not return, the 2 athletes who did return (100%) did so at the same level as before (100%). The mean time to RTS for pitchers, position players, and gymnasts was 13 ± 4 months, 11 ± 11 months, and 11 ± 3 months, respectively. No difference was observed in the duration of RTS between pitchers, position players, and gymnasts/cheerleaders (P = .78). No difference was observed in the duration of RTS between pitchers and position players (P = .69) (Table 2).
Return to Sport and Return to the Previous Level of Sport a
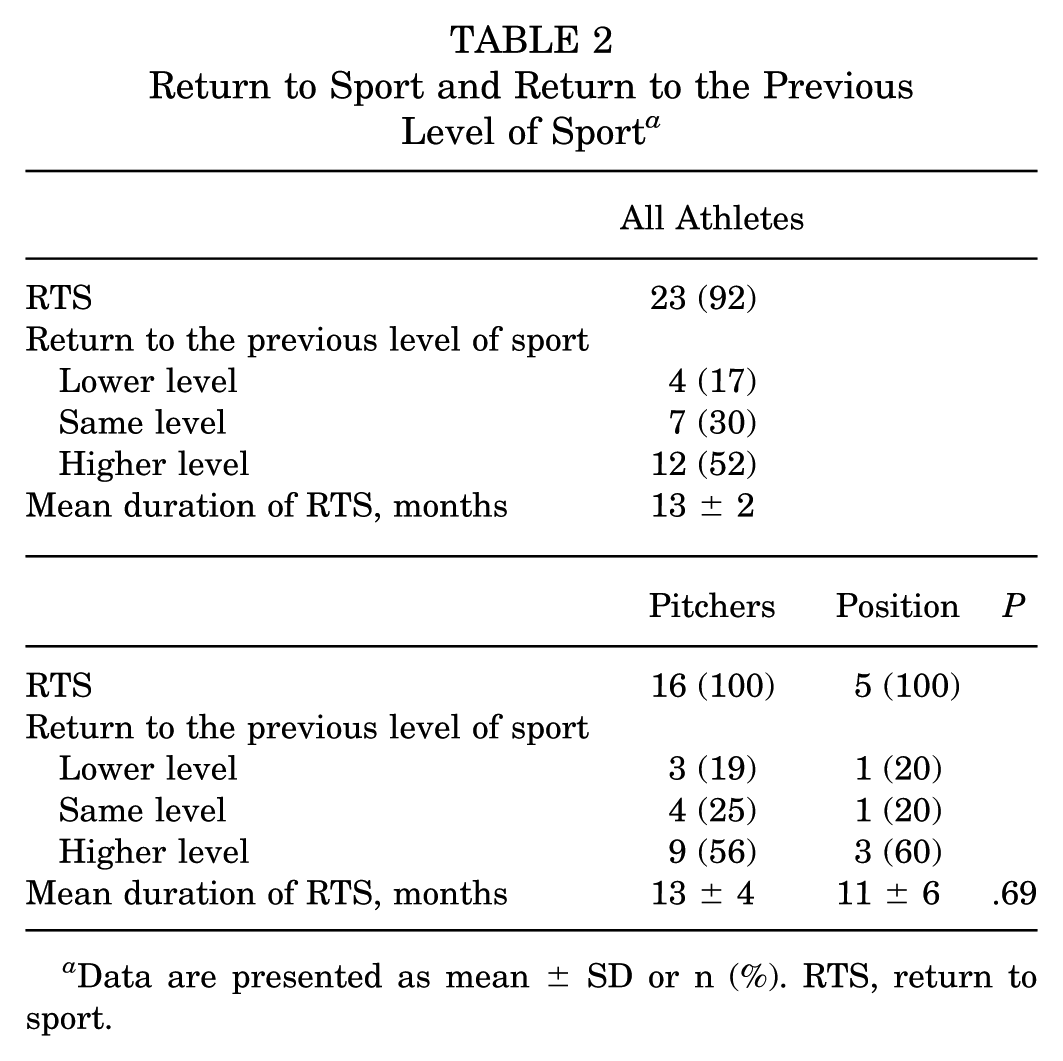
Data are presented as mean ± SD or n (%). RTS, return to sport.
Patient-Reported Outcome Measures
No significant difference was observed between pre- and postoperative SF-12 or VR-12 mental and physical component scores. Detailed values are presented in Table 3.
Postoperative PROMS a

Data are presented as mean ± SD. Postop, postoperative; Preop, preoperative; PROMS, patient-reported outcome measures; SF-12, Short Form-12 Health Survey; VR-12, Veterans RAND 12-Item Health Survey.
Only postoperative values at final follow-up were available for the following PROMs: MEPS, PROMIS UE, DASH, and VAS Pain scores. The mean postoperative MEPS, PROMIS UE, DASH score, and VAS scores were 72.5 ± 5.5, 59.2 ± 4.1, 5.6 ± 14.5, and 4.7 ± 6.9, respectively (Table 4).
Postoperative PROMS a

Data are presented as mean ± SD. MEPS, Mayo Elbow Performance Score; PROMIS UE, Patient-Reported Outcomes Measurement Information System Upper Extremity; QuickDASH, Quick Disabilities of the Arm, Shoulder, and Hand; VAS, visual analogue scale.
Functional Outcomes
Pre- and postoperative grip strength differences between the noninjured and injured arms were reported for 100% of the patients included. Grip strength was assessed preoperatively—after injury but before surgery—and at final follow-up. As true preinjury baseline values were unavailable, comparisons reflect postoperative recovery relative to preoperative (postinjury) status rather than the athlete's native strength. The mean uninjured to injured difference preoperatively was 18 ± 19 lbs and postoperatively was 15 ± 16 lbs (P = .51). All but 1 patient regained their preoperative ROM or demonstrated improvement beyond it. The 1 patient who did not regain their ROM had preoperative active flexion and extension measurements of 3° to 135°, and postoperatively, they measured 10° to 140°.
Failures, Reoperations, Complications
Failure was defined as the need for a revision UCLR after the original procedure. There was 1 reported failure in this cohort, in which the patient underwent revision UCLR for a retear of the UCL allograft approximately 2 years after the index surgery. The patient was a position baseball player who complained of an insidious onset of continued posterior medial elbow pain worsened by throwing and associated ulnar neuropathic symptoms (eg, numbness) after the index procedure, with repeat MRI showing evidence of UCL retear. Intraoperative findings included a recurrent elbow UCL tear with flattening and hyperemia of the ulnar nerve. The patient underwent a revision elbow UCLR with a hamstring allograft and revision anterior transposition of the ulnar nerve. Two other reoperations were reported, both involving the removal of the posterior EndoButto. One patient reported subjective recurrent elbow joint instability during throwing. For this patient, a repeat MRI showed a stable reconstruction. This patient returned to sport at the same preinjury level.
Discussion
This study assessed clinical outcomes for throwing and overhead athletes who underwent UCLR with an allograft. The results demonstrate favorable RTS rates and early clinical outcomes, thereby adding to the limited research supporting the use of allograft in this patient population.
We demonstrated that 92% of patients returned to sport at a mean of 11.5 months after UCLR, with 83% returning to the same or higher level of sport. For overhead throwing athletes specifically, 100% returned to sport. The 2013 case series by Savoie et al 24 on UCLR with allograft in overhead throwing athletes reported a RTS rate of 95% at a mean of 10 months postoperatively. They also reported that 30% were competing at a level above the preinjury level, 58% at the same level, and 13% below the preinjury level. The data from our study are comparable to previously reported data, as evidenced by favorable RTS data, especially in the overhead-throwing athletes. However, the mean RTS time in our series (13 ± 4 months for pitchers and 11 ± 6 months for position players) is slightly longer than that reported by Savoie et al for their cohort, which included both pitchers and position players without separating RTS data by group. Altogether, the data reported in this series add to the previous literature, suggesting that allograft is a reliable option for UCLR in overhead athletes.
Additionally, the favorable PROMs data in this study support the use of allografts for UCLR in overhead athletes. Although the Patient Acceptable Symptom State (PASS) scores for the QuickDASH and PROMIS UE have been reported in the literature, none are available for UCLR. However, the PASS score for the QuickDASH questionnaire has been reported as 19 to 23 for tennis elbow, with lower scores indicating better overall outcomes. 16 The mean QuickDASH score reported in our study was 5.6 ± 14.5. For the PROMIS UE questionnaire, the PASS score for patients with general upper extremity injuries has been reported to be 45 for mild problems, 32.5 for moderate problems, and 25 for severe problems. 4 A 2018 case series on UCLR with autograft from Bartoli et al 3 reported mean QuickDASH and VAS pain scores at final follow-up (mean, 47.9 months) of 9.1 ± 12 and 1.2 ± 1.9, respectively. However, none of the included patients were overhead athletes. The relatively high mean VAS pain score (4.7 ± 6.9) at final follow-up reported in our series likely reflects the short mean follow-up duration, as many athletes were still progressing through return-to-throwing phases or had only recently resumed high-stress activity. Since VAS reflects pain during activity, athletes commonly experience transient medial elbow soreness as they resume higher-stress throwing, which does not necessarily indicate graft problems. The large standard deviation also reflects variability in both the timing of survey completion and sport demands. Importantly, this elevated pain score did not correspond to worse clinical outcomes, as athletes demonstrated high RTS rates and strong functional recovery. The mean PROMIS UE score reported in our cohort was 59.2 ± 4.1, thus meeting the PASS score for all aforementioned severities. Moreover, a study by Erickson et al 12 found no significant difference in functional outcomes scores (Kerlan-Jobe Orthopaedic Shoulder and Elbow Score, P = .251, Timmerman-Andrews score P = .181), RTS at the same level or higher as preinjury (P = .999), or number of complications between patients who underwent UCLR with allograft versus autograft. The results from our study support the use of allograft during UCLR for overhead athletes, as the postoperative PROMs reported meet commonly cited PASS scores for the associated PRO questionnaires, indicating favorable clinical outcomes overall.
Our low complication rate (4%; 1 of 25) further supports the advantages of allograft use, as it eliminates the risks of donor-site morbidity and other adverse events associated with autograft harvest. Importantly, there were no cases of ulnar neuropathy or wound complications, despite all patients in this series undergoing anterior subcutaneous transposition of the ulnar nerve. Our complication rate is consistent with the 6% rate previously reported by Savoie et al 24 for allograft UCLR in overhead athletes. Additionally, these rates compare favorably with complication rates reported for autograft reconstruction, which average 10.2% but have been reported as high as 18% to 40% in select series.8,9,26
It has been reported that the use of allografts increases the risk of graft rejection because the allograft is subject to an immune-mediated response from the host's recognition of donor-specific antigens. This phenomenon is less common with autografts. 19 While there is a theoretical increased risk of infection with allografts compared with autografts, there are multiple studies supporting that there is no significant difference in infection rates between these graft options.1,2,14,21 The results in our study support this notion, as there was no incidence of infection or graft rejection. Moreover, there is debate over whether sterilization and handling procedures for allografts negatively affect graft integrity, thereby increasing the risk of graft failure. 13 This idea, however, has been challenged by studies that have shown no significant difference in revision or failure rate for sterilized ACL allografts when compared with autografts and nonsterilized allografts.6,7 The results in our study support the maintenance of the structural integrity of allografts using our tissue bank's non-irradiated sterilization process because of our low incidence of failure (4%; 1 of 25) within our population. Additionally, the high RTS rate highlights the maintenance of the allograft's structural integrity, especially in overhead athletes who undergo repetitive high-energy motions. Therefore, when considering graft type for UCLR, our results indicate that the risk of infection and graft rejection with an allograft is low, and importantly, the non-irradiated, aseptically processed allografts used in this study did not demonstrate evidence of compromised structural integrity, as reflected by our low failure rate and favorable clinical outcomes.
The present study is not without limitations. First, it was a retrospective case series without a control group, and therefore, no direct comparison could be made with autograft UCLR. Although autograft UCLR cases are performed within the same practice, variability in surgical technique, surgeon preference, and patient population would introduce significant confounding, limiting the validity of a comparative analysis. As such, this study was intentionally designed to focus exclusively on outcomes after allograft UCLR, providing updated data specific to this graft type. Future prospective comparative studies directly evaluating allograft versus autograft outcomes are warranted to further delineate their relative efficacy and long-term outcomes. Second, our study includes only throwing and overhead athletes; therefore, it may not apply to the general population. Third, the lack of preoperative PRO data for many questionnaires may hinder the ability to assess the intervention's true clinical impact. Fourth, the mean follow-up duration of 13 months is relatively short and may underestimate the final RTS rate or level. Future studies with longer-term follow-up are warranted to characterize sustained outcomes better. Fourth, we did not collect objective performance metrics such as ball velocity, spin rate, or innings pitched, which limits our ability to assess postoperative performance changes beyond PROMs and clinical outcomes. Finally, our study has a smaller patient cohort than other articles on similar topics.12,17,20,22,24
Conclusion
Overall, our study supports the utilization of hamstring allograft for throwing and overhead athletes undergoing UCLR. The high RTS rates, favorable PROMs, and low complication incidence support hamstring allograft as a potential alternative graft option that eliminates donor-site morbidity.
Footnotes
Final revision submitted December 12, 2025; accepted December 19, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: N.N.V. has received hospitality payments from Abbot Laboratories, Axonics Inc, Boston Scientific Corporation, Foundation Fusion Solutions LLC, IBSA Pharma Inc, Nalu Medical Inc, Nevro Corp, Orthofix Medical Inc, Pacira Pharmaceuticals Incorporated, Relievant Medsystems Inc, Salix Pharmaceuticals, Spinal Simplicity LLC, Vericel Corporation, and Vertos Medical Inc; research support from Arthrex, Inc, Breg, Ossur, Smith & Nephew, and Stryker; consulting fees from Medacta USA Inc and Stryker; royalties from Arthrex, Inc, Graymont Professional Products IP LLC, Smith & Nephew, and Stryker; and support for education from Medwest Associates; and is a board or committee member for American Orthopaedic Society for Sports Medicine, American Shoulder and Elbow Surgeons, and Arthroscopy Association of North America. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was waived by Rush University Medical Center.