
Abstract
Background:
Although numerous studies have reported on the redislocation rate and functional results of arthroscopic treatment for anterior shoulder instability in athletes, they have not disclosed outcomes in the high-risk group of elite handball players.
Purpose:
To investigate the postoperative outcomes of arthroscopic treatment for anterior shoulder instability as well as the return-to-sport (RTS) rate in professional handball players.
Study Design:
Case series; Level of evidence, 4.
Methods:
Involved in this study were 44 competitive handball players (47 shoulders) who underwent arthroscopic anterior capsulolabral reconstruction between 2010 and 2018 and had a minimum follow-up of 24 months. After surgery, patients completed a questionnaire that collected Rowe and American Shoulder and Elbow Surgeons (ASES) scores and RTS data, and we compared these results with their preoperative scores. We also compared results according to the following subgroups: true dislocations versus recurrent subluxations, younger (<20 years) versus older (≥20 years) age, male versus female sex, and shorter versus longer duration of instability. Statistical analysis included the paired-samples t test and nonparametric Fisher exact test.
Results:
The mean follow-up period was 52.2 ± 21.4 months. There were 4 shoulders (9%) with recurrent instability. There were significant preoperative to postoperative improvements in the mean Rowe score (from 45.2 to 91.8) and mean ASES score (from 70.6 to 95.7) (P < .001 for both). Overall, the RTS rate was 83%, and 64% (30/47 shoulders) were able to return to their preinjury level. The RTS rate was significantly lower in the younger players than in the older players (46% vs 86%, respectively; P = .005).
Conclusion:
The study results indicated that handball players with anterior shoulder instability can be treated using arthroscopic labral reconstruction successfully and 83% of the athletes were able to RTS activity. The handball players aged ≥20 years returned to their preinjury level of sport at a higher rate than did those aged <20 years.
Handball is one of the most popular team sports around the globe. To date, >10 million players are registered, and the majority of them are aged <18 years. Over the past decades, handball has become increasingly competitive. Along with this, the intensity and frequency of training sessions and matches have increased. The shoulder joint of handball players is prone to injuries because of the intensive overhead activity as well as many direct contacts and collisions with the other players. 3,11
Anterior shoulder instability is a common problem among athletes, especially in overhead and contact sports. It can be a consequence of a major single injury or more frequently caused by repetitive microinjuries. Nonoperative treatment is not a valid option for elite athletes, as it leads to an unacceptably high reinjury rate. 8,13,15,19,40 Thus, operative treatment is recommended. Most shoulder surgeons prefer arthroscopic labral reconstruction if there is no significant glenoid bone loss. 13,31,33 In cases of significant bone loss, the Latarjet procedure can be a good alternative. The overall results are satisfying from the aspects of recurrence and function. 2,21 Moreover, continued participation in the sport is the most important factor for athletes after surgery. 1,4,39 The return-to-sport (RTS) rate after arthroscopic labral reconstruction is relatively high for the general athletic population 9,12,16,23,29,30 ; however, this rate has been shown to be lower among overhead athletes. 8,26,34
The primary purpose of this study was to investigate the clinical outcomes of patients treated for anterior shoulder instability using arthroscopic Bankart repair in professional handball. The secondary purpose was to report the incidence of recurrent instability, the RTS rate, the level of RTS, and the time to RTS in elite handball players. We also sought to evaluate the effect of age, sex, degree of instability (dislocation vs subluxation), and duration of instability on the outcomes. Our hypothesis was that subluxation, older age, female sex, and shorter duration of instability would have positive effects on the postoperative results.
Methods
All procedures and protocols were in accordance with the ethical standards of the institutional research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. The study was approved by the regional ethics committee. The participants signed informed consent to participate in the study.
In this retrospective study, 47 shoulders of 44 professional handball players (national team, first and second leagues) were included (mean ± standard deviation age, 21.6 ± 6.5 years; 24 male and 23 female). The right shoulder was treated in 27 cases, and the left shoulder was treated in 20 cases; the dominant side was treated in 34 cases. All handball players who underwent arthroscopic capsulolabral reconstruction for traumatic anterior glenohumeral instability with a minimum follow-up of 24 months were included. All patients were treated between 2010 and 2018 by a single shoulder surgeon (A.P.). The diagnosis of anterior instability was based on the patients’ history as well as physical examination and magnetic resonance imaging findings. Exclusion criteria were glenoid bone defects of >20%, an engaging Hill-Sachs lesion, concomitant rotator cuff lesions, atraumatic and multidirectional instability, and any previous shoulder surgery.
Surgical Procedure and Rehabilitation
Arthroscopic capsulolabral reconstruction was performed using FASTak titanium single-loaded suture anchors (Arthrex) in all cases with patients under general anesthesia. After labral mobilization and glenoid rim debridement, 2 to 4 anchors were inserted into the anterior glenoid rim. A sliding knot with 3 alternating post half-hitches was used for capsulolabral repair.
Postoperatively, all patients wore a sling for 4 weeks. Physical therapy consisted of elbow and wrist exercises in the first 3 weeks, and then passive and active assisted forward flexion was initiated. After 4 weeks, the patients started external rotation in a position of 0° of elevation and continuously kept advancing with elevation. Active motion, abduction, and external rotation were allowed from 6-week follow-up. Strengthening exercises were started at 8 to 10 weeks postoperatively and were followed by a sport-specific exercise program. Return to handball training was permitted not earlier than 4 months postoperatively.
Clinical Evaluation
Descriptive data of the patients were recorded as age, sex, injured side, side dominance, and competition level (national team, first or second league). Preoperative Rowe and American Shoulder and Elbow Surgeons (ASES) scores were obtained retrospectively from the medical charts. 29,31
At the final clinical follow-up, the patients were asked to complete a questionnaire with Rowe and ASES scores. 29,31 Their level of pain, shoulder function, and instability as well as their time to RTS were recorded. All patients were asked to rate their satisfaction with the outcome of the surgical procedure (very satisfied, satisfied, moderately satisfied, or not satisfied). In addition, their level of RTS was assessed.
Statistical Analysis
The paired-samples t test was used to compare the preoperative and postoperative Rowe and ASES scores and to analyze the functional results and time to RTS according to subgroups. The following subgroups were utilized for analysis: younger (<20 years; n = 26) versus older (≥20 years; n = 21) age, true dislocations (n = 21) versus recurrent subluxations (n = 26), male (n = 24) versus female (n = 23) sex, and shorter (n = 26) versus longer (n = 21) duration of instability. We defined longer duration as >6 months from the first instability event for athletes with recurrent subluxations and as >3 dislocations for athletes with true dislocations.
The nonparametric Fisher exact test was used to compare the RTS rate of the subgroups; given that this method is more computationally intense, it is best used for smaller samples. For statistical analysis, the R software package (Version 3.6.3; R Foundation for Statistical Computing) was used. The significance level was set at P < .05. Our post hoc power analysis indicated a statistical power of 92.3% using a sample size of 47 participants, a large effect size (0.5), and an α value of .05. Therefore, our analysis was suitable for demonstrating large differences between subgroups. Using the generally accepted statistical power of 80.0%, α value of .05, and sample size of 47, we obtained an effect size between medium (0.3) and large (0.5).
Results
All patients were available for follow-up; the mean follow-up period was 52.2 ± 21.4 months. There were 4 shoulders (9%) with recurrent instability; all of these shoulders underwent revision surgery, with athletes in 3 cases being able to continue playing handball at a lower level and an athlete in 1 case giving up playing competitive handball. Of the 47 shoulders treated, patients did not report shoulder pain in 33 cases; there was occasional pain in 10 cases; and there was moderate pain in 4 cases, which was mainly activity related. Athletes regained their full range of motion in 33 cases, while 14 shoulders had slightly decreased (<10°) external rotation in 90° of abduction. Subjectively, handball players in 3 cases indicated that they were “not satisfied” with the outcome of treatment, in 2 cases were “moderately satisfied,” in 7 cases were “satisfied,” and in 35 (74%) cases were “very satisfied” with the postoperative result. Of the cases that did not have a “very satisfied” response (n = 12), only 1 athlete (8%) was able to return to the preinjury level of handball compared with 29 (83%) shoulders from the “very satisfied” group (P < .001).
Clinical Outcomes
Overall, the RTS rate was 83%. Moreover, 64% (30/47 shoulders) were able to return to their preinjury level, athletes in 7 (15%) cases changed the type of sport, and only 1 player (2%) gave up his sport career. When analyzing by subgroup, the rate of return to the preinjury level was significantly lower in the younger age subgroup than in the older age subgroup (P = .005; 95% CI, 1.75 to ∞). The odds ratio of an athlete returning to sport was 6.7 times higher if his or her age was ≥20 years at the time of surgery (Table 1). Moreover, 3 recurrences occurred in the younger subgroup (12%) compared with only 1 recurrence in the older subgroup (5%); none of these athletes was able to return to his or her preoperative sport level. The difference was not statistically significant (P = .31).
Return to Preinjury Level of Sport a
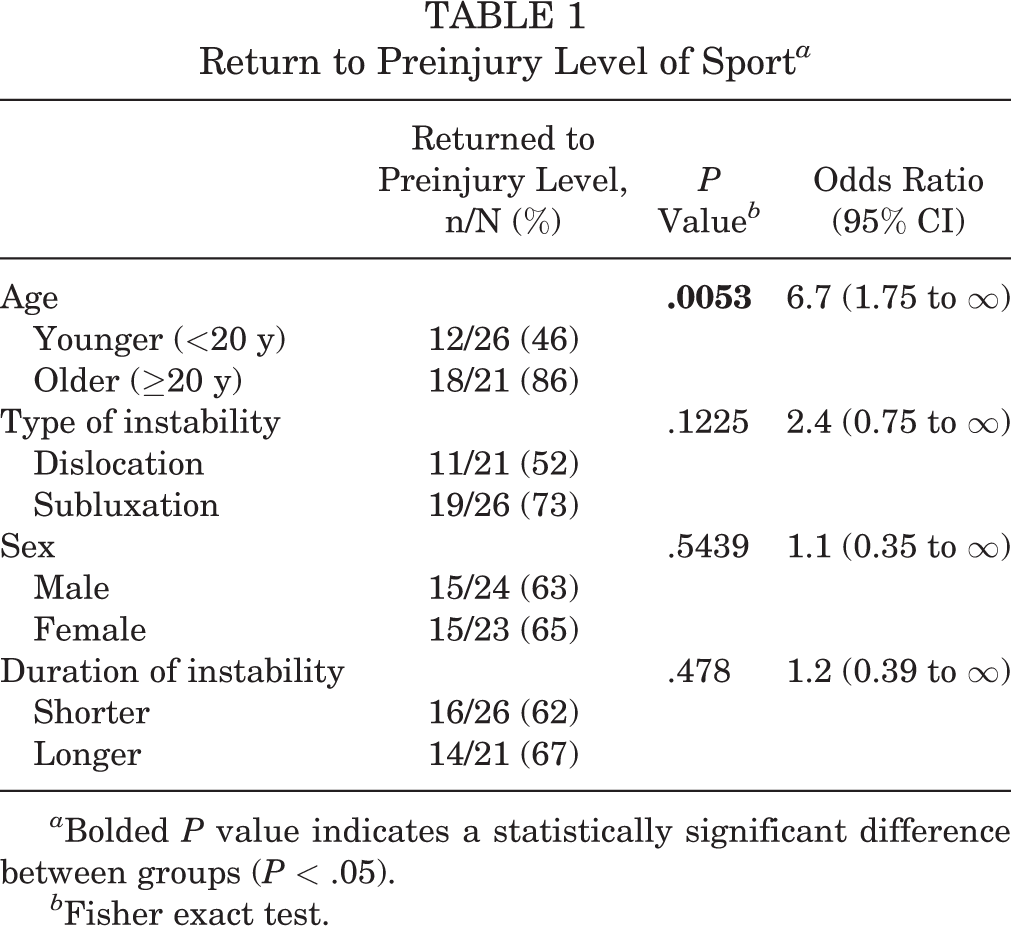
a Bolded P value indicates a statistically significant difference between groups (P < .05).
b Fisher exact test.
The mean time to RTS was 6.2 ± 3.1 months. There was no significant difference regarding the time to RTS in any of the subgroups (Table 2).
Postoperative Outcomes a
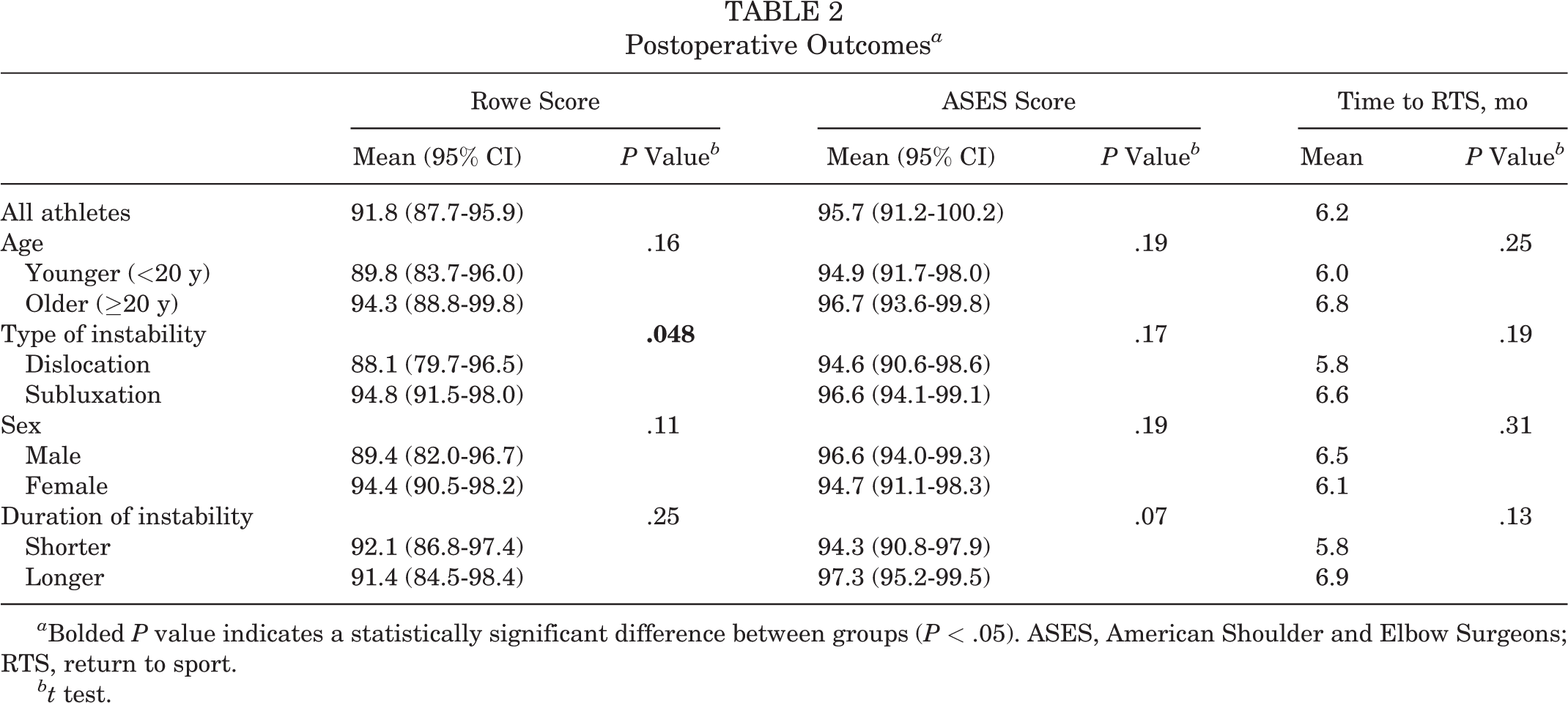
a Bolded P value indicates a statistically significant difference between groups (P < .05). ASES, American Shoulder and Elbow Surgeons; RTS, return to sport.
bt test.
Overall, the mean Rowe and ASES scores increased significantly from preoperatively to postoperatively (from 45.2 ± 11.0 to 91.8 ± 14.0 and from 70.6 ± 6.4 to 95.7 ± 7.4, respectively; P < .001 for both). When analyzing by subgroup, there were no significant differences in outcome scores by age. The subluxation subgroup showed a 2.4 times better chance of returning to the preinjury level than did the dislocation subgroup (73% vs 52%, respectively), but this difference was not statistically significant (P = .12; 95% CI, 0.75 to ∞). The subluxation subgroup had a significantly higher Rowe score versus the dislocation subgroup (94.8 vs 88.1, respectively; P = .048; 95% CI, –∞ to 0.13), although the ASES scores were not significantly different (Table 2). There was no significant difference in outcome scores according to sex or duration of instability (Table 2).
Discussion
The most important finding of the present study was that arthroscopic labral reconstruction resulted in excellent clinical outcomes in competitive handball players, who constitute one of the most injured populations among athletes because of the combination of overhead activity and contact with other players. 3,11 It should be noted that these conclusions were based on the data of patients who underwent arthroscopic labral reconstruction, and the data of patients who underwent other comparative surgical procedures were not considered in this article.
The postoperative Rowe and ASES scores in our study were excellent in the majority of the patients. Nevertheless, for these athletes, the most important aspects of the outcome of surgery are the ability and time to RTS. 1,4,39 Our overall RTS rate was good; 83% of the athletes were able to continue playing handball postoperatively, but only 64% were able to return to their preinjury level. Castagna et al 9 found that 81% of athletes returned to their preinjury level, but their patients underwent surgery acutely after a traumatic instability event. Furthermore, their rugby and water polo players had a significantly increased incidence of recurrence. 9 Similarly, Saper et al 32 concluded that 78.1% of patients returned to the same level of competition in collision and contact sports. Mazzocca et al, 23 using an arthroscopic suture anchor technique, had a 100% RTS rate in 18 contact and collision athletes, while Yamamoto 38 observed that only 48% of contact athletes were able to fully return to their preoperative sport level. These different outcomes can be explained by the differences in study protocols and study population.
However, Bessière et al 5 found that competitions or high-level practices are predictors of recurrent instability in patients who have undergone arthroscopic Bankart repair. We also found that athletes aged <20 years at the time of surgery had a significantly decreased chance of returning to their preinjury level versus the athletes aged ≥20 years. This result was also found by some authors, 5,10,26,36,37 who moreover stated that the type of sport was an important influencing factor. 9,14,15,23,25,26,28 In addition, Bessière et al found that athletes’ RTS rate was lower not only after arthroscopic labral reconstruction but also after the Latarjet procedure. Our study is, as far as we know, the first to specifically evaluate the postoperative results of competitive handball players, providing sport-specific data about a shoulder stabilization procedure. This can be important for patients, as this information may influence their decisions before surgical treatment. It is also worth considering that different extrinsic and intrinsic factors, such as age, competing motivation, and residual stress, can influence athletes’ decision to RTS. 35 In our younger aged subgroup, motivation and the fear of recurrence may have influenced the athletes’ final decision. Our data showed that competitive handball players aged ≥20 years were able to RTS easier than were younger players without a professional contract. Another potential reason for the lower rate of RTS for younger athletes is that they might choose to prioritize their education over their sport career at that time.
In our study, the mean time to RTS was 6.2 months. There was a tendency for younger players, athletes in the dislocation subgroup, and players with a shorter instability period to be able to RTS faster compared with older patients, athletes in the subluxation subgroup, and players with a longer instability period. None of these differences was statistically significant. Ciccotti et al 10 evaluated the criteria for RTS in the literature and stated that the time from surgery is the most commonly used factor besides shoulder strength, range of motion, pain, stability, and proprioception. In their review, the average time to RTS was 6 months, which is similar to that in our study. 10
The rate and level of RTS, however, are the most important factors for athletes; the recurrence rate is also a significant factor in the evaluation of a shoulder stabilization procedure. Since the late 1990s, an increasing number of studies has noted the high recurrence rate after arthroscopic labral reconstruction. 5,7,20,22,32 Other authors have compared the results of arthroscopic and open Bankart and Latarjet procedures through meta-analysis. 1,6,17 Ialenti et al 17 found a significantly lower recurrence rate after the open Latarjet procedure, but the RTS rate was similar after arthroscopic Bankart repair and the open Latarjet procedure. Over time, the results have become comparable, and more surgeons prefer arthroscopic Bankart repair if patients do not have significant bony lesions. 12,18,29,31,33 Our results are in agreement, with both the RTS rate and the recurrence rate being acceptable, even for these high-risk and competitive athletes. 24
Our subjective results showed good satisfaction among the athletes. In addition, it was noted that the handball players who were not able to RTS at their preinjury level were significantly less satisfied with the result of surgery. This observation is in accordance with the conclusions by Warth et al 39 and Plath et al 27 regarding the importance of RTS at the preinjury level after shoulder surgery.
There are some limitations of this study. We used a retrospective design, evaluated only 1 surgical method, and excluded patients with significant bone loss. Furthermore, the number of surgically treated handball players was limited, although this number may be acceptable since all athletes came from the same competitive sport. In addition, we collected all preoperative data of our patients from their medical charts, and after the athletes returned to sport, we did not assess performance measures (eg, minutes played, goals scored). Last, because the number of athletes in the different subgroups was small, the statistical analysis cannot be strong enough and is possibly underpowered. This fact may be not be important because we were not able to find a statistically significant difference in the subluxation versus dislocation subgroup regarding the RTS rate. Future prospective and multicenter studies are needed to gain more data to analyze the influencing factors for RTS in athletes.
Conclusion
Arthroscopic labral reconstruction resulted in an excellent clinical outcome with a low recurrence rate of instability in this high-risk athletic population. The handball players were able to return to competitive sport activity at a high rate, with a mean time to RTS of 6.2 months; however, only 64% were able to return to their preinjury level. The age of the athletes at the time of surgery strongly influenced the RTS level and rate. Finally, there was no significant difference in the RTS rate for sex, dislocations versus subluxations, and duration of instability.
Footnotes
Final revision submitted December 10, 2020; accepted January 12, 2021.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the regional scientific and ethical committee of Saint Emeric and Saint John Hospitals (No. 017/2019).