
Abstract
Background:
The Latarjet procedure is recommended to treat recurrent anterior shoulder instability with glenoid bone loss. Longer return-to-sport (RTS) times have been reported after the open Latarjet when compared with the arthroscopic Latarjet.
Purpose:
To assess the clinical outcomes and RTS in athletes who underwent an arthroscopic Latarjet.
Study Design:
Case series; Level of evidence, 4.
Methods:
This study included 46 professional athletes with recurrent anterior shoulder instability who underwent an arthroscopic Latarjet between 2010 and 2016. Patients were divided by type of sport: noncollision and nonoverhead (n = 22), collision and martial arts (n = 13), and overhead (n = 11). Sport activity was evaluated with the Kerlan-Jobe Orthopaedic Clinic (KJOC) score, Subjective Patient Outcome for Return to Sports score, and RTS time. Clinical results were evaluated by Constant-Murley score, Walch-Duplay score, and range of external and internal rotation. Complication rates, recurrence of shoulder instability, and number of revision procedures were recorded. Correlation tests were used to assess the relationship between measured parameters.
Results:
The mean ± SD patient age was 27.1 ± 7.3 years, and the mean follow-up was 50.7 ± 18 months. Overall, 44 patients (95.7%) returned to their previously practiced sports, and 40 (87%) returned to their preinjury levels. The RTS time was 5 ± 1.4 months, with no significant difference among sport types. KJOC and Subjective Patient Outcome for Return to Sports scores were 95.2 ± 5.6 and 9.5 ± 1, respectively. Significant pre- to postoperative improvement was seen on the Constant-Murley score (from 54.3 ± 9.4 to 87.9 ± 8.2; P = .001) and Walch-Duplay score (from 53.7 ± 7.3 to 88.1 ± 10.7; P = .001). Mean postoperative external and internal rotation was 72.8° ± 18.6° and 81.3° ± 11.3°. Procedure-related complications occurred in 10 patients (21.7%); recurrence of shoulder instability was observed in 4 (8.7%); and 4 (8.7%) underwent revision surgery. A worse Walch-Duplay score was significantly associated with longer RTS time (r = –0.39; P = .019) and lower KJOC score (r = 0.29; P = .03).
Conclusion:
There was a 95.7% RTS rate after the arthroscopic Latarjet procedure, although the procedure was not free from complications.
Keywords
Recurrent anterior shoulder instability is a common pathology in young active patients, particularly those playing contact sports. 27,38 Surgery is indicated after failure of nonoperative treatment in posttraumatic recurrent anterior instability, especially in professional athletes. Over the years, several surgical techniques have been described to stabilize the shoulder. The main goals of these procedures are to restore glenohumeral joint stability and function and to allow athletes to return to sport (RTS) at a competitive level and as early as possible with minimal surgery-related complications.
Traditionally, the most popular procedure was the open Bankart repair, 4 which was superseded by the arthroscopic technique. 3 However, the results of arthroscopic Bankart repair reflect a high recurrence rate in young athletes, with some studies reporting recurrent instability in 48% of the patients aged ≤20 years during long-term follow-up. 9,17,32,33 Moreover, for the combined Bankart and Remplissage procedure, 71% of patients were able to return to restriction-free sport, 8 and 77.8% were able to return to their previous levels. 16 To meet the expectations of such a high-demand group of patients, bony augmentation techniques have gained popularity in recent years, especially the open Bristow-Latarjet method, 26 later developed as an arthroscopic technique. 25
Several studies have been published on RTS after the open Latarjet procedure in athletes. 1,5,6,10,12,20 –22 Because the classic Latarjet procedure is performed as open surgery, it constitutes a difficulty of deeper exposure, a bigger risk of bleeding, as well as damage to the subscapularis muscle, and it can require a longer time to RTS. As such, there is an increasing interest in the arthroscopic Latarjet. 10,19,20 However, there is currently only 1 study reporting results and RTS after the arthroscopic Latarjet. 10
The aim of this study was to report the outcome of the arthroscopic Latarjet in professional athletes in terms of function, complications, time from surgery to RTS, and RTS rate and level. We hypothesized that there will be a high rate of RTS at the preinjury level and that RTS times will be shorter when compared with the open Latarjet.
Methods
Ethics committee approval was received for the study protocol. Professional athletes with recurrent anterior shoulder instability who underwent an arthroscopic Latarjet procedure between 2010 and 2016 were eligible for inclusion to the retrospective study. Professional athletes were regarded as athletes who treat sport as a primary occupation and source of income. All surgical procedures were performed by 2 surgeons (R.B. and A.B.), both of whom had ≥8 years of experience in performing arthroscopic shoulder surgery. The final examination was conducted by 2 authors who were not engaged in performing the surgery (H.L. and W.S.). Exclusion criteria were as follows: voluntary instability, moderate or severe osteoarthritis per the Samilson and Prieto classification, 34 and any previous operative and nonarthroscopic shoulder instability treatment. In addition, patients with follow-up <2 years were excluded.
Preoperative radiologic assessment included plain anteroposterior and axial radiographs and 1.5- or 3.0-T magnetic resonance imaging (MRI) to analyze the presence of osteoarthritis and concomitant pathologies, such as rotator cuff tears, long head of biceps tendon pathology, or Hill-Sachs lesion. Sagittal MRI cut, as described by Owens et al, 31 was used to assess glenoid bone loss (GBL) and the glenoid track. 15 The indication for an arthroscopic Latarjet was a GBL of ≥15% resulting in a lack of anterior curvature, thereby creating a straight vertical cutoff line called a “flatline” 9 and/or an off-track Hill-Sachs lesion. 15
Surgical Technique
Surgery was performed with the patient in the beach-chair position under general anesthesia and an interscalene nerve block. The arthroscopic Latarjet procedure performed in our hospital was a modified technique of the one described by Lafosse et al. 24,25
During the initial arthroscopic examination, labral injury, GBL, and Hill-Sachs lesion were confirmed, and concomitant pathologies, such as a SLAP lesion (superior labrum anterior and posterior), rotator cuff tear, or posterior labrum tear, were identified and repaired in the case of their presence. By viewing through the posterior portal, electrocautery was used to resect the rotator interval at the upper border of the subscapularis. The anteroinferior labrum between 2 and 5 o’clock was resected to expose the glenoid neck. The inspection hole in the capsule between the glenoid neck and the subscapularis was performed to find the proper place of the subscapularis muscle split. The middle glenohumeral ligament was preserved if it did not interfere with creation of the inspection hole in the capsule. While making a decision on the subscapularis split location, we sought to find particular tendinous cords within the subscapularis muscle (Figure 1).

Particular tendinous cords (white arrows) in the subscapularis muscle as viewed from a posterior portal.
Only proper visualization of the tendinous cords from the articular side allows one to perform the split between the desired cords, defined as the lower third of the subscapularis muscle, as this “tendon junction” provides compression against the anteroinferior glenoid rim. Preoperative planning based on the MRI helps to predict the number and position of tendinous cords (Figure 2).

Preoperative (A) coronal and (B) sagittal magnetic resonance imaging planning with tendinous cords (1-5) within the subscapularis muscle.
The arthroscope was moved from the posterior to anterolateral portal, and the anterior portal was used as a working portal to liberate the anterior and lateral parts of the conjoint tendon. The soft tissue pouch between the subscapularis and conjoint tendon was opened to find a prepared split and to visualize the axillary nerve to avoid any nerve injury. The subscapularis muscle was retracted anteriorly, and a new superior portal parallel to the glenoid was performed to introduce the bur and to prepare the glenoid neck more conveniently. The same portal was also used to prepare the contact surface for the coracoid graft (Figure 3).

(A) A glenoid neck preparation fly bur is introduced through a parallel portal. (B) Graft-shaping procedure by a bur inserted through accessory superior portal.
When intra-articular preparation was completed, the arthroscope was moved to the anterior portal to finish preparation of the conjoint tendon and coracoid process. The medial border of the coracoid was released from the portal made just above the center of the coracoid process. After the coracoid was harvested, the graft was fixed to the custom-made graft provider (Figure 4) inserted through the anteroinferior portal.

Custom-made graft provider.
After the coracoid process was harvested, a subscapularis split was performed. The switching stick was introduced through the posterior portal and then, under the control of the camera, through a previously prepared inspection hole in the capsule and subscapularis muscle (Figure 5A). Afterward, external rotation (ER) was performed, resulting in blunt dissection of the subscapularis muscle fibers by the switching stick (Figure 5B).

Performing the subscapularis split as viewed from an anterior portal. (A) A switching stick, as inserted through the posterior portal and under control of the arthroscope in the anterior portal, is introduced into a previously prepared aperture in the capsule. (B) Afterward, external rotation is performed, resulting in blunt dissection of the subscapularis muscle fibers by the switching stick.
Given the many cases of osteolysis of the superior part of the graft described in the literature, 24,25,39 the procedure of graft shaping was modified. The graft was shaped into a “half water drop” shape by a burr through the accessory superior portal (Figure 3B). After that, with a custom-made graft provider, the coracoid process was transferred to the anteroinferior glenoid. The position of the graft was controlled by the switching stick introduced through the posterior portal to protect the prominent position of the graft. After measurement, 2 titanium screws for fixing the bone block were fastened, and graft placement, mobility, and stability were examined. Finally, the axillary nerve and musculocutaneous nerve were liberated by the switching stick to minimize the risk of musculocutaneous nerve entrapment, as found in 66% cases within the subscapularis split 18,37 (Figure 6).

Coracoid process (black star) fixed to the anterior rim of the glenoid. (A) The musculocutaneous or axillary nerve (white star) is often located within the subscapularis split and close to the conjoint tendon (black arrow). (B) A switching stick is inserted through the anterolateral portal, and under control of the camera, the musculocutaneous nerve is liberated from adjacent tissues to prevent the nerve from excessive sling tension.
Rehabilitation Protocol
The postoperative rehabilitation protocol consisted of a simple shoulder arm sling to prevent pain for 3 to 4 weeks after surgery. During the time in the sling, isometric deltoid exercises and passive ER and internal rotation (IR) exercises were performed twice a day. Active range of motion movements were introduced from the third to fourth week. After 4 weeks, routine radiographs were taken to check graft and hardware position. At this time, stretching exercises were introduced as well as exercises with weightbearing. Each patient was thoroughly examined by the same author (H.L.), different from the surgeon, and the extent of full loading was assessed according to the patient’s preoperative load-bearing capability. The loadbearing examination protocol did not differ among patients and consisted of several loaded shoulder exercises performed under supervision of an examiner. Starting from week 10, gradually forced active movements were introduced to restore muscle strength and full range of motion. Three months after surgery, a control radiograph of the shoulder was performed to check for any problems with the graft or hardware. RTS was allowed in cases with radiographic signs of graft union (graft and glenoid rim bone structure continuity), satisfactory range of motion, ability to maintain strengthening exercises, and a negative apprehension test result. All athletes were introduced with occupation-specific workouts before complete RTS.
Outcome Measures
RTS and Sports Activity
We defined RTS in this study as the ability to perform full-load training without pain or significant limitation of the range of motion. We recorded the RTS rate, time of RTS, and whether athletes returned to their preinjury levels. To assess the relationship between RTS rate and type of sport, patients were divided into 3 groups: Group 1: noncollision and nonoverhead (eg, weightlifting, skiing) Group 2: collision (eg, hockey, soccer) and martial arts Group 3: overhead (eg, volleyball, handball).
Patients were allocated to groups of sport respectively to patient-related prevalence of 1 of the aforementioned sports. Previous studies showed a 76.8% rate of RTS after arthroscopic stabilization for overhead athletes 11 and 90% for collision athletes. 13
A 10-item Kerlan-Jobe Orthopaedic Clinic (KJOC) score 2 and Subjective Patient Outcome for Return to Sports (SPORTS) score 7 were used at final follow-up to assess the possibility and quality of sport performance. The KJOC score (maximum, 100) aids in accurate assessment of overhead athletes after injury, treatment, and/or surgery and provides a performance-based measure of outcomes in a high-demand population. 2 The SPORT score is a simple yet validated tool to assess athletes after surgery for shoulder instability. 7 It measures pain, performance, and effort, with a maximum score of 10.
Functional Outcomes
Objective shoulder assessment was carried out with pre- and postoperative comparison of the Constant-Murley score 35 and Walch-Duplay score. 36 The postoperative Subjective Shoulder Value (0-100) was also assessed. Postoperative range of ER and IR, which is crucial in many sport activities, was measured in adduction with the use of the goniometer (EasyAngle; Meloq) and compared with the contralateral side. A positive outcome in this study was defined as full restoration of joint stability in terms of the absence of any dislocations and subluxations and an RTS at the same level as before dislocation.
Complications
Complication rates, recurrence of shoulder instability, and number of revision surgical procedures per patient were recorded.
Statistical Analysis
All data were collected and analyzed using PQStat software version 1.8.4 (PQStat Software). The normality of distribution for each parameter was checked with the Shapiro-Wilk test. Outcome comparisons among sport groups were performed by analysis of variance. Pearson correlation analyses were performed to assess the relationship between outcome measures. Statistical significance was set at P < .05.
Results
Initially, there were 57 shoulders and 57 patients. During the follow-up, 11 patients were lost to follow-up; thus, 46 patients (41 male and 5 female) with a mean ± SD age of 27.1 ± 7.3 years were included in the final analysis. The mean follow-up was 50.7 ± 18 months (Table 1). The dominant shoulder was involved in 23 patients. The time from first dislocation to arthroscopic Latarjet surgery was 4.7 ± 4.7 years. The mean operative time was 118.3 ± 30.7 minutes. Twelve patients (26%) had a GBL between 15% and 25%, while the remaining 34 (74%) had a GBL >25%.
Patient and Surgery Characteristics (N = 46) a

a HAGL, humeral avulsion of the glenohumeral ligament; SLAP, superior labrum anterior and posterior.
b Mean (range).
RTS and Sports Activity
After the aforementioned follow-up period, 42/46 patients (91.3%) had a stable shoulder. Of the 46 professional athletes, 44 (95.7%) returned to their sports, and 40 (87%) returned to their preinjury levels of play. There were 22 patients in group 1 (noncollision/nonoverhead), 13 in group 2 (collision and martial arts), and 11 in group 3 (overhead). The RTS and return-to-preinjury rates by sport group were, respectively, 95.5% (21/22) and 86.4% (19/22) in group 1, 100% (13/13) and 92.3% (12/13) in group 2, and 90.1% (10/11) and 81.8% (9/11) in group 3. The overall mean time to RTS was 5 ± 1.4 months (5 months for group 1, 4.6 months for group 2, and 5.3 months for group 3; P = .214).
Functional Outcomes
RTS and functional outcomes are summarized in Table 2. The KJOC and SPORTS scores were 95.2 ± 5.6 and 9.5 ± 1, respectively. Significant pre- to postoperative improvement was seen in the Constant score (from 54.3 ± 9.4 to 87.9 ± 8.2; P = .001) and Walch-Duplay score (from 53.7 ± 7.3 to 88.1 ± 10.7; P = .001). There were no significant differences in pre- to postoperative ER or IR. The mean postoperative ER (72.8° ± 18.6°) was 97.5% of the contralateral side, and the mean postoperative IR (81.3° ± 11.3°) was 95.3% of the contralateral shoulder.
Overall Postoperative Sports and Functional Outcome a
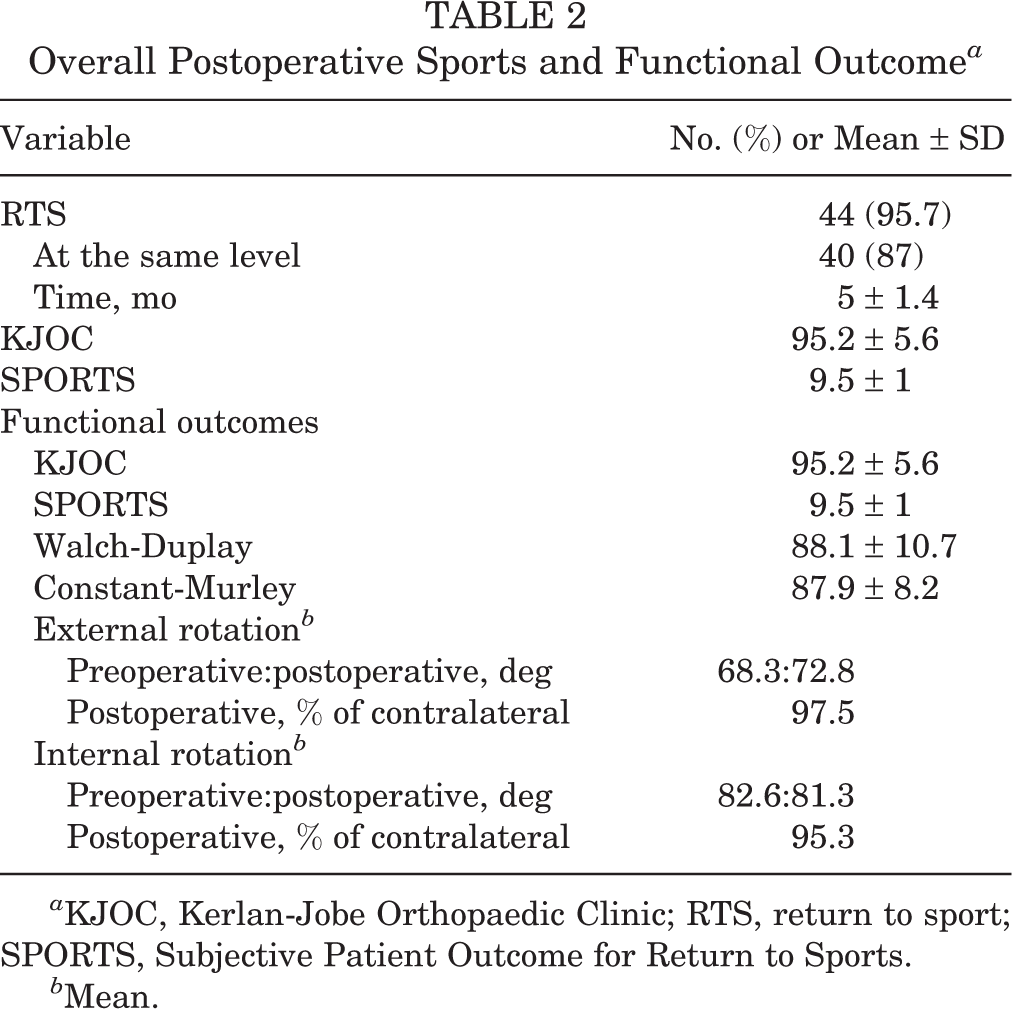
a KJOC, Kerlan-Jobe Orthopaedic Clinic; RTS, return to sport; SPORTS, Subjective Patient Outcome for Return to Sports.
b Mean.
Complications
During the final follow-up period, 4 of 46 (8.7%) patients had a dislocation after trauma during sport activity. There were no reports of subluxation during the follow-up examination. Of 4 patients with recurrence of instability, 2 (4.45%) felt persistent apprehension during sport activities. Postoperative complications occurred in 14 of 46 (30.0%) patients (Table 3), some of which were reported by the same patients.
Postoperative Complications and Additional Procedures (N = 46) a

a SLAP, superior labrum anterior and posterior.
The most common complications were pain during prolonged weightbearing or after overuse (n = 5; 10.9%), a few cases of which (n = 3; 6.5%) required removal of the superior screw. Three (6.5%) patients reported numbness on the superoanterior aspect of the forearm; 1 (2.7%) had crepitations; and 1 (2.7%) had a posttraumatic failure of hardware after a motorbike accident. This trauma led to fracture of the lower screw, which required arthroscopic removal. The arthroscopic removal of screws and debridement were the only reoperation procedures performed on our population during follow-up. The total reoperation rate was 8.7%. We did not perform additional surgery in case of shoulder redislocation. Every patient with a shoulder dislocation event after a Latarjet procedure was addressed successfully with nonoperative management (brace and physical therapy) and did not require surgery.
Additional procedures to treat concomitant pathologies during the arthroscopic Latarjet procedure were performed in 7 (15.2%) patients (Table 3). There was no significant difference between patients with and without additional treatment procedures in terms of ER range and RTS, as well as KJOC, SPORTS, Walch-Duplay, and Constant scores (P < .05).
Correlation Analysis
According to Pearson correlation analysis, performance of additional procedures for concomitant pathology was not associated with time to RTS or Walch-Duplay score (Table 4). The factors associated with lower KJOC score were recurrent instability (r = 0.385; P = .007), higher number of preoperative dislocations (r = 0.355; P = .03), and lower postoperative Walch-Duplay score (r = 0.29; P = .032). There was no correlation between type of sport (groups 1-3) and redislocation event, sports activity score, or functional score. A worse Walch-Duplay score was significantly associated with longer RTS (r = –0.39; P = .019). Recurrence of instability did not affect RTS time, Walch-Duplay score, Constant score, or ER range, but it was significantly associated with decreased KJOC score (P = .022) and SPORT score (r = 0.387; P = .005). Type of sport was not associated with recurrence of instability or complications. GBL bore no correlation with redislocation events.
Results of Correlation Analyses a

a KJOC, Kerlan-Jobe Orthopaedic Clinic; RTS, return to sport; SPORTS, Subjective Patient Outcome for Return to Sports; WD, Walch-Duplay.
b Bold P values indicate statistical significance (P < .05).
Discussion
The study results show that the arthroscopic Latarjet procedure for treatment of recurrent anterior shoulder instability in athletes averted redislocations in 91.3% of all patients. A longer time to RTS was found in those who had lower Walch-Duplay scores (r = –0.39; P = .019). It should be also emphasized that anterior instability arthroscopic Latarjet treatment did not significantly decrease the postoperative range of ER and IR when compared with the contralateral shoulder (97.5% and 95.3% of contralateral, respectively), which is crucial in many sports activities, especially for overhead athletes. The study results showed that the arthroscopic Latarjet is equally effective in terms of all measured parameters regardless of the type of sport. This is contrary to previous studies, in which overhead athletes had an RTS incidence of 76.8% after arthroscopic stabilization 11 while collision athletes reached an RTS in 90% of cases. 13
In a systematic review with 2134 patients undergoing an open Latarjet, Hurley et al 20 estimated an RTS of 88.8%, of which 72.6% of athletes returned to the same level of play at a mean 5.8 months. Kee et al 22 reported an RTS of 96%, and only 16.1% returned to the same level of sports after an open Latarjet. Recurrence of instability was observed in 5.4% of patients. In a meta-analysis comparing the open Latarjet with other open and arthroscopic stabilization techniques in athletes, Ialenti et al 21 reported an RTS of 73% for the open Latarjet with an instability recurrence rate of 3.5%. In a study by Neyton et al, 30 65% of athletes were able to RTS, and 56% were able to reach the preinjury level of sport after surgery.
To date, only 1 study has focused on the assessment of function and sport criteria after an arthroscopic Latarjet in athletes. In this study by Buckup et al, 10 89.4% of the initial 47 patients were able to perform their original sports at a predislocation level after a mean 4.6 months. Furthermore, patients who underwent Latarjet as revision surgery after failed arthroscopic Bankart repair demonstrated a tendency toward prolonged rehabilitation and longer RTS, but they did not show significantly inferior results when compared with patients after a primary Latarjet procedure. However, overhead athletes and martial arts athletes showed a significantly longer time to RTS as compared with noncollision/nonoverhead athletes. This tendency was not confirmed in our study. In the Buckup et al study, 2 patients (4.1%) had a recurrence of instability after trauma, which was comparable with our result (8.7%).
However, Buckup et al 10 did not report any complications. 10 In our study, the rate of complication was 30.4% (n = 14), but just 8.7% (n = 4) of severe cases required revision procedures (3 superior and 1 lower screw removal). The complication rate of 30.4% in our research appears to be very high at first glance. Nevertheless, it is worth mentioning that because of athletes’ very high expectations, we included even the smallest complications, such as pain during training or painless cracking. In our opinion, even the slightest ailment may alter the time and quality of professional RTS. However, in terms of serious complications (ie, those requiring revision surgery), the complication rate was comparable with that in the study by Dumont et al 14 of 62 patients, 58 of whom practiced sports. In their study, the complication rate was 7.8%, and the revision rate was 15.6%. In a multicenter study by Matais et al, 29 the complication rate was 5.6% after an arthroscopic Latarjet in a group of 390 patients. Kordasiewicz et al 23 and Meraner et al 28 reported respective complication rates of 12.6% and 6.1% after an arthroscopic Latarjet requiring revision. Note, however, that these studies were not focused on athletes. Given that the patients were exclusively professional athletes, the 8.7% revision rate appears to be an acceptable result, especially when compared with the general population. This finding suggests high efficacy of the arthroscopic Latarjet procedure for treatment of recurrent anterior shoulder instability in athletes.
Strengths and Limitations
The strength of this study is that it is a single-center series of consecutive patients that examined the outcomes of a relatively large group of professional athletes after an arthroscopic Latarjet with a mean follow-up of >4 years. This is an appropriate time to assess the efficacy and complication rate, as most athletes are likely to encounter any problems during this time span. We also note some limitations to this study. It is a retrospective case series with no comparative group to verify whether this is a superior technique. We did not report any radiologic outcomes, such as arthritic changes or graft resorption and/or osteolysis, which are known complications of Latarjet. This would have been best assessed with computed tomography, which is not routinely carried out postoperatively at our institute unless there are any concerns.
Conclusion
A success rate >90% was found after the arthroscopic Latarjet in the treatment of recurrent anterior shoulder instability in athletes. This technique provides a high RTS rate; however, the procedure is burdened with a relatively high complication rate. Further technique or equipment development may help in reducing complications.
Footnotes
Final revision submitted December 12, 2022; accepted January 27, 2023.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the regional ethics committee of Bielsko-Biala (No. 2019/05/30/2).