
Abstract
Background:
Posterior shoulder instability accounts for a small proportion of all shoulder instability, although it can affect athletes of all types, from contact to overhead athletes. Surgical treatment is quite successful in these patients; however, the literature reports a wide range of rates of return to sport.
Purpose/Hypothesis:
The purpose was to determine the return-to-sport rates after surgical stabilization for posterior shoulder instability. It was hypothesized that patients would experience a high rate of return to sport.
Study Design:
Systematic review and meta-analysis; Level of evidence, 4.
Methods:
Embase, PubMed, and MEDLINE were searched for relevant literature from database inception until April 2020, and studies were screened by 2 reviewers independently and in duplicate for studies reporting rates of return to sport after surgical management of posterior shoulder instability. Demographic data as well as data on return to sport and functional outcomes were recorded. A meta-analysis of proportions was used to combine the rates of return to sport using a random effects model. A risk of bias was assessed for all included studies.
Results:
Overall, 32 studies met inclusion criteria and comprised 1100 patients (1153 shoulders) with a mean age of 22.8 years (range, 11-65) and a mean follow-up of 43.2 months (range, 10-228). The pooled rate of return to any level of sport was 88% (95% CI, 84%-92%; I2 = 68.7%). In addition, the pooled rate of return to the preinjury level was 68% (95% CI, 60%-76%; I2 = 79%). Moreover, the pooled return-to-sport rate for contact athletes was 94% (95% CI, 90%-97%; I2 = 0%), while for throwing athletes it was 88% (95% CI, 83%-92%; I2 = 0%).
Conclusion:
Surgical management of posterior shoulder instability resulted in a high rate of return to sport, as well as significant pain reduction and functional improvement in most patients. However, only two-thirds of athletes can return to their preinjury levels of sport.
Posterior shoulder instability is often unrecognized, leading to delays in diagnosis and treatment. 20 While glenohumeral instability itself is common, posterior shoulder instability is relatively rare, representing only 2% to 10% of all shoulder instability and 4% of all shoulder dislocations.4,36,44 Similar to anterior shoulder dislocations, posterior dislocations can lead to recurrent posterior instability, albeit at a lower rate.35,36
While many patients can recall an injury to the shoulder that initiated symptoms,16,20 in the majority of patients recurrent posterior shoulder instability does not follow a frank posterior dislocation event.35,61,63 Rather, posterior instability is typically associated with repetitive and traumatic posterior loading, as seen in football linemen, or repetitive microtrauma, affecting athletes participating in overhead sports such as baseball, swimming, and tennis.20,38,47,52 Classically, the traumatic event is a posteriorly directed blow with the arm in a position of flexion, adduction, and internal rotation. 50 These posteriorly directed and often repetitive traumatic forces can lead to capsulolabral detachment, frequently described as a reverse Bankart lesion, as well as attenuation of the posterior capsule.22,32,46 In overhead athletes, the more insidious mechanism of instability is thought to be gradual failure owing to repetitive overhead movements, leading to laxity of the posterior capsule.48,59 Similar to anterior instability, posterior instability can be associated with bony glenoid erosion,16,52 as well as an impaction injury to the humeral head (reverse Hill-Sachs lesion). 18
Nonoperative management of posterior shoulder instability is still considered by many the first-line treatment16,20,24,36; however, when nonoperative treatment has failed, patients can be offered surgical management. Arthroscopic and open soft tissue repair techniques for posterior instability include repair of the posterior labrum and plication or thermal shrinkage of the posteroinferior capsule.9,19,32,45,63 With arthroscopic techniques especially, this allows for management of concomitant shoulder pathology that can affect athletes, such as superior labrum anterior to posterior (SLAP) lesions, impingement, and rotator cuff tears.1,7,14,23 Surgical management of posterior instability can also address bony pathology, in the form of posterior bone block procedures for glenoid defects8,51,54 and glenoid osteotomy to correct excess retroversion.53,62 After these surgical treatment options for posterior instability, the rate of return to sport varies considerably across studies, ranging from as low as 38% to a perfect 100%.7,10,11,20,63 The purpose of this systematic review is to determine the return-to-sport rate after surgical management of posterior shoulder instability, including the overall rate of return to sport, the rate of return to preinjury level, and the rate of return in overhead and throwing athletes, as well as the sport-specific return rate. Secondarily, this systematic review examines secondary clinical outcomes after surgical management of posterior shoulder instability.
Methods
This systematic review was conducted in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines for conducting and reporting systematic reviews. 40
Search Strategy
Three online databases (MEDLINE, Embase, and PubMed) were searched from inception to April 15, 2020, for literature addressing return to sport after surgical management of posterior shoulder instability. Search terms used to identify eligible studies included “posterior,”“subluxation,”“dislocation,”“shoulder,” and “instability” (Appendix Table A1, available in the online version of this article).
Study Screening
Studies identified during the comprehensive search were screened at the title, abstract, and full-text stages by 2 reviewers (J.K., M.M.) independently and in duplicate. Disagreements during the title and abstract screening stages were carried forward to the next stage for more in-depth review. Any disagreements at the full-text stage were resolved by consensus between the reviewers, and a senior author (O.R.A.) was consulted for any remaining discrepancies. The references of included studies subsequently underwent manual screening to identify any additional articles that may have eluded the initial search strategy.
Assessment of Study Eligibility
The research question and study eligibility were established a priori. The inclusion criteria were as follows: therapeutic studies of all levels of evidence, English-language studies, human studies, and studies reporting return to sport after surgical management of any type for posterior shoulder instability. Exclusion criteria were cadaveric studies, conference abstracts, review papers, technique guides, case series of <5 patients, and textbook chapters. As well, when 2 studies had an overlapping group of patients, the study with more recent follow-up was included.
Assessment of Agreement
The kappa (κ) statistic was used to evaluate interreviewer agreement at all screening stages. Agreement was classified a priori as follows: κ of 0.81 to 0.99 was considered nearly perfect agreement; κ of 0.61 to 0.80, substantial agreement; κ of 0.41 to 0.60, moderate agreement; 0.21 to 0.40, fair agreement; and a κ≤0.20, slight agreement. 30
Quality Assessment
The methodological quality of nonrandomized studies was evaluated using the Methodological Index for Non-randomized Studies (MINORS) criteria. 56 Using the items on the MINORS checklist, noncomparative studies can achieve a maximum score of 16, while comparative studies can achieve a maximum score of 24. Noncomparative studies were categorized a priori on the basis of a previous systematic review by our group as follows: 0 to 4, very low-quality evidence; 5 to 7, low quality; 8 to 12, fair quality; and ≥13, high quality. 55 For comparative studies, categorization was as follows: 0 to 6, very low quality; 7 to 10, low quality; 11 to 15, fair quality; and >16, high quality. 55
Data Abstraction
Two reviewers (K.G., J.K.) independently abstracted relevant data from included articles and recorded data onto spreadsheets created a priori (Microsoft Excel Version 2007). Demographic data of the patient population were recorded, such as information on preoperative sport (including contact athletes and overhead athletes), level of competition, and the surgical procedures that patients received. Data were recorded on return to sport, time to return, and return to the same level, as well as additional clinical outcomes and the rate of complications.
Data Analysis
The primary outcome was the rate at which patients returned to sport. A meta-analysis of proportions was conducted to determine the pooled rate of return to any level of sport and return to the preinjury level. Subgroup analyses were conducted where possible. To establish the variance of the raw proportions, a Freeman-Tukey transformation was applied. 15 The transformed proportions were then combined using the DerSimonian-Laird random effects model (to incorporate the anticipated heterogeneity). 13 The proportions were back-transformed using an equation derived by Miller. 37 The I2 test was used to assess heterogeneity. I2 values between 25% and 49% indicated low statistical heterogeneity; 50% to 74%, moderate; and ≥75% high. 21 For outcomes that are reported less uniformly, the results are presented in a descriptive summary fashion. Descriptive statistics—namely, means, proportions, standard deviations, and 95% CIs—were calculated using Minitab statistical software (Version 17; Minitab Inc).
Results
Literature Search
The initial literature search yielded 7148 studies, which after removal of duplicates was reduced to 4361. Systematic screening and assessment of eligibility resulted in 33 full-text studies that satisfied inclusion criteria. One study that satisfied inclusion criteria comprised a cohort of patients who were in a larger and more recent series, and so this study was excluded, resulting in 32 studies in the analysis. A PRISMA flow diagram detailing the search and screening process is displayed in Figure 1. Agreement between the reviewers was substantial at the 3 stages: title (κ = 0.71; 95% CI, 0.62-0.80), abstract (κ = 0.74; 95% CI, 0.68-0.80), and full text (κ = 1.00; 95% CI, 1.00-1.00).
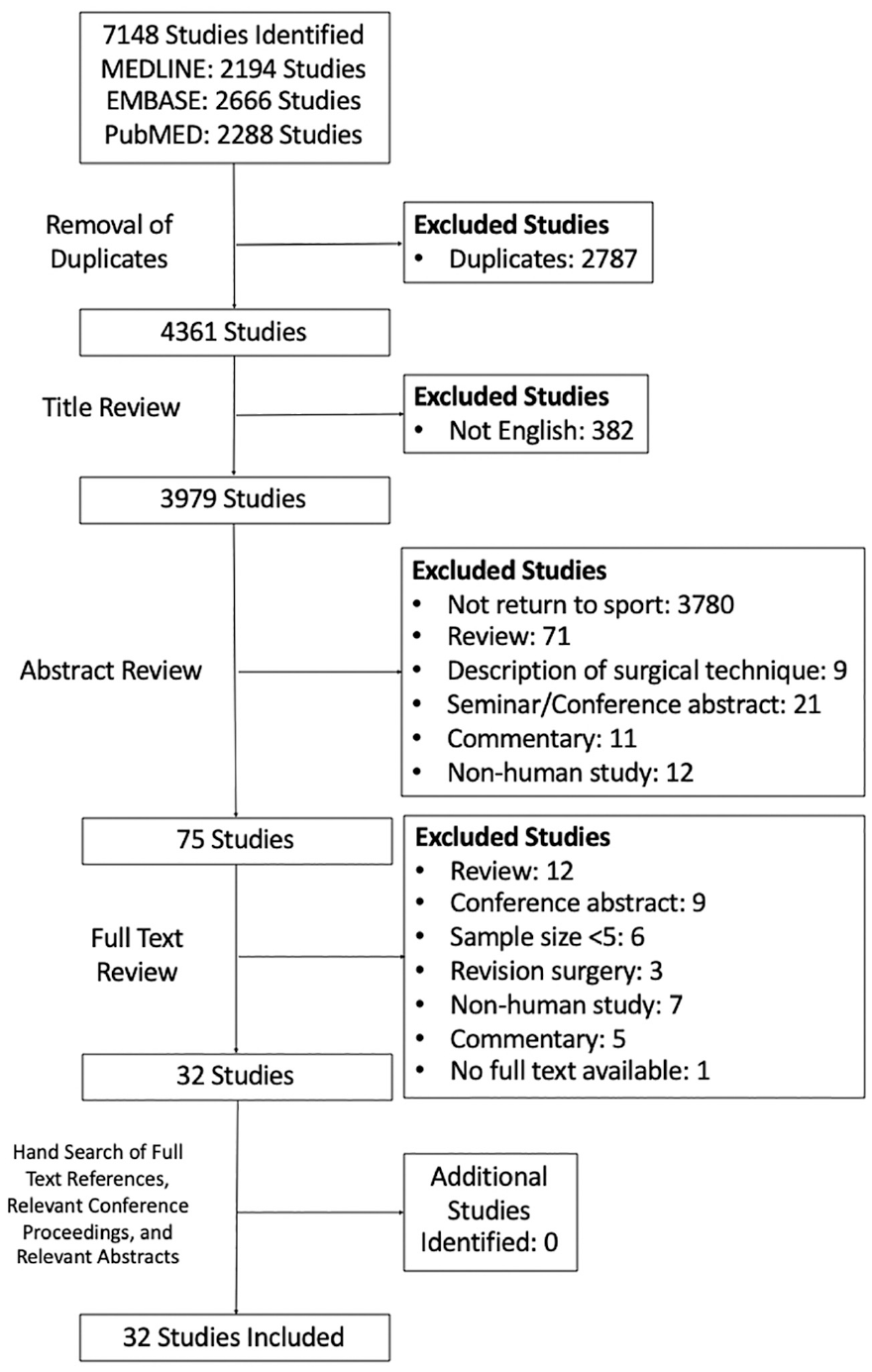
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram demonstrating the systematic review of the literature for return-to-sport outcomes after surgical management of posterior shoulder instability.
Study Quality
Among the 32 studies in this review, there were 26 case series (level 4 evidence), 4 retrospective comparative studies (level 3 evidence), and 2 prospective cohort studies (level 2 evidence). Notably this resulted in 81% (26/32) of studies involving noncomparative level 4 evidence. The median MINORS score was 10 (range, 7-12) for noncomparative studies (maximum score, 16) and 17.5 (range, 16-20) for comparative studies (maximum score, 24). Of the 32 studies, 20 (62%) cited inclusion of consecutive patients, as well as a loss to follow-up of <5%. However, only 9 (28%) reported prospective data collection, and just 1 (3%) specified unbiased outcome assessment.
Study Characteristics
Overall, 1100 patients (1153 shoulders) underwent surgical stabilization for posterior shoulder instability (Table 1). The median number of patients per study was 22 (range, 5-183). Patients had a mean age of 22.8 years (range, 11-65), and 82.5% were male. Mean time from injury to surgery was 23.5 months (range, 0.5-192), and mean follow-up time was 43.2 months (range, 10-228).
Characteristics of Included Studies a
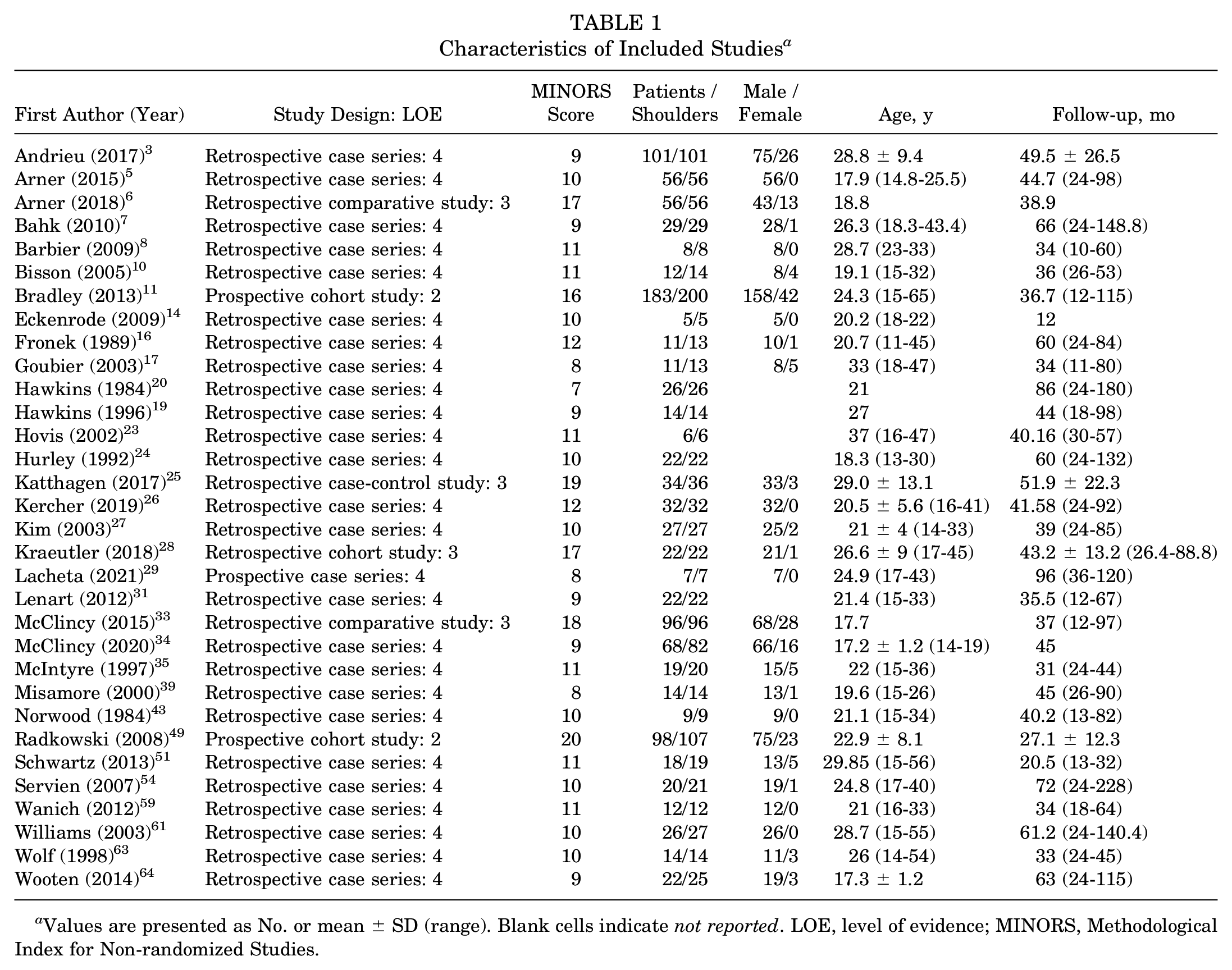
Values are presented as No. or mean ± SD (range). Blank cells indicate not reported. LOE, level of evidence; MINORS, Methodological Index for Non-randomized Studies.
Patient Sport Characteristics
Preoperative level of competition was available for 774 athletes (Table A2, available online): 27 professional, 175 collegiate, 416 high school, 6 amateur, and 122 recreational. An additional 28 athletes were simply described as competitive. In addition, among the 1100 patients, the preoperative type of sport involvement was reported for 735 patients: 338 participated in contact sport (46%; 338/735), and 320 in an overhead or throwing sport (44%; 320/735). The individual sports played are listed in Appendix Table A2 (available online). For our definition of “contact” sports, we noted whether the study described the patients as unspecified contact athletes, as well as if the sport was classified as a contact sport by the commonly cited classification of the American Academy of Pediatrics Committee on Sports Medicine. 2
Surgical Details
While the majority of studies used posterior shoulder instability as the indication for operative management, 5 studies stated that pain in the absence of instability was the indication for 60 patients.3,10,17,26,35 Additionally, 19 studies (882 patients) explicitly stated that they excluded patients with multidirectional instability, and 3 (166 patients) excluded patients with SLAP tears.
Of the 32 studies, 24 (1028 shoulders) had patients who underwent arthroscopic surgical stabilization, and 8 (125 shoulders) examined patients after open surgical stabilization. Surgical details as well as concurrent procedures are described in Table A3 (available online). The most commonly performed arthroscopic procedures were capsulolabral repair/plication (20 studies) and thermal capsulorrhaphy (2 studies). Concurrent procedures were reported by 9 of the 32 studies. The most common procedures in addition to surgical stabilization were rotator cuff debridement (n = 27), subacromial decompression (n = 24), and rotator interval closure (n = 13).
Rehabilitation and Return-to-Sport Protocol
Of the 32 studies, 27 had a postoperative rehabilitation protocol (Table A3, available online). Postoperative immobilization was cited by 25 studies, which ranged from 2 to 8 weeks; however, the majority (14 studies) detailed 4 to 6 weeks of immobilization, as compared with 5 studies with 3 weeks of immobilization. Most studies noted immobilization in neutral or external rotation, as opposed to 8 studies with immobilization in slight abduction, typically 20° to 30°. Seven studies published criteria for return to sport, all of which required the operative shoulder to have complete or near-complete strength and range of motion. For the 3 studies that commented on return-to-sport criteria for throwing athletes, all required patients to be able to throw at full velocity for 2 consecutive weeks without symptoms.11,33,49 Of the 12 studies that reported the time at which athletes were allowed to return to sport, 10 allowed return to full activity at 4 to 6 months.
Return-to-Sport Outcomes
All 32 studies reported on return to sport, and such outcomes were available for 1100 patients who underwent surgical stabilization for posterior shoulder instability (Table 2). Rates of return to sport ranged from 38% to 100%, with a pooled rate of 88% (95% CI, 84%-92%; I2 = 68.7%) (Figure 2). Time to return was cited by 6 studies, with a mean of 7.5 months (range, 3-18 months). Postoperative return to the same level of sport was noted for 934 patients, and the pooled rate was 68% (95% CI, 60%-76%; I2 = 79%) (Figure 3). The pooled rate of return to sport after an arthroscopic procedure (979 patients) was 90% (95% CI, 86%-93%; I2 = 58.3%) and after an open procedure (121 patients) was 80% (95% CI, 62%-95%; I2 = 78.2%). Moreover, the pooled rates of return to preinjury level were 73% (95% CI, 67%-78%; I2 = 58.2%) and 34% (95% CI, 3%-73%; I2 = 90.8%) for arthroscopic and open procedures, respectively. Regarding arthroscopic capsulolabral repair, the pooled rate of return to sport was 89% (95% CI, 85%-93%; I2 = 59.4%), and that to the preinjury level was 73% (95% CI, 68%-79%; I2 = 60.5%). Last, the rate of return to sport after surgical management of traumatic posterior instability was 92% (95% CI, 86%-97%; I2 = 0%) while return to the preinjury level was 76% (95% CI, 64%-86%; I2 = 0%).
Return to Sport and Success of Stabilization a
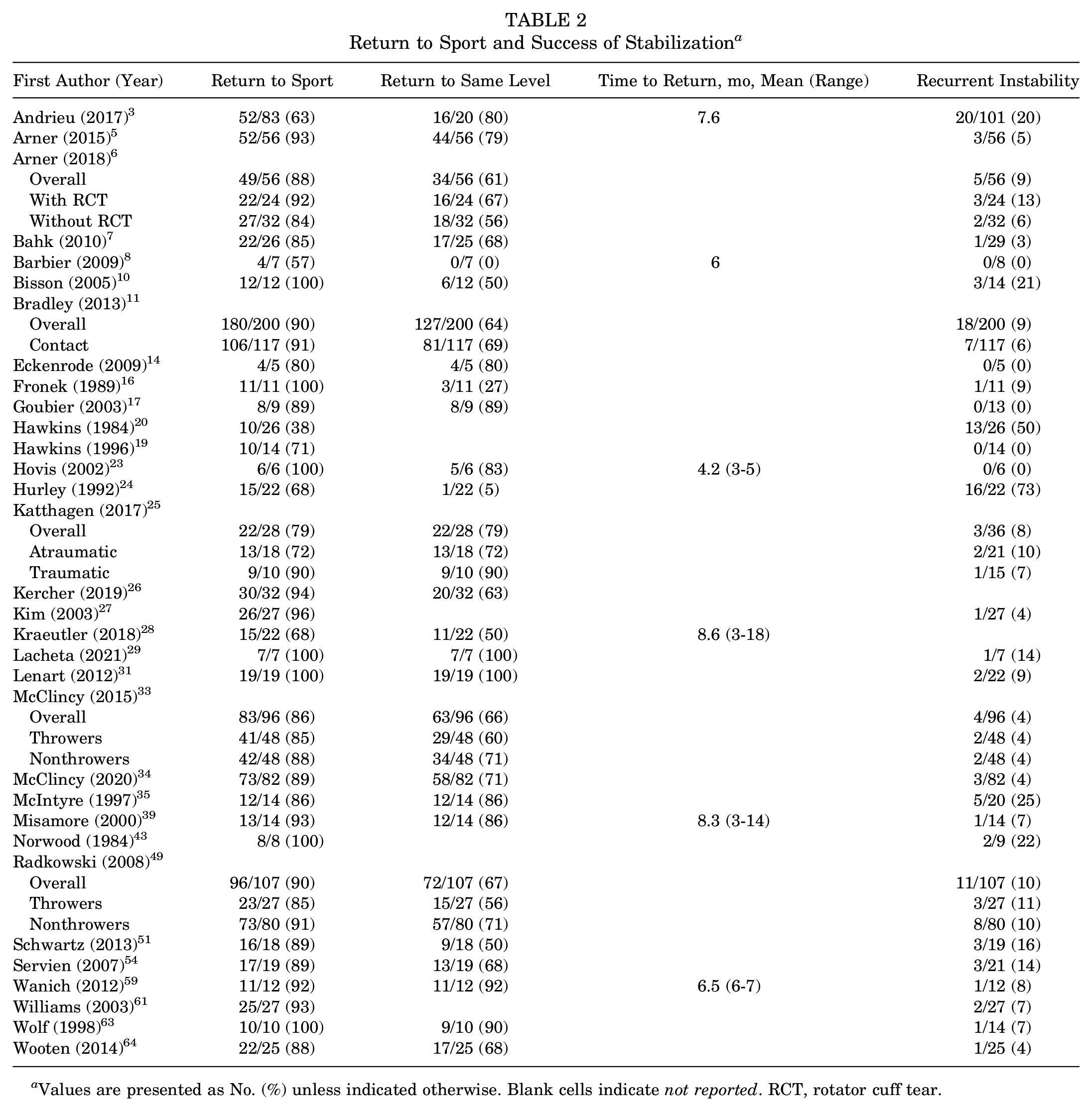
Values are presented as No. (%) unless indicated otherwise. Blank cells indicate not reported. RCT, rotator cuff tear.
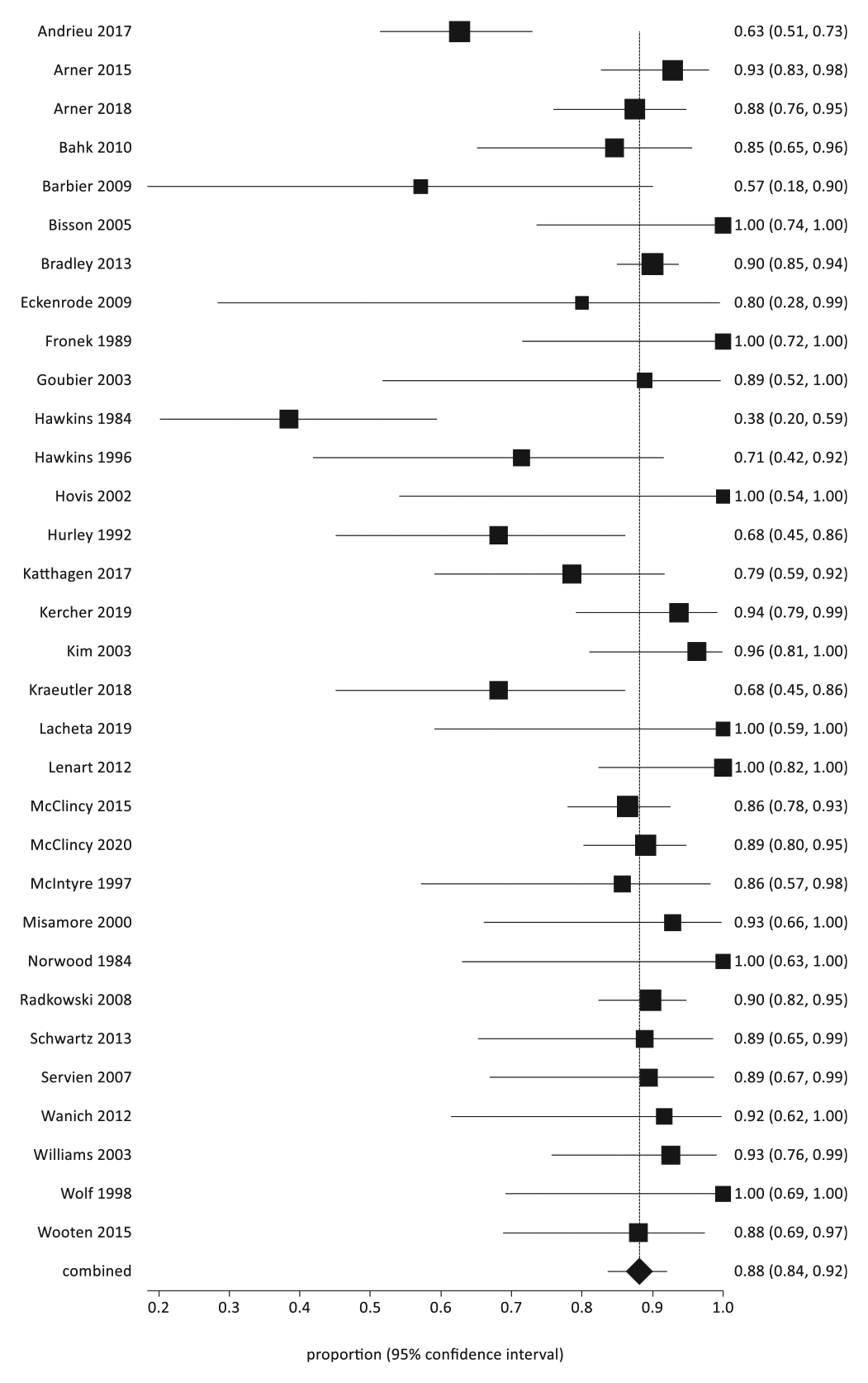
Overall return to sport at any level.
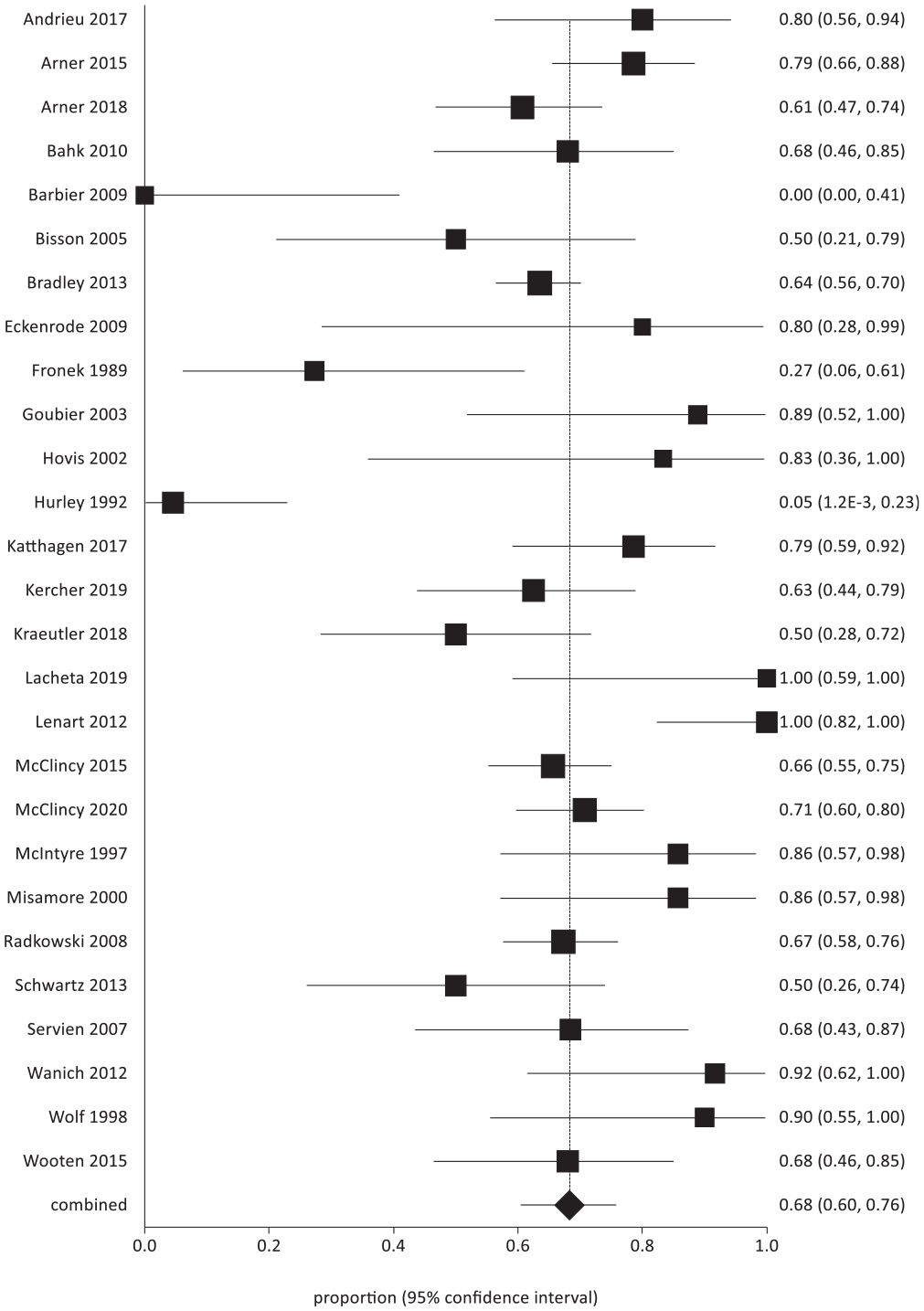
Overall return to sport to the preinjury level.
Various subgroups of athletes were also analyzed when it came to return to sport. In 6 studies, the pooled rate of overall return for contact athletes was 94% (95% CI, 90%-97%; I2 = 0%), with 73% (95% CI, 65%-81%; I2 = 25.9%) returning to their previous levels (Figures 4 and 5). For throwing athletes (6 studies), pooled rates were 88% (95% CI, 83%-92%; I2 = 0%) and 62% (95% CI, 55%-70%; I2 = 15.5%), respectively (Figures 6 and 7). For studies examining football players (3 studies), the pooled rate of return to sport was 94% (95% CI, 88%-98%; I2 = 0%), and for baseball players (2 studies), it was 94% (95% CI, 83%-100%; I2 = not applicable). Three studies compared throwers and nonthrowers, and all 3 found no significant difference in the rate of return to sport.33,34,49
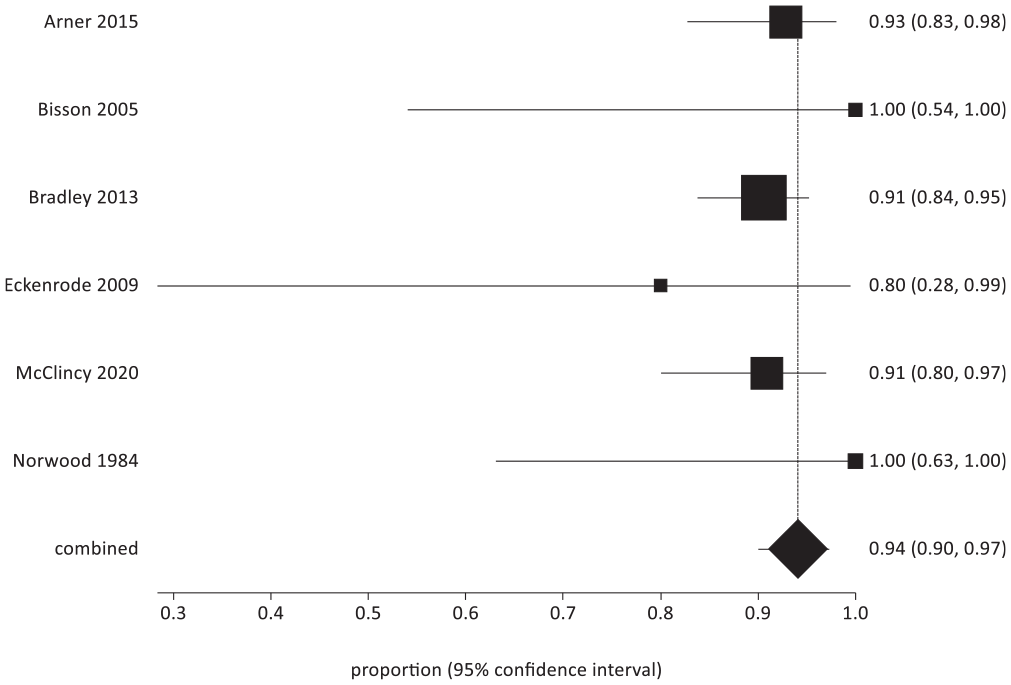
Return to sport at any level for contact athletes.
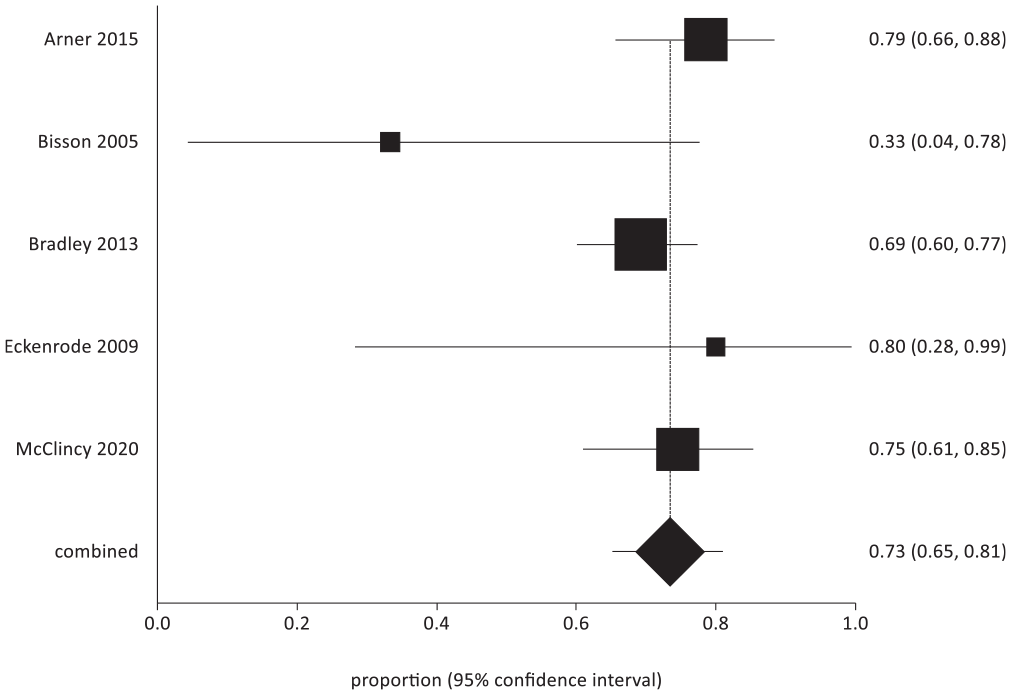
Return to sport at the preinjury level for contact athletes.
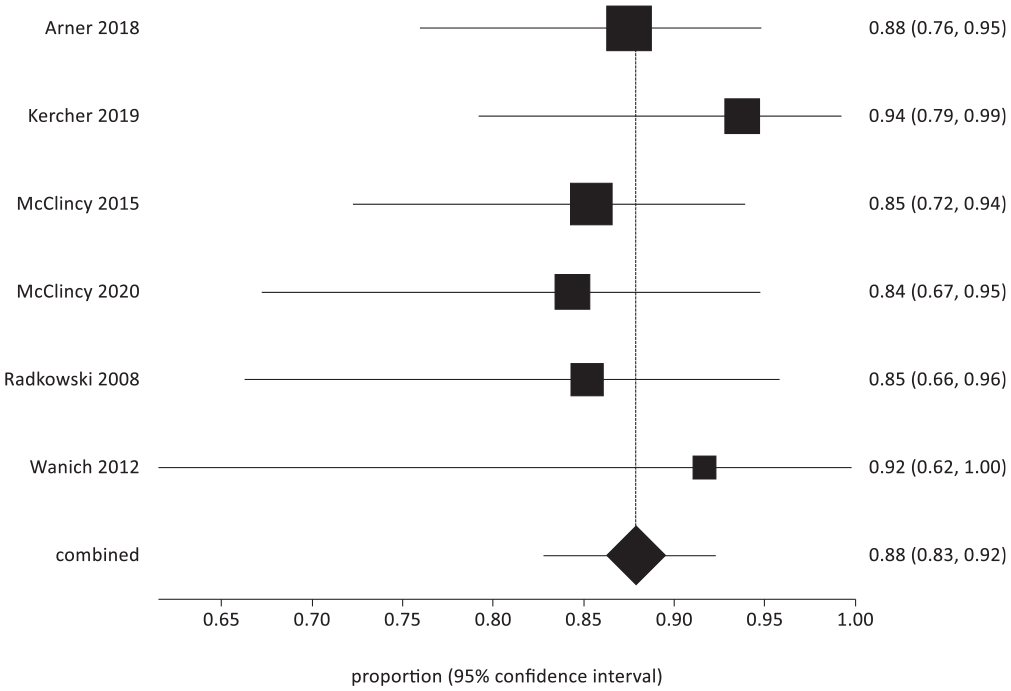
Return to sport at any level for throwing athletes.
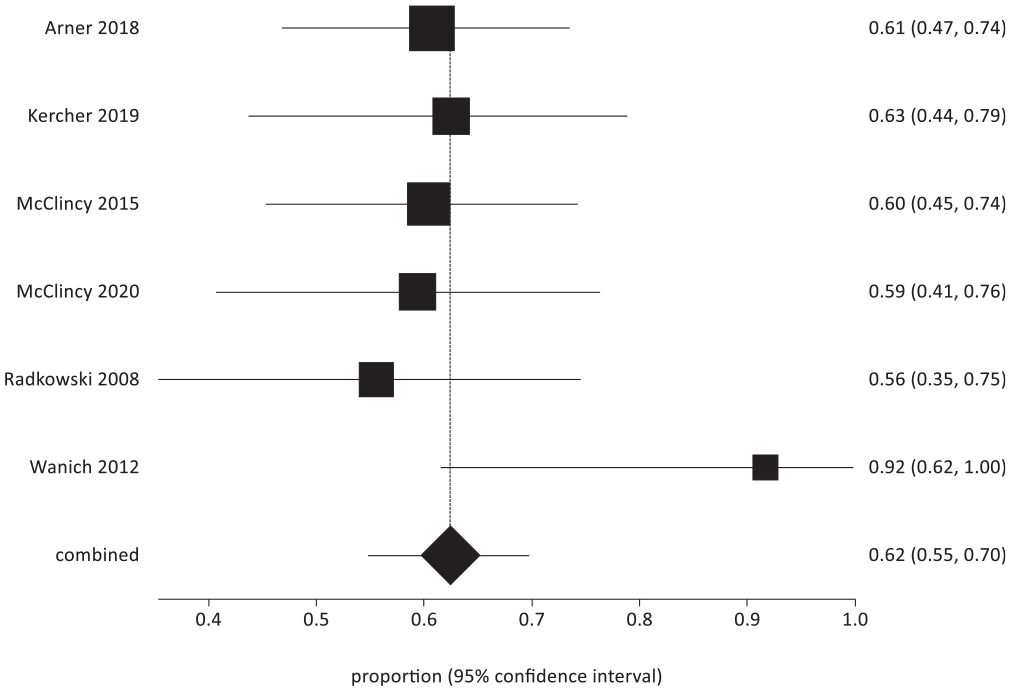
Return to sport at the preinjury level for throwing athletes.
Additionally, in throwers with and without concomitant partial-thickness rotator cuff tears, there was no significant difference in the rate of return to sport. 6 However, Kercher et al 26 did subgroup analysis on pitchers and noted lower rates of return to the same level of play as compared with position players (41% vs 86%; P = .0113). As well, McClincy et al 33 cited a similarly low rate of return to the same level of play for pitchers (50%). Last, Katthagen et al 25 compared traumatic and atraumatic posterior instability and found no significant difference in return to sport postoperatively.
Last, to address heterogeneity in the patient population and study date, other various subgroups were analyzed. In studies with exclusively patients aged ≤40 years, overall return was 86% (95% CI, 79%-91%; I2 = 75.1%), and return to the same level was 69% (95% CI, 58%-79%; I2 = 83%). In the 19 studies that excluded patients with multidirectional instability, overall return was 91% (95% CI, 86%-94%; I2 = 63.4%), and return to the preinjury level was 73% (95% CI, 67%-79%; I2 = 65.5%). Last, when studies published after the year 2000 were examined, the pooled rate of return to sport overall was 89% (95% CI, 85%-92%; I2 = 59.7%) and to the preinjury level was 71% (95% CI, 64%-77%; I2 = 67.2%).
Recurrent Instability and Failures
Postoperative stability was reported for 1099 shoulders. If recurrent instability in the form of dislocation or subluxation was not explicitly stated, shoulders were considered unstable if they had less than good or excellent stability on a subjective scale. Rates of recurrent instability ranged from 0% to 73% (Table 2), with an overall rate of 11% (124/1099). Two studies compared throwers and nonthrowers and found rates of recurrent instability of 4% and 11% for throwers and 4% and 10% for nonthrowers.33,49 Additionally, Bradley et al 11 analyzed a subset of contact athletes who had a 6% rate (7/117) of recurrence, while Arner et al 5 examined only contact athletes for a 5% rate (3/56) of recurrence.
Five studies (541 shoulders)5,11,33,34,49 reported on failures as they relate to suture anchor use, and 4 of 5 found at least a 2-fold increased rate of failure in those patients who received a repair without anchors.11,33,34,49 The 1 additional study had only 2 failures and both involved anchored repairs; however, anchored repairs accounted for 79% of repairs in this study. 5 For the 2 studies using knotless anchors,29,61 the combined failure rate was 9% (3/34), which was the same rate for studies using knotted repairs (85/940).
Pain and Functional Outcomes
Overall, 13 studies (804 patients) reported on pain scores, all utilizing a visual analog scale ranging from 0 to 10. Of these, 11 studies (753 patients) published pre- and postoperative pain scores, and all demonstrated significant improvement (Table 3). Additionally, functional outcome scores were noted by 24 studies, with 16 utilizing multiple outcome scores. The most common functional outcome scores were the American Shoulder and Elbow Surgeons score (14 studies) as well as its function component (5 studies), followed by the Rowe score (4 studies), Constant score (3 studies), and Single Assessment Numeric Evaluation (3 studies). All functional outcome scores showed improvement postoperatively, and functional outcomes by individual study are presented in Table 3.
Pain and Functional Outcomes a
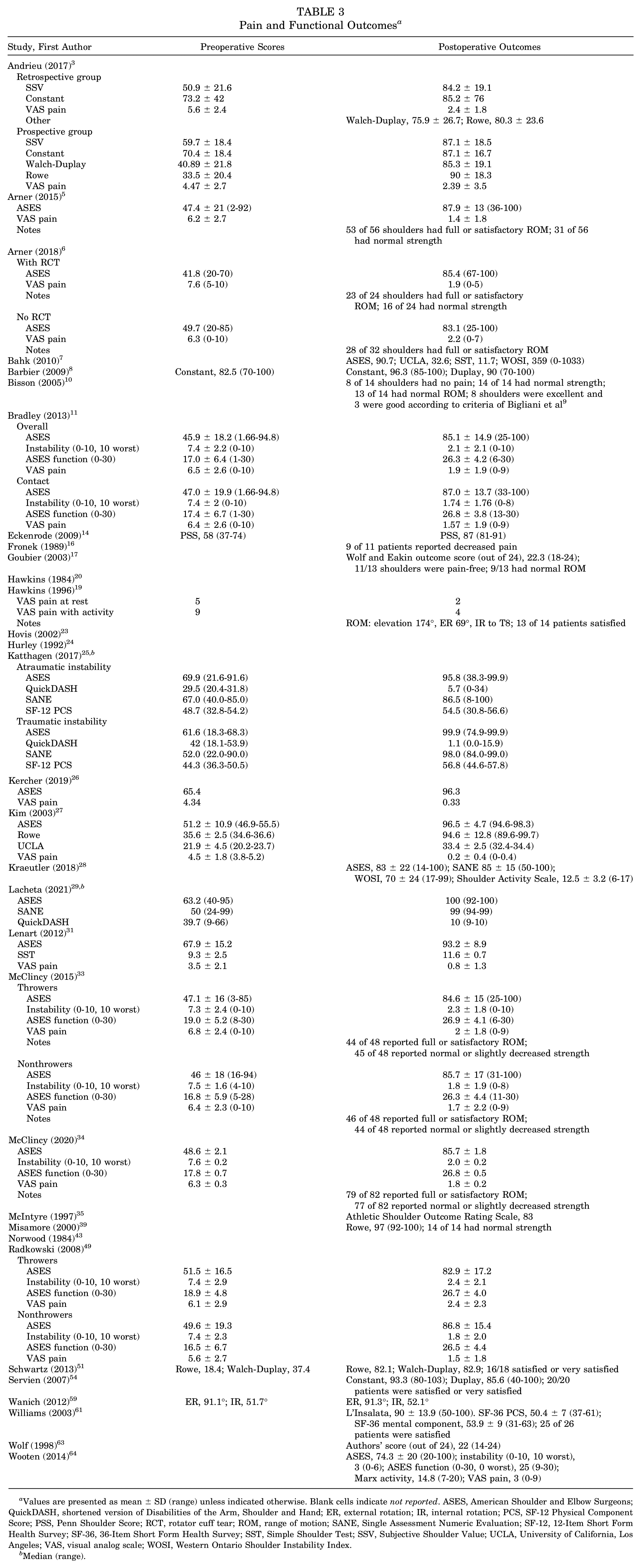
Values are presented as mean ± SD (range) unless indicated otherwise. Blank cells indicate not reported. ASES, American Shoulder and Elbow Surgeons; QuickDASH, shortened version of Disabilities of the Arm, Shoulder and Hand; ER, external rotation; IR, internal rotation; PCS, SF-12 Physical Component Score; PSS, Penn Shoulder Score; RCT, rotator cuff tear; ROM, range of motion; SANE, Single Assessment Numeric Evaluation; SF-12, 12-Item Short Form Health Survey; SF-36, 36-Item Short Form Health Survey; SST, Simple Shoulder Test; SSV, Subjective Shoulder Value; UCLA, University of California, Los Angeles; VAS, visual analog scale; WOSI, Western Ontario Shoulder Instability Index.
Median (range).
Discussion
The primary finding of this review was that there was a high rate of return to sport after surgical management of posterior shoulder instability. Using a meta-analysis of proportions, the pooled rate of return to any level of sport was 88%, while 68% of patients returned to their preinjury levels. Pooled rates for arthroscopic and open procedures were 90% and 80%, respectively; however, pooled rates of return to preinjury levels were 73% and 34%. Additionally, subgroup analysis found high rates of return to sport in contact athletes (94%) and throwing athletes (88%), as well as for those playing baseball (94%) and football (94%), with similar rates in studies comparing throwers and nonthrowers. Last, this review revealed widespread improvement in pain and functional outcome scores after operative management.
These findings are significant in that operative management of posterior shoulder instability resulted in a high rate of return to sport, in addition to significant pain reduction and improvement in functional outcomes. Return to sport is often the primary expectation for those about to undergo arthroscopic shoulder surgery, and a high rate of return to sport is important not only for athletes but for the clinicians considering offering operative management. 60 While the return-to-sport rates in the available literature varied quite widely, from 38% to 100%, this review revealed a more encouraging rate of 88%. This is similar to the rate identified in a previous review by DeLong et al 12 of 92% overall after an arthroscopic procedure, although that study did not employ a meta-analysis of proportions.
An additional finding of this review was that patients undergoing open surgical procedures appeared to have lower return-to-sport rates as compared with those after arthroscopic stabilization—overall (80% vs 90%) and to the preinjury level (34% vs 73%). However, this is potentially due to patients with more complex pathology, such as the presence of significant bone loss, needing an open stabilization procedure. 42 As well, for studies reporting return to the preinjury level after an open procedure, there was a small sample size and high heterogeneity. Nevertheless, these findings suggest that patients undergoing open procedures for posterior shoulder instability are likely to have a relatively low chance of returning to their preinjury levels of sport, which is an important factor for clinicians, patients, and families to consider. Another significant finding with regard to the operative procedure is the effect of the use of suture anchors in arthroscopic repairs. Successful return to sport requires successful stabilization, and of the 5 studies citing failures based on suture anchor use, 4 studies had at least a 2-fold increased rate of failure in those patients who received a capsulolabral repair or plication without anchors.11,33,34,49 This would suggest that the use of suture anchors in arthroscopic capsulolabral repairs may provide less of a postoperative failure risk. Additionally, while similar failure rates occurred between knotted and knotless anchor repairs, only 2 studies used knotless anchors.
Contact athletes represent a high-risk group when it comes to posterior shoulder instability 57 ; however, this review revealed high rates of overall return (94%), as well as return to the preinjury level (73%) when compared with the total population of athletes. Bradley et al 11 reviewed 200 shoulders and compared them with a subset of 117 shoulders of contact athletes and found rates of return that were nearly identical between contact athletes (91%) and the entire study population (90%). However, not all contact athletes share the same risk profile, and those who engage in activities that involve posterior forces to a flexed and adducted arm are at higher risk for failure and inability to continue competition. A review of players drafted into the National Football League revealed that linemen (offensive and defensive), whose position involves repetitive posteriorly directed impacts, were the only position group to demonstrate an association between posterior labral tears and performance metrics. 41 However, despite the increased risk associated with this group of athletes, linemen were also the only group to have significant differences that benefited surgically treated athletes in terms of snaps played when compared to nonsurgically treated ones. So, while it is true that some contact athletes engage in higher-risk activities, they may be the ones who will benefit the most from surgical management.
Owing to repetitive stresses on the capsulolabral complex, the act of overhead throwing places a great deal of strain on the athlete’s shoulder. Despite this, throwing athletes had relatively high rates of return to sport (88% overall; 62% to preinjury level). It should be recognized that these results likely cannot be applied to all throwing athletes, considering that a subgroup analysis of baseball pitchers revealed a 41% to 50% rate of return to preinjury levels.26,33 This suggests that return to preinjury-level sport may be more difficult for those throwing athletes whose sport or position requires high numbers of throwing repetitions and at maximal or near-maximal effort (eg, pitchers, quarterbacks, javelin throwers). For these patients, any reduction in power or accuracy, as well as the inability to perform many repetitions, may prevent return to sport at the same level. Additionally, in our analysis, the throwing shoulder was not isolated, and lower return-to-sport rates may be expected in those who had their throwing shoulders operated on, as this may reflect posterior instability secondary to the throwing motion seen in pitchers. This is supported by data indicating that pitchers are more likely to be affected in their throwing shoulders than all other baseball players. 26
Despite the generally positive return-to-sport rates in this review, just two-thirds of athletes are returning to their sports at a preinjury level. Still, there remain inconsistencies in this reporting. There is still no certain definition of what return to preinjury level means, with studies even acknowledging they rely purely on the athlete’s subjective opinion. 33 As well, additional factors can affect an athlete’s return, of which graduation is often referenced for high school and collegiate athletes.6,14 Other reasons identified as affecting return to sport were fear of reinjury and shifts in priority. 58
While the majority of studies had a rehabilitation protocol, just 22% cited criteria for returning to competition, and only 9% specified return-to-play criteria for throwing athletes. This demonstrates that further research is needed to develop consensus criteria and a return-to-sport protocol for athletes after surgical stabilization for posterior shoulder instability. Additionally, future research in the area of posterior shoulder instability is warranted because of the present paucity of high-level research (level 1 or 2 evidence) available on the subject.
The strength of this systematic review is that it is a comprehensive analysis of the available literature regarding return to sport after surgical management of posterior shoulder instability. It employed rigorous methodology and utilized a meta-analysis of proportions to determine pooled rates of return to sport. Furthermore, it offers insight into the postoperative functional outcomes of these patients. Finally, the information that this review provides on overall return to sport, as well as preinjury return and rates for various subgroups of patients, allows clinicians to have meaningful discussions with patients regarding their expectations and decision to move forward with surgical management.
The primary limitations of this review stem from the quality of available evidence investigating return to sport after surgical management of posterior shoulder instability. There were no randomized studies, and the majority of studies were case series (level 4 evidence), which were noncomparative and utilized primarily retrospective data collection. This evidence is potentially prone to selection bias, as well as bias relating to data reporting and the assessment of outcomes. Furthermore, there was significant heterogeneity in patients’ age, characteristics, and operative procedures; however, subgroup analysis found similar rates of return to sport throughout. Last, there was significant statistical heterogeneity in return-to-sport rates across studies, although the rates were combined using a random effects model in a meta-analysis of proportions to account for this heterogeneity.
Conclusion
Surgical management of posterior shoulder instability resulted in a high rate of return to sport, as well as significant pain reduction and functional improvement in most patients. Similarly high rates of return to sport were identified among those considered to be at higher risk, including overhead throwing and contact athletes. However, just two-thirds of athletes can return to their preinjury levels of sport.
Supplemental Material
sj-pdf-1-ajs-10.1177_03635465211011161 – Supplemental material for Return to Sport After Surgical Management of Posterior Shoulder Instability: A Systematic Review and Meta-analysis
Supplemental material, sj-pdf-1-ajs-10.1177_03635465211011161 for Return to Sport After Surgical Management of Posterior Shoulder Instability: A Systematic Review and Meta-analysis by Kyle Gouveia, Jeffrey Kay, Muzammil Memon, Nicole Simunovic, Asheesh Bedi and Olufemi R. Ayeni in The American Journal of Sports Medicine
Footnotes
Submitted August 1, 2020; accepted December 8, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: A.B. has received royalties and consulting fees from Arthrex and Smith & Nephew, consulting fees from Flexion Therapeutics, and hospitality payments from GE Healthcare and Synthes GMBH. O.R.A. has received speaking fees from ConMed. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
An online CME course associated with this article is available for 1 AMA PRA Category 1 Credit™ at ![]() . In accordance with the standards of the Accreditation Council for Continuing Medical Education (ACCME), it is the policy of The American Orthopaedic Society for Sports Medicine that authors, editors, and planners disclose to the learners all financial relationships during the past 12 months with any commercial interest (A ‘commercial interest’ is any entity producing, marketing, re-selling, or distributing health care goods or services consumed by, or used on, patients). Any and all disclosures are provided in the online journal CME area which is provided to all participants before they actually take the CME activity. In accordance with AOSSM policy, authors, editors, and planners’ participation in this educational activity will be predicated upon timely submission and review of AOSSM disclosure. Noncompliance will result in an author/editor or planner to be stricken from participating in this CME activity.
. In accordance with the standards of the Accreditation Council for Continuing Medical Education (ACCME), it is the policy of The American Orthopaedic Society for Sports Medicine that authors, editors, and planners disclose to the learners all financial relationships during the past 12 months with any commercial interest (A ‘commercial interest’ is any entity producing, marketing, re-selling, or distributing health care goods or services consumed by, or used on, patients). Any and all disclosures are provided in the online journal CME area which is provided to all participants before they actually take the CME activity. In accordance with AOSSM policy, authors, editors, and planners’ participation in this educational activity will be predicated upon timely submission and review of AOSSM disclosure. Noncompliance will result in an author/editor or planner to be stricken from participating in this CME activity.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.