
Abstract
Background:
The all-inside anterior cruciate ligament reconstruction (ACLR) procedure uses a single hamstring tendon folded twice and secured to itself to form a 4-stranded graft. There are several possible configurations for preparing the graft.
Purpose:
To investigate the biomechanical properties of a new graft preparation technique in comparison with 2 commonly used configurations.
Study Design:
Controlled laboratory study.
Methods:
Five porcine flexor tendons were prepared into the test graft configuration: side-to-side fixation with a backup fixation at the button loop (graft M). The test configuration was compared with the results of a previous study that included grafts with simple interrupted sutures (graft A; n = 5) and end-to-end fixation (graft C; n = 5). All grafts were subjected to the same mechanical testing protocol to determine the mean failure load, stiffness, rate of elongation, and total elongation during both cyclic loading and pull to failure. Differences between groups were evaluated.
Results:
Graft A had a significantly lower failure load (637 ± 99 N) compared with graft M (883 ± 66 N; P = .002) and graft C (846 ± 26 N; P = .002). Graft A also had significantly lower stiffness (166 ± 12 N/mm) compared with graft M (215 ± 8 N/mm; P < .001) and graft C (212 ± 11 N/mm; P < .001). Graft C had a significantly lower elongation during cyclic loading (3.42 ± 0.24 mm) compared with graft M (4.37 ± 0.74 mm; P = .026) and graft A (4.90 ± 0.88 mm; P = .006). The unsecured fixation was the weakest graft, with the lowest failure load and stiffness. The new side-to-side configuration and end-to-end configuration were equally strong.
Conclusion:
The new side-to-side configuration was not biomechanically superior to the end-to-end configuration; however, they were both stronger than unsecured fixation.
Clinical Relevance:
As the all-inside ACLR is gaining popularity, this study provides surgeons with a new method of preparing grafts and evaluates the method with respect to currently used configurations.
The all-inside anterior cruciate ligament (ACL) reconstruction (ACLR) technique is becoming increasingly utilized as a means of treating patients with ACL injuries. In this technique, closed socket tunnels are drilled in a retrograde fashion. Adjustable length looped cortical button devices are used for fixation of the graft on the tibial and femoral ends. This technique allows for potential benefits, including gracilis tendon preservation, reduced bone removal, decreased graft length requirements, smaller skin incisions, and less postoperative pain. 3,13 Several outcome studies have been published that suggest comparable outcomes with a standard ACLR. 12,18 The graft for the all-inside technique is typically constructed using the semitendinosus tendon due to its favorable biomechanical properties. 1,7,8,11,15
In this technique, the quadrupled graft is formed into a closed loop by securing the graft to itself with a variety of suture techniques. In a previous study, we investigated the biomechanical properties of 5 different graft fixation techniques, finding that grafts with end-to-end fixation and without secondary fixation have superior biomechanical properties. 2 Another fixation technique, known as the Sommerfeldt configuration, is used clinically by our group; in this method, the surgeon secures the 2 free ends of the graft using a side-to-side fixation and adds an additional backup fixation at the button loop. It is unknown whether this additional backup fixation improves the biomechanical properties of the graft, as this graft-preparation technique was not evaluated in our previous study. This extra step in the graft-preparation process does add time for the surgeon; therefore, delineating whether this configuration has superior biomechanical properties is prudent.
The purpose of this study was to evaluate the biomechanical properties of the all-inside ACL graft preparation technique of an additional suture configuration in comparison with end-to-end fixation without secondary fixation and unsecured fixation. We hypothesized that the new side-to-side fixation with an additional backup fixation at the button loop would have superior biomechanical properties compared with the end-to-end fixation and unsecured fixation methods.
Methods
Three groups of 5 porcine digital flexor tendons 5,6 were used for mechanical testing. Overall, this was the test group (n = 5) along with 2 groups (n = 5 per group) we previously tested. 2 The tendons were not frozen prior to graft preparation. The specimens were cut to 200 mm to produce a 4-stranded graft of approximately 50 mm. 4,10 The 50-mm grafts were trimmed to fit through a 12 mm-diameter tube. Grafts were stored at –20°C and thawed at room temperature for 1 hour before testing.
Graft Preparation
Grafts were prepared in the same manner as previously described 2 (Figure 1). Suture loops and buttons (Arthrex Tightrope RT; Arthrex) were used on both the tibial and femoral ends to suspend the grafts. The graft preparation is briefly summarized here.

Illustration of graft preparation technique. Graft A, unsecured fixation; Graft C, secured end-to-end fixation; and Graft M, secured side-to-side fixation with backup fixation to button (button is at bottom of figure).
Graft A (Unsecured Fixation). The tendon was folded over the tibial suture loop symmetrically, and both free ends were doubled and passed through the femoral suture loop in alternating directions, yielding a quadrupled graft. The free ends of the graft were passed to the same side of the loop so that they could be stitched together with No. 2 FiberWire (Arthrex). Next, the 4 strands of the graft were secured with 4 No. 2 Fiberwire interrupted sutures to create the final quadrupled loop structure. Each stitch was passed through all 4 strands of the graft, and the suture-free limb was wrapped around the entire graft configuration to form a self-reinforcing suture noose. 2,9
Graft C (Secured End-to-End Fixation). The tendon was folded over the tibial suture loop symmetrically, and both free ends were doubled and passed through the femoral suture loop in alternating directions, yielding a quadrupled graft. To achieve end-to-end fixation, 1 free end of the graft was passed through the tibial loop. A single No. 2 FiberWire was then used to secure the 2 ends of the graft together. The ends were whipstitched over a length of 20 mm on each limb of the graft. The needle was then removed, and 1 end of the suture was passed through the tibial suture loop and tied to the other suture end. The 4 strands of the graft were then secured with 4 No. 2 FiberWire interrupted sutures as in Graft A. 2,9,14
Graft M (Secured Side-to-Side Fixation With Back-up Fixation to Button). The tendon was folded over the tibial suture loop symmetrically, and both free ends were doubled and passed through the femoral suture loop in the same direction, yielding a quadrupled graft. The free ends of the graft were whipstitched together with 3 throws up and 3 throws down in a side-to-side manner with a No. 2 FiberWire over a length of 20 mm. The needle was removed, and 1 end of these side-to-side sutures was passed through the suture loop on the tibial side and tied to the other suture. The 4 strands of the graft were then secured with 2 No. 2 FiberWire interrupted sutures on the femoral side. On the tibial side, another No. 2 FiberWire was used to whipstitch all 4 tendon strands together with 3 throws up and 3 throws down. This suture was then tied as backup fixation over the tibial button.
Mechanical Testing
The mechanical testing protocol followed our previous work. 2 A Bose Electroforce 3510 mechanical testing machine (TA Instruments) was used to apply tensile loading to each graft. The grafts were fixed to the machine with the Tightrope Arthrex RT and a button loop and aligned with the loading axis (Figure 2). A preload of 20 N was applied at a rate of 1 N/s. Grafts were then held at a pretension of 20 N for 5 minutes. Cyclic preconditioning was applied from 20 N to 50 N at 0.1 Hz for 10 cycles followed by a cyclic loading phase from 50 N to 250 N at 1 Hz for 500 cycles. Finally, the grafts were pulled to failure at a rate of 20 mm/min.

Mechanical testing setup with graft M2 fixed in the machine.
During the cyclic loading phase, the elongation rate (mm/s) was calculated as the slope of a portion of the linear section of the graph of the displacement as a function of time. The elongation (mm) during the cyclic loading was calculated as the difference between the last and first trough of the cyclic loading phase. The elongation (mm) during the pull to failure was calculated as the difference between the displacement at the failure load and the displacement at the last trough of the cyclic loading. The total elongation (mm) was recorded as well as the combined elongation of the cyclic loading and the pull to failure. The stiffness (N/mm) was determined as the initial slope of the linear portion of the graph of the displacement as a function of load. The failure load (N) as well as the mode of failure were recorded for each specimen. The mode of failure was either a tendon rupture or button loop rupture.
Statistical Analysis
Descriptive statistics (mean ± SD) were recorded for each of the 5 variables. Differences in biomechanical properties were evaluated using 1-way analysis of variance (ANOVA). The relevance of the differences was evaluated using post hoc t tests, with the Benjamini-Hochberg procedure for multiple comparisons. Statistical significance was set at P < .05.
Results
Table 1 shows the biomechanical properties of each graft type. Most properties were found to be significant (ultimate failure load, P < .001; stiffness, P < .001; elongation rate, P = .155; elongation during cyclic loading, P = .014; elongation during pull to failure, P = .065; and total elongation, P = .155; ANOVA). To identify the differences between the preparation methods, all groups were compared using post hoc t tests. Figure 3 shows the results of the post hoc test comparing preparation methods in all biomechanical properties compared.
Biomechanical Properties of the Graft Types a

a Data are reported as mean ± SD.
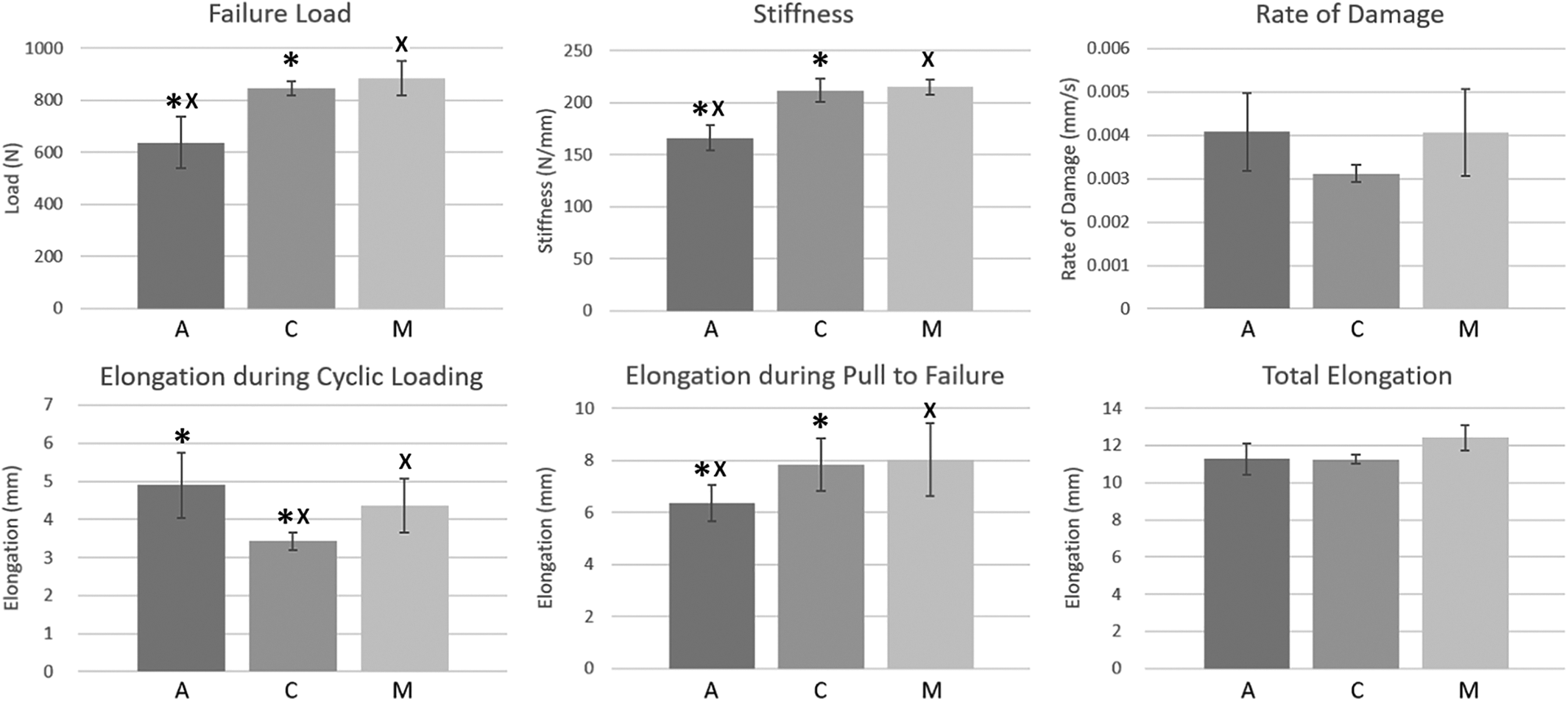
Biomechanical properties for each group. Symbols (*, x) indicate statistically significant differences between the groups (P < .05, post hoc test). A, unsecured graft; C, secured end-to-end fixation; M, secured side-to-side fixation with backup fixation to button.
Failure Load
Graft M (Sommerfeldt configuration) had the highest mean failure load (883 N). Graft C (end-to-end fixation) had the second highest mean failure load (846 N). Graft A (unsecured fixation) had the lowest mean failure load of the grafts (637 N). Graft A had a significantly lower mean failure load than both graft M (P = .002) and graft C (P = .002). There was no statistically significant difference between grafts C and M (P = .282).
Stiffness
Graft M had the highest mean stiffness of the 3 grafts (215 N/mm). Graft C had the second highest mean stiffness (212 N/mm). Graft A had the lowest mean stiffness of the grafts (166 N/mm). Graft A had a significantly lower mean stiffness than graft M (P < .001) as well as graft C (P < .001). Neither graft C nor graft M had any statistically significant differences (P = .590).
Elongation Rate During Cyclic Loading
Graft C had the lowest mean rate of damage (0.0031 mm/s) of the 3 grafts. Graft M and graft A had the same rate of damage (0.0041 m/s). There were no statistically significant differences between any of the graft preparation techniques (P = .155; ANOVA)
Elongation During Cyclic Loading
Graft C had the lowest mean elongation during the cyclic loading phase (3.42 mm). Graft M had the second lowest mean elongation during the cyclic loading (4.37 mm). Graft A had the highest mean elongation during the cyclic loading out of the grafts (4.90 mm). Graft C had a significantly lower elongation during cyclic loading compared with graft M (P = .026) and compared with graft A (P = .006). The were no statistically significant differences between grafts M and A (P = .322).
Elongation During Pull to Failure
Graft M had the highest mean elongation during the pull to failure phase (8.04 mm). Graft C had the second highest mean elongation during the pull to failure (7.82 mm). Graft A had the lowest mean elongation during the pull to failure out of the grafts (6.37 mm). There were no statistically significant differences between any of the graft preparation techniques (P = .065; ANOVA)
Total Elongation
Graft C had the lowest mean combined elongation (11.2 mm). Graft A had the second lowest mean combined elongation (11.3 mm). Graft M had the highest mean combined elongation out of the grafts (12.4 mm). There were no statistically significant differences between any of the graft preparation techniques (P = .155; ANOVA).
Mode of Failure
The mechanism of failure for each graft was recorded as either a tendon suture tear (Figure 4A) or a button loop suture tear (Figure 4B). All grafts A (n = 5) failed by a tear at the tendon suture. All grafts C (n = 5) and grafts M (n = 5) failed by a tear at the button loop suture.
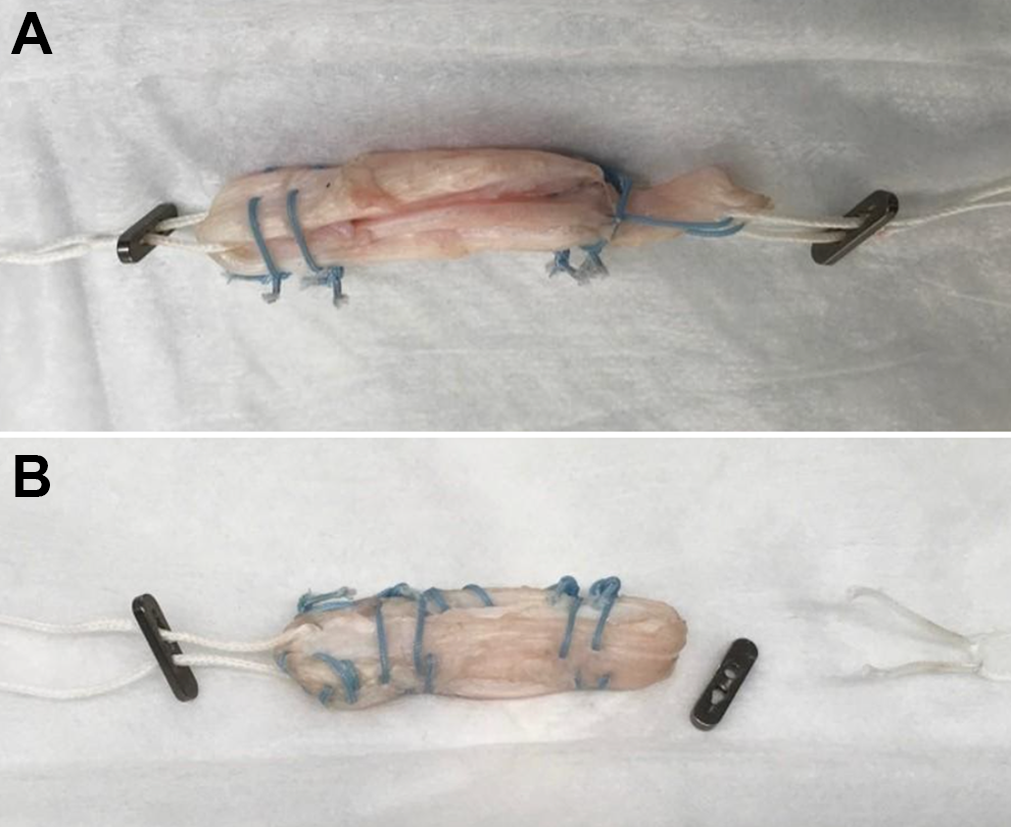
(A) Graft A5 classified as a tendon suture tear after the pull to failure. (B) Graft C4 classified as a button suture tear after the pull to failure.
Discussion
This study shows a biomechanical analysis of a new graft preparation technique and 2 older preparation techniques for the all-inside ACLR procedure. The most important finding of this study is that the new side-to-side fixation with an additional backup fixation is not biomechanically favorable to the end-to-end fixation as there is no significant difference between the 2 in either ultimate failure load, stiffness, or rate of damage. Another important finding is that the end-to-end fixation as well as the side-to-side fixation with the backup fixation both have more biomechanically favorable properties than the unsecured fixation method, which is the current clinical standard.
Within the medical community, there are still doubts regarding the performance of a graft suspended by 2 buttons, regardless of the theoretical advantages the procedure provides. The mean failure loads determined in this study ranged from 637 N to 883 N. These are consistent with failure loads reported by Pailhé et al 11 (mean ± SD, 630.82 ± 239.15 N; range, 408.13-1123.44 N). All these values are on the lower end of the range reported for bovine tendon and porcine tendon grafts 2,5,11,16 and the native ACL (739-2300 N). 17 For quadrupled bovine tendon grafts, failure loads between 767 N and 1097 N were reported by Vertullo et al. 16 The mean stiffnesses determined in this study ranged from 166 N/mm to 215 N/mm, which is consistent with literature on native ACLs, 16 porcine and bovine tendon grafts, 5,16 and grafts prepared for typical ACLR. 5,11
The unsecured fixation utilizing only interrupted sutures to hold the 4 graft limbs together is the currently recommended method of practice. In our findings, we determined that it has the poorest mechanical properties of the 3 grafts tested in this study. The unsecured fixation (graft A) had the lowest failure loads, stiffness, and elongation during the pull to failure. Based on our results, we would recommend to the manufacturer company that it revise its current standard and encourage surgeons to make use of other preparation techniques than the unsecured fixation when preparing quadrupled hamstring tendon graft for all-inside ACLR procedures.
The side-to-side fixation with the additional backup fixation seems to have equal biomechanical properties as the end-to-end fixation method. The 2 preparation techniques performed in the same fashion, with no difference in ultimate failure loads, stiffness, rate of damage, elongation during the pull to failure, or total elongation. The only significant difference between the 2 groups was in the elongation during the cyclic loading, where the end-to-end fixation had a significantly lower elongation. While their mechanical properties are equal, the new side-to-side fixation method requires an additional step during preparation to make the backup fixation. This additional step allows for more room for error in preparation, which could make the graft less reproducible. It was also observed that the end-to-end grafts had lower standard deviations in the ultimate failure load, rate of damage, and elongations. This suggests that end-to-end fixation produces more consistent results; however, this was not investigated in this study.
The hypothesis of the study, that the new side-to-side fixation with a backup fixation would be biomechanically favorable to unsecured fixation and end-to-end fixation, was partially disproven. While the new preparation method was biomechanically favorable to unsecured fixation, it was not favorable to end-to-end fixation as they were equal in strength. Side-to-side fixation with the additional sutures had a higher ultimate load, a higher stiffness, and a higher elongation during the pull to failure than the unsecured fixation. The end-to-end fixation was equal to the new procedure in terms of failure load, stiffness, rate of damage, total elongation, and elongation during the pull to failure, but it did have a lower elongation during the cyclic loading.
It is suspected that the weak point of the grafts used in ACLRs lies at the interface of the 4 limbs of the hamstring tendon. In recent biomedical studies, this has been confirmed.
16
However, we suggest that the weak point of the graft is dependent on the preparation technique used. The weak point of the unsecured fixation lies somewhere at the interface between the button loop sutures and the graft, as all samples failed at the tendon suture with the button loop intact. In the end-to-end fixation, all samples failed by a suture rupture, which suggests that the main sutures and the graft are stronger than the button loop sutures. Side-to-side fixation with the backup fixation at the button loop also failed entirely by the button suture tearing, which also suggests that the graft itself was stronger than the adjustable button loop. The most favorable
The strength of this study is that it confirms the results reported by our previous work, 2 which suggests unsecured fixation as recommended by the manufacturer is biomechanically inferior to other graft-preparation techniques. In addition, we also introduced the Sommerfeldt fixation method of graft preparation and demonstrated that it is superior to the current unsecured fixation method.
The study has several limitations to note. This is a laboratory design, and while it gives us an idea as to which one of these grafts will perform best, we are not sure how they will perform in vivo. Future work may include the assessment of patients who have undergone all-inside ACLR to determine whether graft biomechanical properties translate into failure rates or clinical outcomes. We did see some trends in the data; however, due to the small sample size, limited interpretation of these trends could be made. With a larger sample size, it is possible that these trends could become statistically significant.
Conclusion
This study shows that grafts prepared with the manufacturer-recommended unsecured fixation method demonstrate inferior biomechanical properties to grafts prepared with end-to-end fixation or the Sommerfeldt side-to-side fixation with backup fixation. Further studies are required to evaluate how these graft-preparation methods perform clinically in vivo.
Footnotes
Final revision submitted October 17, 2020; accepted December 14, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: Support for this study was received from the Edmonton Civic Employees Charitable Fund. The adjustable button-loop devices used were contributed by Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was waived by the University of Alberta (study No. RES0044360).