
Abstract
Background:
The all-inside anterior cruciate ligament (ACL) reconstruction technique involves a graft with 2 adjustable loop devices at each end of a closed loop graft, made from folded tendon(s) with cerclage sutures along its length to enhance strength. There is no consensus on the optimal number of cerclage sutures, and this study evaluates their effect on graft strength.
Purpose:
To establish the effect of the number of cerclage sutures on graft strength.
Study Design:
Controlled laboratory study.
Methods:
A controlled cadaveric study of 27 graft specimens was conducted, with specimens standardized to 60 mm in length and 10 mm in diameter and divided into 3 groups: 2-cerclage, 3-cerclage, and 4-cerclage. They were tested using an Instron machine, and data on stiffness, ultimate load to failure (uLTF), and mode of failure were recorded.
Results:
The 3- and 4-cerclage groups showed no significant difference in stiffness (P = .95) and uLTF (P = .81), but both were significantly stiffer with higher uLTF than the 2-cerclage group (3-cerclage, P = .002; 4-cerclage, P = .005). The double-tendon 3-cerclage specimens were significantly stiffer (P = .014) than single-tendon 3-cerclage specimens, but this was not seen in the 4- and 2-cerclage groups. No significant difference in mode of failure was found across the groups.
Conclusion:
A double-tendon 3-cerclage graft matches the stiffness and uLTF of a 4-cerclage graft for diameters ≥10 mm, whereas a 2-cerclage graft appears suboptimal relative to a 3- or 4-cerclage graft. This finding adds to the current literature on all-inside ACL graft techniques.
Clinical Relevance:
The number of cerclages used in ACL graft preparation may play an important role in optimizing graft tension and stiffness. This potentially contributes to reduction of reinjury risk and a safe return to sports.
Keywords
Anterior cruciate ligament (ACL) injuries are common, especially in athletes and active individuals. 13 The ACL plays a critical role in maintaining knee stability and a rupture results in significant functional impairment as well as increased risk of posttraumatic osteoarthritis if left untreated. 8 Surgical reconstruction remains the gold standard with the development of various techniques over the years. 4
The all-inside ACL reconstruction technique has gained popularity in recent years, as it offers the advantages of bone preservation, 28 reduced postoperative pain, lower risk of tunnel collision in multiligament reconstruction, and optimization of graft tensioning.2,5,17 An additional benefit is graft preservation, as the smaller and shorter tibial and femoral sockets allow an adequate graft size to be achieved using a single tendon.14,24,30 One key aspect of a favorable outcome is adequate graft strength and the use of a shorter graft with a bigger diameter, which increases the graft tensile strength. 3 Besides graft diameter, 7 cerclage sutures placed at intervals along the graft enhance its strength and stiffness. However, to our knowledge, there is limited literature correlating the number of cerclages and graft strength. In biomechanical studies, Rovere et al 21 used 2 cerclages, Vertullo et al 23 used 3 cerclages, and Haber et al, 10 Bowes et al, 6 and Wicks et al 25 used 4 cerclages. Different cerclage techniques were used as well. The current study aims to establish the effect of the number of cerclage sutures on graft strength.
Methods
Five fresh-frozen human cadaveric lower limb specimens (4 right; 1 left) from 4 donors (2 male; 2 female) were used. The cadavers were stored at –40°C to –30°C before testing and thawed for 48 hours to room temperature. The donors had a mean age at death of 77.1 ± 13.8 years (range, 59-92 years) and mean body mass index of 23.7 ± 3.4 kg/m2 (range, 19-28 kg/m2). There were no obvious wounds or injuries noted in the specimens.
Cadaveric Tendon Harvesting
This was performed in the laboratory at the authors’ institution (Changi General Hospital, Singapore). Different muscles were identified and harvested—namely, semitendinosus, quadriceps, tendon Achilles, tibialis anterior, tibialis posterior, flexor hallucis longus, extensor digitorum longus, peroneal longus, and peroneal brevis. Each tendon was stripped from its muscle with a Cobb elevator (Carnegie Surgical).
Graft Preparation and Preservation
Each tendon was quadruple-folded onto 2 adjustable loop devices (ALDs; Ultrabutton; Smith & Nephew) with the free ends stitched together with a No. 2-0 Ultrabraid suture (Smith & Nephew) to create a continuous loop (Figure 1). In the current study, a graft diameter of 10 mm and a length of 60 mm was standardized for all specimens. When the quadrupled single-tendon graft exceeded 10 mm, it was trimmed down to achieve a 10-mm diameter. When the quadrupled single-tendon graft diameter was <10 mm, a second quadrupled tendon was added and placed adjacent to the first, with no overlap on the first tendon to achieve the desired 10-mm diameter (Figure 2). Each specimen was tensioned on the graft board after the free ends were stitched together. After the application of a cerclage suture, the graft was retensioned. This process was repeated with each cerclage application from one end of the graft to the other. A total of 27 specimens were prepared. Each specimen was tensioned on the graft board after the free ends were stitched together. After the application of a cerclage suture, the graft was retensioned. This process was repeated with each cerclage application from one end of the graft to the other.

Schematic sagittal diagram of tendon ends stitched together to form a continuous loop and moved onto an adjustable loop device.
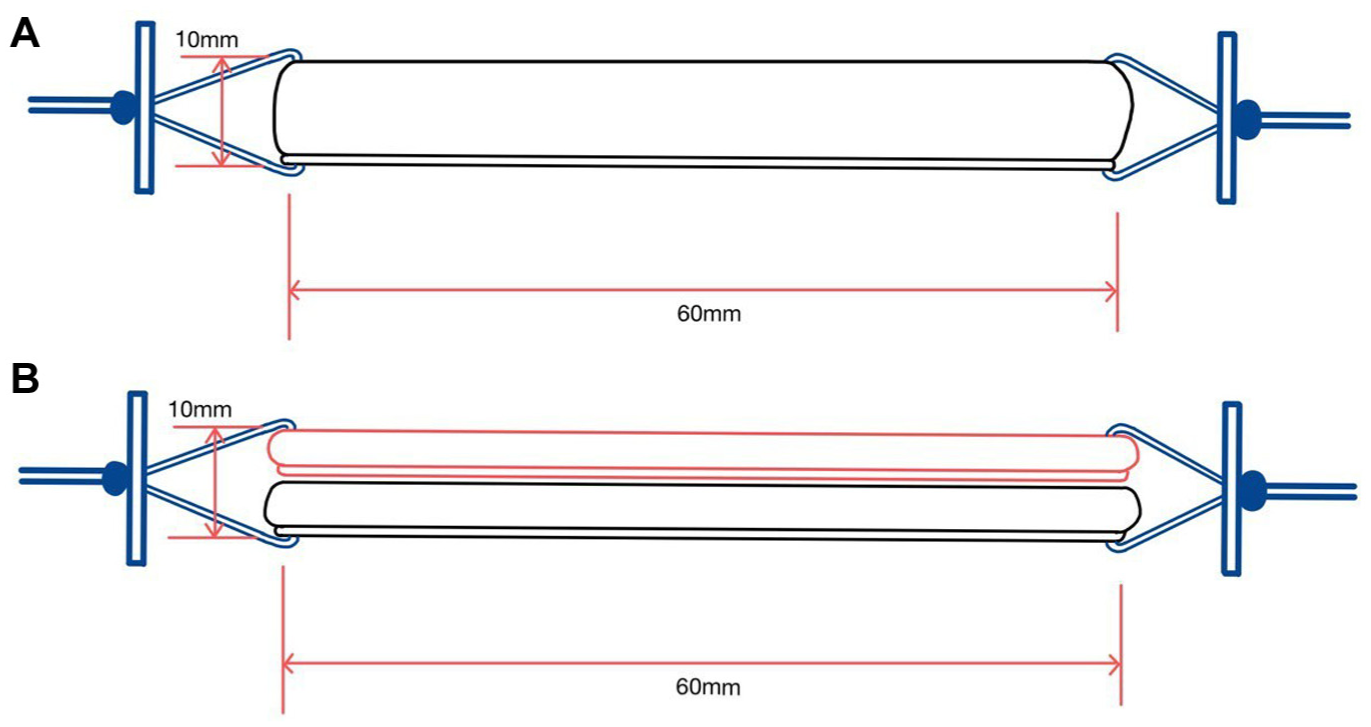
Schematic coronal diagram of (A) single quadrupled tendon vs (B) double quadrupled tendon, with second tendon placed alongside the first tendon with no overlap, to achieve the standardized 10-mm diameter.
The specimens are divided into 3 groups: a 2-cerclage group (Figure 3A), 3-cerclage group (Figure 3B), and 4-cerclage group (Figure 3C). In the 2-cerclage group, the cerclages were located at 20-mm intervals on the graft. In the 3-cerclage group, the cerclages were placed at 15-mm intervals. In the 4-cerclage group, the cerclages were located at 10-mm and 20-mm intervals from each end of the graft. These intervals were marked by ink and No. 2 Ultrabraid (Smith & Nephew) were used for cerclage. The following method was utilized for each cerclage: the suture was passed between the 2 innermost graft strands at each marking on the graft. It was then threaded through as many graft strands as possible, with 2 passes perpendicular to the graft's longitudinal axis. This was followed by tying the suture around the graft circumference 3 times while maintaining tension. The suture was then passed again between the 2 innermost graft strands, from the side opposite its entry point to the entry point, and knotted. The knot was buried within the graft. Figure 4 illustrates the specimens in the 3 groups.

Schematic sagittal diagram of cerclage positions at marked intervals along each graft in the 3 groups: (A) 2-cerclage, (B) 3-cerclage, and (C) 4-cerclage.

Specimen example from each group: (A) 2-cerclage, (B) 3-cerclage, and (C) 4-cerclage.
Biomechanical Testing
The prepared specimens were stored at –40°C to –30°C before testing and thawed for 48 hours to room temperature. Two identical specially designed jigs were made from PLA (polylactic acid) filament with an AnyCubic i3 Mega 3D printer (Anycubic). Each jig consisted of a tract that provided passage for the ALD button to sit on the outer surface of the jig, at one end of the tract. The other end of the tract was expanded into a socket to house the specimen. The 2 jigs were positioned mirroring each other to suspend the specimen between them (Figure 5A and 5B). Each specimen was pulled to failure with the Instron tensile tester 5943 machine. Figure 6 shows the final setup in the machine with the specially designed jigs and the specimen in situ.

Specially designed jigs: (A) one end of a specimen is seated in the socket and the adjustable loop device button is deployed at the opposite end of the tract in each jig; (B) close-up view of a button deployed on the outer end of the tract.

A specimen snugly fitted into the 2 specially designed jigs mounted on the Instron tensile tester 5943 machine.
The stiffness of each specimen (N/mm) was calculated as the initial slope of the linear portion of the stress-strain curve, and the ultimate load to failure (uLTF) (N) was recorded. The mode of graft failure was categorized into 3 types: cerclage failure, end-to-end failure, and graft material failure, which can occur in isolation or in combination. Cerclage failure was defined as cerclage loosening or rupture. End-to-end failure was defined as suture failure at the tendon ends. Graft material failure was defined as graft rupture involving only graft material.
Statistical Analysis
Statistical analysis was performed using SPSS statistical software, Version 29 (IBM Corp). Nominal variables are presented as the mean and standard deviation while categorical variables are presented as frequency and percentage. First, the data were stratified into the 3 groups (2-, 3-, and 4-cerclage specimens). Then, the Shapiro-Wilk test was performed to determine if the data set for stiffness and uLTF values in the 3 groups followed normal distribution and equal variances, which was negative. Therefore, to determine the relation of stiffness and uLTF across the groups, the Kruskal-Wallis test, a nonparametric test, was used followed by a Bonferroni post hoc test for pairwise analysis. Post hoc power analysis for stiffness and uLTF revealed a mean power of 0.93 and 0.98, respectively, which is greater than the desired power of 0.8, indicating that the sample size was sufficient. Second, the data were subdivided into single-tendon and double-tendon groups within each cerclage group. A multiple logistic regression analysis was performed to adjust for potential differences in material properties related to cadaveric factors, including age, sex, and side of the lower limb. As these factors were found to be insignificant, the Mann-Whitney U test, a nonparametric test, was used to assess the relation of stiffness and uTLF in relation to the number of tendons in each graft. Last, the Pearson chi-square test was performed to determine if the mode of graft failure was related to the 3 groups. Overall, the level of significance was set at P < .05.
Results
Table 1 shows the summary of the cadaveric details, graft used, stiffness, uLTF, and the mode of graft failure.
Summary of Findings in Each Cerclage Group a

Data are reported as n (%) or mean ± SD. BMI, body mass index.
Stiffness Across Cerclage Groups
The stiffness of the specimen increased with the number of cerclages used (Table 1 and Figure 7). The 4-cerclage specimens (56.6 ± 13.6 N/mm) and 3-cerclage specimens (55.9 ± 10.1 N/mm) were significantly stiffer than the 2-cerclage specimens (38.6 ± 5.1 N/mm), both with P values of .002 (Table 2). The stiffness of 3- and 4-cerclage specimens was not statistically different (P = .95) (Table 2).

Cluster boxplot illustrating stiffness in single- vs double-tendon specimens in each group.
P value Outcomes in Each Cerclage Group a

P-value outcomes of stiffness and uLTF comparing between each cerclage group. Dashes indicate not applicable.
Parenthetical P values correspond to Bonferroni post hoc analysis after Kruskal-Wallis test.
Ultimate uLTF Across Cerclage Groups
The uLTF of the graft constructs increased with the number of cerclages used (Table 1 and Figure 8). The 4-cerclage specimens (728.1 ± 144.7 N) and 3-cerclage specimens (696.6 ± 166.8 N) demonstrated significantly higher mean uLTF values than the 2-cerclage specimens (449.0 ± 45.9 N) with P values of .002 and .005, respectively (Table 2). The uLTF of 3- and 4-cerclage specimens was not statistically different (P = .81) (Table 2).

Cluster boxplot illustrating ultimate load to failure in single- vs double-tendon specimens in each group.
Stiffness in Single Versus Double Tendon per Graft Specimen
In the 2-cerclage group, the stiffness of the double-tendon specimens (52.0 ± 14.2 N/mm) was not statistically different from the single-tendon specimens (48.8 ± 13.0 N/mm) (P = .81) (Table 3 and Figure 7). In the 3-cerclage group, the stiffness of the double-tendon specimens (64.1 ± 9.9 N/mm) was significantly higher than the single-tendon specimens (49.2 ± 5.6 N/mm) (P = .014) (Table 3 and Figure 7). In the 4-cerclage group, the stiffness of the double-tendon specimens (56.0 ± 12.1 N/mm) was not statistically different from the single-tendon specimens (57.1 + 17.6 N/mm) (P = .62) (Table 3 and Figure 7). In summary, the double-tendon specimens showed greater stiffness of statistical significance only in the 3-cerclage group.
Outcomes Stratified According to Single or Double Tendon per Graft a

Data are reported as mean ± SD.
uLTF in Single Versus Double Tendon per Graft Specimen
In the 2-cerclage group, the uLTF of the double-tendon specimens (632.2 ± 212.6 N) was not statistically different from the single-tendon specimens (617.4 ± 160.5 N) (P = .46) (Table 3 and Figure 8). In the 3-cerclage group, the uLTF of the double-tendon specimens (753.7 ± 158.0 N) was not statistically different from the single-tendon specimens (650.7 ± 194.9 N) (P = .56) (Table 3 and Figure 8). In the 4-cerclage group, the uLTF of the double-tendon specimens (753.7 ± 223.1 N) was not statistically different from the single-tendon specimens (707.7 ± 92.9 N) (P = .56) (Table 3 and Figure 8). In summary, there was no demonstrated statistical difference in uLTF between single- and double-tendon specimens in all 3 groups.
Mode of Failure
The number of cerclage failures of single-tendon specimens (n = 14) and double-tendon specimens (n = 13) in all 3 groups showed no significant statistical difference (P = .63; P = .57) (Table 4). There are similar numbers of end-to-end failure across the 3 groups for single-tendon specimens (P = .35), and there were end-to-end failures in all double-tendon specimens in the 3 groups (Table 4). There was no statistically significant difference in graft material failure among the 2-, 3-, or 4-cerclage groups, for either single-tendon (P = .33) or double-tendon grafts (P = .34) (Table 4). There was no ALD failure noted.
Mode of Graft Failure in Each Group a

Data are reported as n (%). NA, not applicable, as all double-tendon grafts experienced end-to-end failure.
None of the specimens with 2 cerclages exhibited an isolated mode of failure, whereas the specimens with 3 and 4 cerclages showed similar numbers of occurrences (P = .50) (Table 5). While there is a trend of reduction in cerclage failure combined with end-to-end failure with an increase in number of cerclages, it was not statistically significant in comparison with the other various combined modes of failure across the 3 groups (P = .17) (Table 5). There was also no statistical difference across the groups in terms of total isolated versus total combined modes of failure (P = .31) (Table 5).
Isolated Versus Combined Mode of Graft Failure in Each Group a

Data are reported as n (%).
P value across isolated mode of failure only.
P value across combined mode of failure only.
P value of total isolated vs total combined mode of failure.
Discussion
Several studies have provided convincing evidence that a minimal ACL graft diameter of 8 mm is needed to reduce the risk of revisions.15,16,19,22 Inadequate ACL graft size has been shown to contribute to ACL reconstruction failure rates of 1.8% to 10.4%. 26 It had been reported that the mean graft diameter using the semitendinosus tendon in certain patient populations are approximately 7.4 mm 27 or 7.9 mm, 1 often necessitating the inclusion of the gracilis tendon to attain the desired graft size. This is more prevalent in Southeast Asians, females, and patients with small stature. 29 Data from the current study showed an added advantage of increased stiffness in using a double tendon for a 3-cerclage graft. The double-tendon specimens were significantly stiffer than the single-tendon specimens in the 3-cerclage group. This is likely due to better load distribution across both tendons, thereby reducing the risk of failure in each strand and increasing the graft's resistance to deformation.11,12 However, this observation was not present in the double-tendon specimens in the 2- cerclage and 4-cerclage groups. A possible explanation is that the 4-cerclage specimens were stronger with 4 cerclages and this offset the effect of improved load distribution and greater resistance to deformation between single and double tendon per graft. In the 2-cerclage specimens, the advantage of cerclages and double tendon was overall not adequate as evidenced by the statistically significant lower stiffness and uLTF values. This finding supports the use of both gracilis and semitendinosus to achieve a minimum graft diameter of 10 mm in selected patient population with a 3-cerclage graft. There is no similar advantage noted in a 2-cerclage or 4-cerclage graft.
Overall, the data demonstrated that 3- and 4-cerclage specimens exhibited similar stiffness and uLTF. Both groups showed statistically significant higher stiffness and uLTF compared with 2-cerclage specimens. It is postulated that a double-tendon 3-cerclage graft offers similar functional strength to a 4-cerclage graft, implying the fourth cerclage offers no significant clinical benefit in a graft of ≥10-mm diameter. From a biomechanical perspective, 2-cerclage grafts appear suboptimal compared with 3- and 4-cerclage grafts, as reflected by their significantly lower stiffness and uLTF values. Further clinical studies are warranted to evaluate the implications of these findings.
There was a reduction in cerclage failure with more cerclages used. It is likely that additional cerclages improve load distribution and reduced the likelihood of individual cerclage failure. Conversely, an increase in graft material rupture was observed with additional cerclages, demonstrating that graft strength increased proportionately with the number of cerclages, up to the point where graft material strength became the limiting factor. From this stage, additional cerclages offers no value. A trend toward reduced combined failure (cerclage and end-to-end) was observed with the use of more cerclages, although the result was not statistically significant. All the specimens in the 2-cerclage group had combined mode of failure, compared with 77.8% in the 3- and 4-cerclage groups. The remaining specimens in the 3 and 4-cerclage groups sustained isolated modes of failure (isolated end-to-end failure or graft material rupture).
Our study employed uniaxial tensile loading to isolate the intrinsic mechanical properties of the graft–cerclage constructs. Paschos et al 20 demonstrated that under uniaxial tension, native ACL failure typically follows 3 patterns, beginning with partial or complete tearing of fiber bundles, after which the remaining intact fibers continue to bear load. However, in vivo, reconstructed ACL grafts are exposed to complex, multiplanar forces, particularly during activities involving pivoting or combined anterior and rotational loading, which have been shown to increase rotational instability after ACL reconstruction. 9 While our uniaxial testing does not fully replicate the complex in vivo environment, particularly at the bone-graft interface, it provides a standardized method for comparing mechanical properties between cerclage constructs. Future studies incorporating cyclic and multiplanar loading may offer further insight into clinically relevant failure patterns.
Limitations
There are limitations in all biomechanical studies. First, the donor age group was older than the clinically relevant population of younger and more active athletes. The use of intact but degenerative cadaveric specimens and various tendons harvested could alter the biomechanical performance of the grafts, potentially skewing the outcomes. Second, the graft specimens were explanted and tested outside of the intact knee, which may not fully replicate the mechanical properties observed in a functional native knee. There was no cyclic loading or rotational torque applied, no implantation into bone sockets, and no healing process between graft and bone. Third, the application of uniaxial loading alone does not completely capture the complex, multiplanar forces to which the ACL is subjected during failure in vivo. Last, the absolute values in stiffness and uLTF for the specimens might not be comparable with selected studies,6,18,23 and this likely relates to graft preparations, test conditions, and quality of the cadavers.
Conclusion
It is postulated that a double-tendon 3-cerclage graft achieves similar strength to a 4-cerclage graft, provided a diameter of ≥10 mm is used. From a biomechanical perspective, 2-cerclage grafts appear suboptimal compared with 3- and 4-cerclage grafts, as reflected by their significantly lower stiffness and uLTF values with no improvement after the addition of a second tendon. The current findings contribute to the existing knowledge in all-inside graft preparation, as it is essential to choose the most effective technique to achieve a stable reconstruction.
Footnotes
Final revision submitted October 7, 2025; accepted October 9, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: The research was funded by the Professor Low Boon Yong department research grant. S.-Y.J.L. has received funding from Smith & Nephew on other occasions. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.