
Abstract
Background:
The self-cinching stitch has been verified to have high mechanical strength. The mechanical strength of combining transosseous rotator cuff repair (RCR) and the self-cinching stitch in the lateral row is unknown.
Purpose/Hypothesis:
The purpose of this study was to evaluate the biomechanical properties of transosseous RCR combined with the cinch stitch in the lateral row. We hypothesized that this construct would have better mechanical strength than would transosseous repair using a vertical cinch stitch or simple stitch.
Study Design:
Controlled laboratory study.
Methods:
Rotator cuff tears were simulated in 48 porcine shoulder specimens. The tears were repaired using 1 of 6 repair configurations: 2–simple stitch transosseous repair alone (group 2TO), with a vertical cinch stitch (group 2TO-VC), or with a horizontal cinch stitch (group 2TO-HC) or 4–simple stitch transosseous repair alone (group 4TO), with a vertical cinch stitch (group 4TO-VC), or with a horizontal cinch stitch (group 4TO-HC). All specimens were set at a 45° angle from the footprint and underwent cyclic loading from 10 to 160 N for 200 cycles, followed by a load-to-failure test at 10 mm/min.
Results:
During cyclic loading, all specimens in group 2TO and half of the specimens in group 2TO-VC failed by suture pullout. In the other groups, none of the specimens failed before 200 cycles. The yield load in group 2TO-HC was significantly greater than that in group 2TO-VC (261.43 vs 219.54 N, respectively; P < .05). There were significant differences between groups 4TO-HC and 4TO with regard to elongation (3.92 vs 5.68 mm, respectively), yield load (304.04 vs 246.94 N, respectively), and linear stiffness (63.44 vs 52.28 N/mm, respectively) (P < .01 for all). Group 4TO-HC also had shorter elongation and a superior yield load and linear stiffness compared with group 2TO-HC (P < .05 for all), and group 4TO-VC had shorter elongation and a stronger maximum load to failure and yield load than did group 2TO-VC (P < .05 for all).
Conclusion:
Increasing the number of medial simple stitches can prevent suture pullout. Adding the horizontal cinch stitch to the lateral row in transosseous repair can further improve biomechanical properties through a self-cinching mechanism.
Clinical Relevance:
Transosseous RCR with a horizontal cinch stitch in the lateral row may reduce the retear rate.
The surgical technique to repair rotator cuff tears has progressed from open and mini-open methods of creating transosseous bone tunnels to arthroscopic methods using various devices and suture anchors. Arthroscopic rotator cuff repair (RCR) has an advantage: it is a less invasive technique, although its outcomes are similar to those of the open and mini-open approaches. 1,2,27
The initial fixation strength of the tendon to bone is thought to be one of the most important factors affecting the success of RCR. Gerber et al 7 suggested that the ideal RCR technique should have high initial fixation strength, allowing minimal gap formation between the tendon and bone. Many studies have investigated the biomechanical properties of RCR by performing the cyclic loading test and load-to-failure test. 4,6,7,9,12,15,18,25
In 2006, Park et al 16 described the transosseous-equivalent (TOE) repair technique, also called suture bridge repair, for rotator cuff tears. Although TOE repair using medial mattress sutures obtained superior ultimate failure loads and energy absorbed to failure compared with double-row repair, 18 Cho et al 5 noted that mattress sutures of the medial row caused retears because of the possibility of strangulation and relatively quick necrosis of the rotator cuff. In 2016, Hawi et al 8 reported that the simple cinch stitch, which is a self-cinching stitch, is simple and easy to perform for arthroscopic RCR. It has stronger biomechanical strength compared with a simple stitch and horizontal mattress stitch. Mihata et al 15 reported that adding simple stitches to the lateral row in TOE repair resulted in better biomechanical properties at both 0° and 40° of abduction. However, the mechanical strength of combining transosseous repair with the self-cinching stitch in the lateral row is unknown.
We conceived of a mattress cinch stitch technique that could adequately grasp tissue from the tendon, and in this study, we aimed to evaluate the biomechanical properties of transosseous RCR combined with the cinch stitch in the lateral row. We hypothesized that this construct would have better mechanical strength than would transosseous repair using a vertical cinch stitch or simple stitch. To assess in detail the effect of the cinch stitch on biomechanical properties, we tested different numbers of sutures through the tendon using the same repair method. Thus, 3 transosseous RCR configurations were assessed with varying suture throws in this study.
Methods
Specimen Preparation
A total of 48 fresh-frozen porcine shoulders were bought from a meat packer and used in this study. The specimens were stored at −40°C and thawed for 24 hours at room temperature before dissection. All soft tissues were removed from the humerus, except the infraspinatus muscle and tendon. The infraspinatus tendon was carefully released from the greater tuberosity using a scalpel. There were no preexisting abnormalities in any specimens. To prevent tissue damage, the specimens were kept moist using saline, as necessary, during testing.
The supraspinatus tendon measures 25 mm wide and 12 mm long, as reported by Ruotolo et al. 23 For this reason, a 20 × 10–mm rectangular area was used in this study. To simulate a full-thickness rotator cuff tear, all infraspinatus tendons were trimmed to a 20-mm width, and we measured the thickness using a digital caliper (Absolute Digimatic Caliper; Mitutoyo). The repair site was within 10 mm away from the free edge of the tendon. No. 2 FiberWire suture (Arthrex) was used in all groups.
Repair Techniques
The specimens were randomly assigned to 1 of 6 transosseous repair configurations (n = 8 specimens per group). The first 3 groups were repaired using 2 transosseous simple stitches with 4-mm intervals at 10 mm from the stump (group 2TO) or with a vertical cinch stitch (group 2TO-VC) or horizontal cinch stitch (group 2TO-HC) added in the lateral row at 5 mm from the stump (Figure 1). For the vertical cinch stitch, a double-folded thread was passed through the tendon, and the thread-free ends were passed through the loop. For the horizontal cinch stitch, a double-folded thread was passed through the mattress sutures with a width of 4 mm, and the thread-free ends were passed through the loop (Figure 2). We also evaluated the 3 previously mentioned repair configurations using 2 additional simple stitches—1 on each side of the tendon (group 4TO, group 4TO-VC, and group 4TO-HC) (Figures 3 and 4).

The 3 different transosseous repair configurations using 2 simple stitches: (A) group 2TO, (B) group 2TO-VC, and (C) group 2TO-HC. Red indicates the cinch stitch, and blue indicates the simple stitch. 2TO, 2–simple stitch transosseous repair; 2TO-VC, 2TO with a vertical cinch stitch; 2TO-HC, 2TO with a horizontal cinch stitch.

Repair configurations using the cinch stitch: (A) vertical cinch stitch and (B) horizontal cinch stitch.

The 3 different transosseous repair configurations using 4 simple stitches: (A, D) 4TO, (B, E) 4TO-VC, and (C, F) 4TO-HC. (A-C) The blue lines show simple stitches, and the red lines show cinch stitches. 4TO, 4–simple stitch transosseous repair; 4TO-VC, 4TO with a vertical cinch stitch; 4TO-HC, 4TO with a horizontal cinch stitch.

Biomechanical testing setup.
All inferior limbs of the simple stitch in the medial row were passed through each of 2 or 4 straight bone tunnels created in the footprint. The bone tunnels were created using a 1.6-mm K-wire at an angle of 45° from the footprint. All bone tunnels were not damaged during RCR. The free limbs of the cinch stitch were passed through each of the 2 central bone tunnels. In the groups with added cinch stitches, we sutured the lateral row, followed by the medial row.
Biomechanical Testing
Using an Instron 8872 material testing machine (Instron), each specimen was clamped at 20 mm from the stump and set at an angle of 45° from the footprint (Figure 4). The angle allowed the tendon to be stressed using the greatest tensile force. 30 The humerus was firmly fixed using bolts and nuts.
After preloading at 10 N/min, cyclic loading was performed 200 times between 10 and 160 N at 0.5 Hz to the record peak-to-peak elongation. The number of cyclic loads was set to 200 times because 80% of elongation occurs by 100 cycles during the cyclic loading test. 24 Elongation was defined as displacement between the first cyclic peak and the last cyclic peak. 6,14 In the study by Burkhart et al, 3 a 180-N load was based on an estimated two-thirds of the load of a maximum contraction of the rotator cuff. Salata et al 25 set the upper cyclic loading limit to 160 N as a modified protocol based on the previous study. 17,18 Assuming rehabilitation would include early active exercises, we chose a 160-N load for the upper cyclic loading limit.
After cyclic loading, the load-to-failure test was performed at a crosshead speed of 10 mm/min. We calculated the maximum load to failure, yield load, and linear stiffness from the load-displacement curve and recorded the mode of failure. The maximum load to failure was defined as the peak force, and the yield load was defined as the force at which the load-displacement curve deviated from the linear region. Linear stiffness was calculated by determining the slope of the load-displacement curve following the initial toe region (Figure 5).

Load-displacement curve: maximum load to failure (A), yield load (B), and linear stiffness (C).
Statistical Analysis
A 1-way analysis of variance, followed by the Tukey post hoc test or Student t test, was performed separately in the groups with 2 medial simple stitches and in those with 4 medial simple stitches to compare the thickness of the tendon, elongation after preloading, maximum load to failure, yield load, linear stiffness, and peak-to-peak elongation. In addition, the Student t test was performed to compare the groups with different numbers of medial stitches using the same repair technique. The level of statistical significance was set at P < .05. The statistical analyses were performed with EZR Version 1. 40 (R Core Team).
Results
There were no significant differences in the thickness of the infraspinatus tendon among all groups (Table 1).
Thickness of the Infraspinatus Tendon a

a Data are reported as mean ± SD. 2TO, 2–simple stitch transosseous repair; 2TO-VC, 2TO with a vertical cinch stitch; 2TO-HC, 2TO with a horizontal cinch stitch; 4TO, 4–simple stitch transosseous repair; 4TO-VC, 4TO with a vertical cinch stitch; 4TO-HC, 4TO with a horizontal cinch stitch.
Cyclic Loading Test
The biomechanical results are summarized in Table 2. Regarding the 2–simple stitch transosseous repair groups, all specimens in group 2TO and 4 of the 8 specimens in group 2TO-VC failed by suture pullout during cyclic loading. The specimens in group 2TO failed before 10 cycles, and the specimens in group 2TO-VC failed before 70 cycles. There was no significant difference in elongation between the specimens in group 2TO-VC that did not fail and those in group 2TO-HC.
Biomechanical Results a

a Data are reported as mean ± SD. Dashes indicate the values were unmeasurable. 2TO, 2–simple stitch transosseous repair; 2TO-VC, 2TO with a vertical cinch stitch; 2TO-HC, 2TO with a horizontal cinch stitch; 4TO, 4–simple stitch transosseous repair; 4TO-VC, 4TO with a vertical cinch stitch; 4TO-HC, 4TO with a horizontal cinch stitch.
b All specimens in group 2TO failed by suture pullout during cyclic loading.
c Four specimens in group 2TO-VC failed by suture pullout during cyclic loading.
d Significant difference (P < .01) between groups 4TO and 4TO-HC.
e Significant difference (P < .05) between groups 2TO-VC and 4TO-VC.
f Significant difference (P < .01) between groups 2TO-HC and 4TO-HC.
g Significant difference (P < .05) between groups 2TO-VC and 2TO-HC.
h Significant difference (P < .01) between groups 2TO-VC and 4TO-VC.
i Significant difference (P < .05) between groups 2TO-HC and 4TO-HC.
Regarding the 4–simple stitch transosseous repair groups, none of the specimens failed before 200 cycles. Group 4TO-HC showed significantly smaller elongation (3.92 ± 0.43 mm) compared with group 4TO (5.68 ± 1.16 mm) (P < .01). However, there were no significant differences between group 4TO-VC (4.56 ± 1.09 mm) and the other groups.
Comparing group 2TO-VC with group 4TO-VC, elongation was significantly longer in group 2TO-VC (5.99 ± 1.31 vs 4.56 ± 1.09 mm, respectively; P < .05). Moreover, comparing group 2TO-HC with group 4TO-HC, elongation was significantly longer in group 2TO-HC (5.78 ± 1.48 vs 3.92 ± 0.43 mm, respectively; P < .01).
Load-to-Failure Test
As for the 3 groups with 2 simple stitches in the medial row, group 2TO-HC showed a significantly stronger yield load (261.43 ± 34.85 N) than did group 2TO-VC (219.54 ± 22.61 N) (P < .05). There were no significant differences in the maximum load to failure and linear stiffness between the groups (Figure 6).

Comparison of the maximum load to failure, yield load, and linear stiffness in groups 2TO-VC and 2TO-HC. *P < .05. 2TO-VC, 2TO (2–simple stitch transosseous repair) with a vertical cinch stitch; 2TO-HC, 2TO with a horizontal cinch stitch.
As for the 3 groups with 4 simple stitches in the medial row, no significant differences were observed in the maximum load to failure among the 3 groups. Group 4TO-HC showed a significantly higher yield load and linear stiffness (304.04 ± 41.95 N and 63.44 ± 8.15 N/mm, respectively) than did group 4TO (246.94 ± 38.86 N and 52.28 ± 7.85 N/mm, respectively) (P < .01 for both). However, no significant differences were observed between group 4TO-VC (282.36 ± 32.37 N and 56.21 ± 8.58 N/mm, respectively) and the other groups (Figure 7).
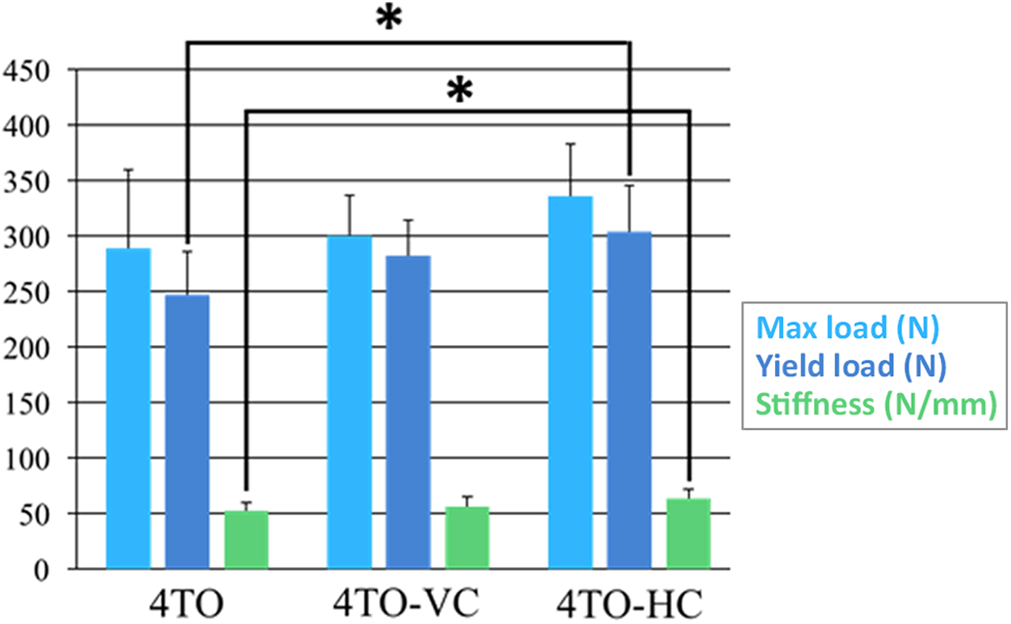
Comparison of the maximum load to failure, yield load, and linear stiffness in groups 4TO, 4TO-VC, and 4TO-HC. *P < .01. 4TO, 4–simple stitch transosseous repair; 4TO-VC, 4TO with a vertical cinch stitch; 4TO-HC, 4TO with a horizontal cinch stitch.
Comparing group 2TO-VC with group 4TO-VC, the maximum load to failure and yield load of group 4TO-VC (300.50 ± 36.30 N and 282.36 ± 32.37 N, respectively) were significantly stronger than were those of group 2TO-VC (233.36 ± 31.74 N and 219.54 ± 22.61 N, respectively) (P < .05 and P < .01, respectively). No significant difference was observed in linear stiffness between the groups.
Comparing group 2TO-HC with group 4TO-HC, the yield load and linear stiffness of group 4TO-HC (304.04 ± 41.95 N and 63.44 ± 8.15 N, respectively) were significantly stronger than were those of group 2TO-HC (261.43 ± 34.85 N and 54.32 ± 5.19 N, respectively) (P < .05 for both). No significant difference was observed in the maximum load to failure between the groups.
With regard to the mode of failure, all specimens in the 6 groups failed by suture pullout through the tendon (Figure 8).

Mode of failure (specimen of group 4TO after load-to-failure test). 4TO, 4–simple stitch transosseous repair.
Discussion
In this study, we conducted biomechanical testing of porcine infraspinatus tendons, assuming its application to human supraspinatus tendon repair. We demonstrated that adding horizontal cinch stiches in the lateral row in transosseous RCR significantly improved biomechanical properties and that increasing the number of throws in the medial row could prevent suture pullout at 45° of abduction.
The vertical cinch stitch is a type of self-cinching stitch represented by lasso-loop, lasso-mattress, and double-cinch stitches. 8,13,19 Liodakis et al 13 evaluated the biomechanical properties of 3 self-cinching stitch configurations (lasso-loop, lasso-mattress, and simple cinch stitches) using the infraspinatus tendon of sheep. The simple cinch stitch had a biomechanical strength equal to that of the lasso-mattress stitch and a biomechanical strength better than that of the lasso-loop stitch.
Tsuge et al 28 developed an intratendinous tendon suture technique using looped nylon sutures for finger flexor tendon injuries, and the repair technique showed good clinical outcomes. The horizontal cinch stitch is similar to an intratendinous tendon suture technique: the double-guided suture crosses the tendon fiber in the vertical direction and grasps the tissue of the tendon.
In this study, all specimens in group 2TO and 4 of the 8 (50%) specimens in group 2TO-VC failed by suture pullout through the tendon during the cyclic loading test. Although adding the vertical cinch sutures in the lateral row could not prevent pullout of the suture threads, none of the specimens from group 2TO-HC failed during the test. Furthermore, the yield load of group 2TO-HC was significantly greater than was that of group 2TO-VC. Although no significant differences were observed in the maximum load to failure between group 4TO and group 4TO-VC, group 4TO-HC showed shorter elongation as well as a higher yield load and linear stiffness than did group 4TO. Whereas the vertical cinch technique involves a single pass through the tendon, the horizontal cinch technique entails a double pass through the tendon. We consider the horizontal cinch stitch to have grasping strength superior to that of the vertical cinch stitch.
Few previous in vivo studies have evaluated the biomechanical properties of transosseous repair versus TOE repair using suture anchors. Salata et al 25 evaluated TOE repair using a mattress suture in the medial row and transosseous repair with 2 points of passage through the rotator cuff tendon. TOE repair had a significantly greater maximum load than did transosseous repair. By contrast, Kilcoyne et al 9 evaluated the biomechanical properties of transosseous repair using 6 simple stitches through the tendon and TOE repair using medial mattress sutures. They showed that transosseous repair had a significantly higher failure load compared with TOE repair. Furthermore, they suggested that the number of sutures may lead to differences in biomechanical performance.
In this study, increasing the number of medial simple stitches for transosseous repair prevented pullout of suture threads during cyclic load testing. In adding the cinch stitch, groups 4TO-VC and 4TO-HC had significantly superior biomechanical properties compared with groups 2TO-VC and 2TO-HC, respectively.
Sano et al 26 reported that a concentration of biomechanical stress was observed around the medial-row tying site in double-row repair. At a shoulder abduction angle of 45°, stress was concentrated in the tendon, especially in the medial row. Biomechanical factors are important for bone-to-tendon healing, and surgeons can potentially control the RCR technique. Park et al 17 reported that the TOE repair technique using medial mattress sutures had better biomechanical strength and significantly increased the contact area and interface pressure between the tendon and footprint. Busfield et al 4 and Leek et al 12 compared the biomechanical strength of the TOE repair technique with the addition of mattress sutures in the medial row to the knotless repair technique. They reported increased gapping at the repair site and a decreased load to failure in knotless TOE repair. These data showed the importance of medial-row knots in protecting the repair site from biomechanical stress. However, a previous clinical outcome study reported that no significant difference was observed in retear rates between double-row repair and TOE repair using medial knots. 10 In the literature, 5,22 TOE repair using medial knots has been shown to result in retears at the musculotendinous junction because of the concentration of stress on the medial row.
Our study revealed that adding the horizontal cinch stitch could increase biomechanical properties by its grasping mechanism. The self-cinching mechanism is effectively utilized when elongation occurs during tensile loading, resulting in increased strength in grasping the tendon in the lateral row. Therefore, knotting the medial row using the horizontal cinch stitch in the lateral row might not only cause additional tissue damage in the medial row but also inhibit the self-cinching mechanism in the lateral row. On the contrary, the double-row repair technique, using a simple stitch in the medial row and the horizontal cinch stitch in the lateral row, should have a contact area similar to that in TOE repair, might not inhibit the self-cinching mechanism, and could decrease the incidence of retears in the medial row.
Based on the results of our study, despite the fact that group 4TO-HC had the strongest biomechanical properties, all specimens failed by suture pullout. Many studies have reported the same mode of failure. Liodakis et al 13 reported that all types of self-cinching stitches, including the vertical cinch stitch, failed by suture pullout. Hawi et al 8 reported that the simple cinch stitch failed because of a combination of knot breakage and suture pullout. Ponce et al 20 assessed the effect of tissue bite size on various stitches at 5 or 10 mm away from the free end of the tendon. They reported that the strength of the stitch configuration was affected by the length of the tissue bite. We thought that one of the factors causing suture pullout in our study was the small tissue bite size of the cinch stitch at 5 mm away from the tendon edge.
Arthroscopic RCR is a common surgical technique that achieves good outcomes. There have been changes in arthroscopic suture anchor techniques, from the single row to double row and then the suture bridge. Recently, several studies 11,21 have reported the clinical outcomes of arthroscopic transosseous repair techniques. Kuroda et al 11 reported that these techniques achieved low retear rates and clinical scores as good as those of suture anchor techniques. In addition, they also pointed out that there are several problems with suture anchor techniques such as dislodgement, expensive cost, knot impingement, and difficulty of reoperations. Randelli et al 21 reported that the arthroscopic transosseous repair technique has the advantages of a larger suture-tendon contact area, increasing adhesion pressure at the footprint surface. They evaluated the clinical and radiologic results of transosseous repair compared with suture anchor repair, and there were no significant differences between the groups.
In this study, we investigated the biomechanical properties of various transosseous repair techniques using an open approach. We consider that the cinch stitch can be performed easily using the arthroscopic approach and can be applied to arthroscopic RCR techniques. In the future, we plan to conduct a biomechanical study of suture bridge repair combined with cinch sutures and mattress sutures.
This study has several limitations. First, we used porcine infraspinatus tendons instead of human tendons. The porcine bone quality may be better than that seen in elderly humans. However, porcine tendons have mechanical properties similar to those of humans, 29 and the size of porcine infraspinatus tendons is similar to that of human supraspinatus tendons. In addition, the porcine tendon is inexpensive and easily available in our country. Second, we used an open repair technique, and knot tying in all suture techniques was performed using manual maximum strength. However, manual maximum strength had no effect on the results because none of the sutures broke during the load-to-failure test in this study. Third, we measured elongation and not gap formation using a digital tracking system. It is possible that peak-to-peak elongation may not accurately demonstrate the effect of cinch stitches in the lateral row. Fourth, this is a time-zero study with in vitro testing that did not take into account the physiologic healing process and patient backgrounds.
Conclusion
The study results indicated that increasing the number of medial simple stitches can prevent suture pullout. Adding horizontal cinch stitches to the lateral row can further improve biomechanical properties through a self-cinching mechanism. The horizontal cinch stitch is a simple technique and can be easily performed in arthroscopic RCR. We believe that the use of the horizontal cinch stitch may be able to reduce rotator cuff retear rates.
Footnotes
Acknowledgment
The authors thank M. Sekikawa and the department administrators for assistance with the study.
Final revision submitted November 19, 2020; accepted December 21, 2020.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.