
Abstract
Background:
Transosseous rotator cuff repair provides robust fixation and broad footprint compression without the risk of foreign body reaction that may be seen with suture anchors. We present our technique for anchorless transosseous repair using a modern device to efficiently create bone tunnels and assist in suture passage.
Indications:
Tears of the supraspinatus tendon, with or without extension to the infraspinatus, in patients with acute or chronic tears, with good bone quality, and who fail appropriate nonoperative management.
Technique:
The beach-chair position with an articulating arm holder is preferred for this procedure. A glenohumeral diagnostic arthroscopy is performed, and intra-articular pathology is addressed as needed. The arthroscope is brought into the subacromial space, and a lateral viewing portal is established. A thorough bursectomy with or without acromioplasty is performed to attain visualization of the cuff. After the tear is identified, the tendon edges are debrided. It is critical to determine the tear pattern, the reduction maneuvers necessary, and the number of bone tunnels that are warranted. The desired location of the bone tunnel is marked with a pilot hole. The device is positioned over the pilot hole and a power drill is advanced through the lateral cortex. The device assists in creating a bone tunnel through the greater tuberosity and passes a nitinol loop through the tunnel. The loop is retrieved by the device and is brought to the lateral portal. Sutures are loaded into the loop and are brought through the bone tunnel. The sutures are then passed through the tendon using a curved retrograde suture passer in simple fashion and are tied to secure the tendon to the footprint. For larger tears, 2 or 3 tunnels may be used to widen the area for footprint compression. The specific configuration used will depend on the tear size, pattern, and surgeon preference.
Results:
Arthroscopic transosseous repairs have yielded promising results. Healing rates are comparable to anchor-based techniques, with the benefit of avoiding foreign bodies at the footprint.
Discussion:
Anchorless transosseous rotator cuff repair may be reproducibly performed with the use of a modern device for bone tunnel creation and suture passage. However, this technique should be used with caution in patients with osteoporosis or poor bone quality due to theoretical concerns of greater tuberosity fracture or suture pullout through the tunnels.
Patient Consent Disclosure Statement:
The author(s) attests that consent has been obtained from any patient(s) appearing in this publication. If the individual may be identifiable, the author(s) has included a statement of release or other written form of approval from the patient(s) with this submission for publication.
This is a visual representation of the abstract.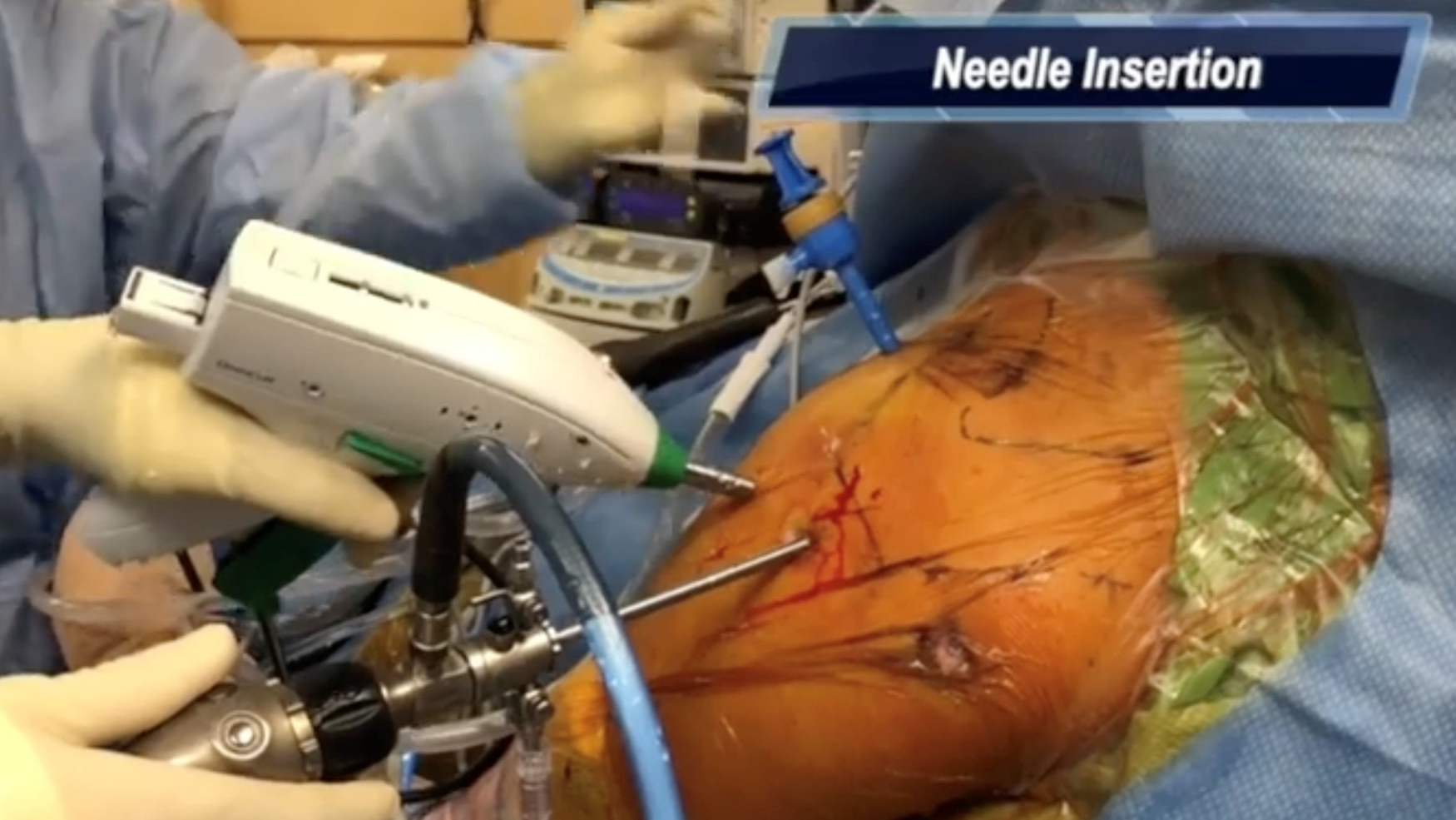
Keywords
Video Transcript
In this video, we describe our preferred surgical technique for anchorless transosseous rotator cuff repair using the OmniCuff device. The senior author has a relevant disclosure for this presentation which can be found on the AAOS (American Academy of Orthopaedic Surgeons) website.
The rotator cuff is a critical structure in the shoulder as it maintains stability through the concavity-compression mechanism and contributes to active glenohumeral motion. 6 Diagnosis of symptomatic tears has increased since the year 2000 to 715 per 100,000 person-years in 2018. 9 Transosseous anchorless repairs produce a wide area for footprint compression. They also provide a greater surface for tendon-to-bone healing compared with anchor-based repairs, while avoiding potential foreign body reactions to anchors. 6 Meta-analyses have indicated that transosseous repairs yield comparable patient-reported outcomes compared with anchor-based techniques.3,7 This technique should be reserved for patients with reasonable bone quality to avoid the risk of greater tuberosity fracture. It may be used in both primary and revision settings and may be particularly useful in revision cases where old anchors need to be removed, leaving limited area for secure anchor fixation.
Our patient is an active 76-year-old woman who presented with left shoulder pain that had been ongoing for 6 months. She reported pain with overhead activities and pain with activities of daily living. She underwent an exhaustive course of conservative treatment, which included physical therapy and a subacromial corticosteroid injection. On physical examination, she demonstrated full range of motion comparable to her contralateral shoulder, though she was limited by pain, particularly with forward elevation. She had 5/5 strength throughout testing of her rotator cuff. She also demonstrated positive Jobe's sign and positive Neer and Hawkins impingement tests. Radiographs demonstrate no evidence of glenohumeral arthritis and a type 1 acromion. Magnetic resonance imaging demonstrates a full-thickness anterior supraspinatus tear with Goutallier 1 fatty infiltration.
The patient is positioned in the usual beach-chair position and anatomic landmarks are marked. A posterior view and portal are established and standard diagnostic arthroscopy of the glenohumeral joint is performed. Next, the subacromial bursectomy is performed and the tear is identified. It is important to perform a thorough bursectomy of the subdeltoid space so as not to impede the path of the OmniCuff device. A stab incision is made off the lateral edge of the acromion and a punch is used to create a pilot hole at the desired location of the bone tunnel, which is located at the medial aspect of the footprint. An anterolateral portal is established for usage of the OmniCuff device. Viewing from the lateral portal, the needle is inserted from the tip of the device into the pilot hole. The lower working channel port of the device is positioned at the lateral cortex of the greater tuberosity. A drill bit is then introduced into the working channel port of the device and creates the bone tunnel. A cartridge containing nitinol wire is then placed in the device. The needle is advanced through the superior opening of the bone tunnel by repeatedly squeezing the lever. A diagram of the needle capturing the nitinol loop within the cartridge is seen here. Once the indicator on the device signals that the nitinol loop has been captured by the needle, the device may be removed, and a nitinol loop remains passed through the bone tunnel. The nitinol loop is then used to pass 3 suture tapes through the bone tunnel. These sutures are then docked through the anterior portal for suture management purposes. We can then proceed with the rotator cuff repair. The specific configuration used will depend on the tear size, pattern, and surgeon preference. In this case, we passed 3 sutures through the isolated supraspinatus tear using our standard technique. Viewing laterally, we used a retrograde curved suture passer through the posterior portal and retrieved through the anterolateral portal. After all sutures are passed, we reduced the tear and proceeded with tying each suture using a series of reversing half hitches on alternating posts. The final transosseous repair can be seen here. Knots are typically placed over the tendon to maximize footprint compression. It should be noted that surgeons should be careful not to overtighten knots with their first throws to avoid rare cases of suture cutout.
For larger tears, 2 or 3 tunnels may be used to widen the area for footprint compression. The senior author prefers an X-box configuration in which limbs from one suture from each adjacent tunnel are tied to one another, while the second suture from each tunnel is passed and tied in simple fashion. Limbs from adjacent tunnels may also be tied in mattress fashion (Figure 1). 4 The specific configuration used will depend on the tear size, pattern, and surgeon preference. While we have found this particular device to be effective and efficient in creating bone tunnels for transosseous repair, there are a number of commercially available devices that may be used for this purpose.
Patients progress through their postoperative rehabilitation in 3 phases as listed below. There are a number of pearls and pitfalls for this procedure. First, it is important to do a thorough bursectomy to establish visualization of both the tear and the lateral aspect of the greater tuberosity for tunnel localization. Next, it is important to reduce the tear and be precise about choosing your tunnel placement to ensure that your sutures adequately compress the tendon against the footprint. The lateral portal for this procedure is approximately 1 cm distal to a typical rotator cuff repair performed with anchors. This will allow you to get the proper trajectory for your tunnels. And finally, internally and externally rotating the arm allows you to create your tunnels in the correct position in the sagittal plane. Along those lines, it is important to avoid placing your tunnels too close together in the anterior-posterior dimension. And finally, we advise using suture tape for severely osteoporotic bone to reduce the chance of suture cutout. There are a number of potential benefits of using a transosseous repair. This technique allows broad footprint coverage without placing any foreign bodies in the tuberosity compared with anchor-based repairs. 2 There is therefore no risk of anchor dislodgement or overcrowding of the tuberosity in revision cases. Lower rates of failure at the musculotendinous junction compared with transosseous equivalent repairs have been observed.2,5 In addition, biomechanical models have demonstrated improved vascularity at the bone-tendon interface with transosseous repairs. 1 Finally, a prospective randomized controlled trial demonstrated similar functional results compared with a single row repair, although patients undergoing transosseous repair reported lower postoperative pain levels. 8 Thank you for watching our technique.
Footnotes
Submitted November 27, 2022; accepted June 16, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: M.R.C. received support for education from Medwest Associates and hospitality payments from Encore Medical and Medical Device Business Services. J.A.A. is a board or committee member for American Shoulder and Elbow Society (ASES), ASES Foundation, Mid Atlantic Shoulder and Elbow Society, Pacira, and Shoulder 360; receives research support from Arthrex, Inc, Department of Defense, Zimmer Biomet, OREF, Orthofix, and Lima; is a consultant for Bioventus, DJO, Globus, Stryker, and Zimmer Biomet; received consulting fees from Encore Medical, Wright Medical Technology, Pacira Therapeutics, and Trice Medical; has stock or stock options in Asvumed, Shoulder JAM LLC, Marlin Medical Alliance, LLC, OBERD, and OTS Medical; receives royalties from DJO, Integra Life Sciences, Globus, Slack Orthopaedics, Smith + Nephew, Stryker, Zimmer Biomet, and OsteoCentric Technologies; and co-founded Shoulder JAM LLC and Shoulder 360. N.N.V. is a board or committee member for AOSSM, ASES, and Arthroscopy Association of North America; is on the editorial or governing board for Knee and SLACK Incorporated; received consulting fees from Athrex and Stryker; royalties from Athrex; hospitality payments from Spinal Simplicity; research support from Arthrex, Inc, Breg, Ossur, Smith + Nephew, and Wright Medical Technology, Inc; publishing royalties, financial, or material support from Arthroscopy and Vindico Medical-Orthopedics Hyperguide; has stock or stock options in Cymedica, Minivasive, and Omeros; is a paid consultant for Minivasive and Orthospace; and receives intellectual property royalties from Smith + Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.