
Abstract
Background:
Previous studies have aimed to biomechanically improve the transosseous tunnel technique of rotator cuff repair. However, no previous work has addressed tunnel inclination at the time of surgery as an influence on the strength of the repair construct.
Hypothesis:
We hypothesized that the tunnel angle and entry point would influence the biomechanical strength of the transosseous tunnel in rotator cuff repair. Additionally, we investigated how tunnel length and bone quality affect the strength of the repair construct.
Study Design:
Controlled laboratory study.
Methods:
Mechanical testing was performed on 10 cadaveric humeri. Variations in the bone tunnel angle were imposed in the supraspinatus footprint to create lateral tunnels with inclinations of 30°, 45°, and 90° relative to the longitudinal axis of the humeral shaft. A closed loop of suture was passed through the bone tunnel, and cyclic loading was applied until failure of the construct. Load to failure and distance between entry points were the dependent variables. Analysis of variance, post hoc paired t tests, and the Bonferroni correction were used to analyze the relationship between the tunnel angle and failure load. The Pearson correlation coefficient was then used to evaluate the correlation of the distance between entry points to the ultimate failure load, and t tests were used to compare failure loads between healthy and osteoporotic bone.
Results:
Tunnels drilled perpendicularly to the longitudinal axis (90°) achieved the highest mean failure load (167.51 ± 48.35 N). However, there were no significant differences in the failure load among the 3 tested inclinations. Tunnels drilled perpendicularly to the longitudinal axis (90°) measured 13.86 ± 1.35 mm between entry points and were significantly longer (P = .03) than the tunnels drilled at 30° and 45°. We found no correlation of the distance between entry points and the ultimate failure load. Within the scope of this study, we could not identify a significant effect of bone quality on failure load.
Conclusion:
The tunnel angle does not influence the strength of the bone-suture interface in the transosseous rotator cuff repair construct.
Clinical Relevance:
The transosseous technique has gained popularity in recent years, given its arthroscopic use. These findings suggest that surgeons should not focus on the tunnel angle as they seek to maximize repair strength.
The transosseous suture technique is one of the original approaches to rotator cuff repair. 9,25 As the incidence of rotator cuff repairs increased, 37,40 various surgical approaches were developed and modified. 8,40 The evolution continued with the single-row suture anchor method. 22,24,38 Later, the double-row approach gained popularity, as it was found to better reproduce the original footprint. 10,22,24,26,38 Transosseous-equivalent suture anchor repair was developed to increase contact between the tendon and footprint in a similar fashion to traditional transosseous repair. 22,31,38 The arthroscopic approach to these techniques became popular because it is functionally equivalent to open and semi-open techniques 5,7,10,35 and results in fewer surgical site infections. 39 A cohort study comparing the aforementioned techniques found the lowest retear rate in the transosseous-equivalent repair group. 27 Despite these advancements, rotator cuff retears, causing pain, muscle weakness, and decreased range of motion, 28 remain relatively common. 17,19
To decrease retear rates, 21 anchor pullout, and operative costs, 3,13,36 while improving tendon-footprint healing, 20,32 an arthroscopic transosseous repair method was recently developed. Via this procedure, bone bridges are created arthroscopically using intersecting transosseous tunnels, with the medial tunnels directly adjacent to the articular surface of the humerus 14,20,34 and the lateral tunnels approximately 1.5 cm below the superior tip of the greater tuberosity. 4,13
The advantages of transosseous techniques over single-row and double-row suture anchor methods are increased circumferential pressure and contact between the tendon and footprint, which are important considerations in tendon healing. 13,30 A number of biomechanical studies have found similar pullout strength and stability between suture anchors and transosseous tunnels. 14,16,20,33,36 Furthermore, the arthroscopic transosseous tunnel technique is more economical because of the absence of anchors and is similar to anchor-based transosseous-equivalent repair in terms of surgical time. 3,20 Transosseous repair have also demonstrated good postoperative outcomes in recent clinical studies. 4,11,21
The tendon, bone, and sutures are the documented failure sites of transosseous tunnels in rotator cuff repair. 4,16,18,20,34,41 Augmentation methods addressing these issues have been proposed. Caldwell et al 6 found improved ultimate failure loads in cadaveric humeri by augmenting the dimensions and bone-suture interface of the bone bridge. In a study by Hinse et al, 18 transosseous tunnels with braided suture tape achieved biomechanical properties that were not significantly different from a double-row anchor construct. These studies, however, did not address tunnel inclinations.
Considering that transosseous construct failures at the bone are well documented, 16,34,41 the aim of the present study was to identify the tunnel angle that can strengthen the bone-suture interface. We hypothesized that the tunnel angle would influence the biomechanical performance of the transosseous tunnel. Additionally, we sought to determine whether tunnel length and bone condition affect this association.
Methods
Specimens
Cadaveric specimens were obtained from Science Care. An institutional review board was consulted, and approval for the use of human tissues was not required. Mechanical testing was performed on 10 unpaired humeri randomly harvested from freshly frozen cadaveric specimens with a mean age of 76.1 ± 17.3 years, mean weight of 138.3 ± 30.1 lb, and mean height of 65.6 ± 7.6 inches. There were an equal number of male and female specimens. Before instrumentation, the specimens were cleaned of the surrounding soft tissues to properly identify failure locations during testing. After testing, each specimen was sectioned along the planes passing through the bone tunnels. Bone quality was estimated by an experienced orthopaedic surgeon (A. P.) based on visual inspection of the density and thickness of trabeculae in the sections. 23
Surgical Technique
The variations in the bone tunnel angle were imposed with a goniometer (Figure 1), following the surgical technique of the ArthroTunneler instrument (Tornier). Three configurations were re-created within each supraspinatus footprint. To avoid interference between the tunnels, tunnel sites were marked at the entry points. Then, tunnel sites were randomized among the 3 configurations. The tunnels were drilled using a 2.9-mm drill bit with lateral tunnel inclinations of 30°, 45°, and 90° in relation to the long axis of the humeral shaft. Nonabsorbable, high–tensile strength No. 2 sutures were passed through the tunnels and knotted firmly, forming a closed loop of approximately 150 mm.
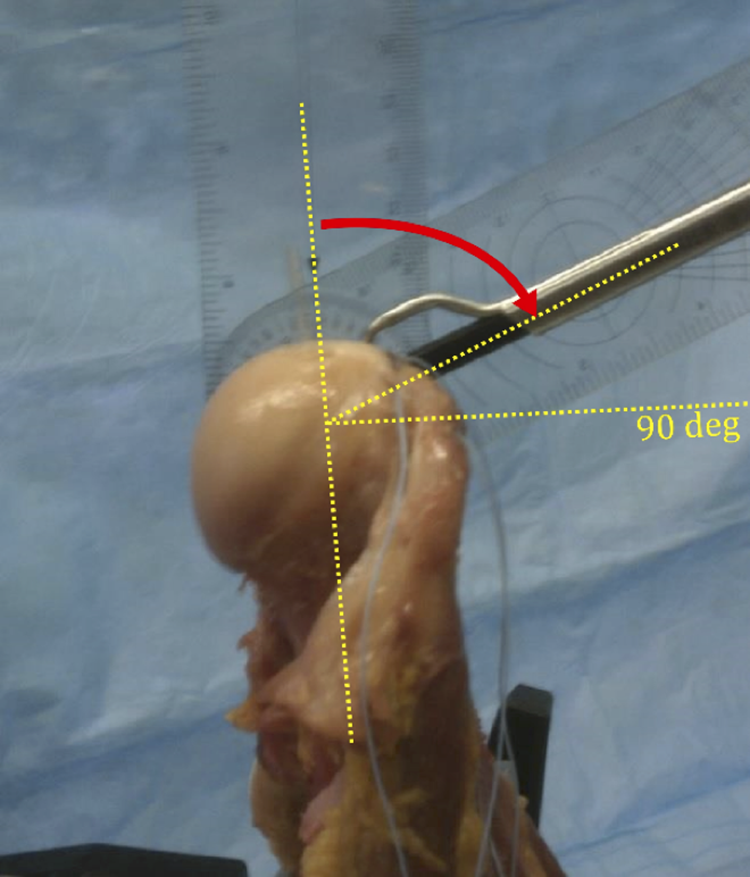
Reference for the measurement of tunnel inclinations considered in the current study.
Experimental Testing
Because we focused on the bone-suture interface rather than the complete repair construct, bone tunnels were tested individually. To ensure the absence of rigid rotation due to the applied load, the humeri were cut at the proximal one-third of their lengths and fixed to the mechanical testing machine with 2 stainless steel rods 5 mm in diameter. After instrumentation and before testing, the distance between tunnel entry points was measured using a digital caliper (500 caliper; Mitutoyo). This distance was proportional to the tunnel length, given the fixed angle of intersection created by the tunneling device. Therefore, it was selected as a substitute for tunnel length. The specimens were mounted in the mechanical testing machine (Instron). The vector of pull was aligned with the simulated line of pull of the supraspinatus at 45° of thoracohumeral abduction (Figure 2). This angle is associated with the maximal load exerted by the supraspinatus. 15 The closed loop formed with the suture was pulled through a metal chain attached to the testing machine.
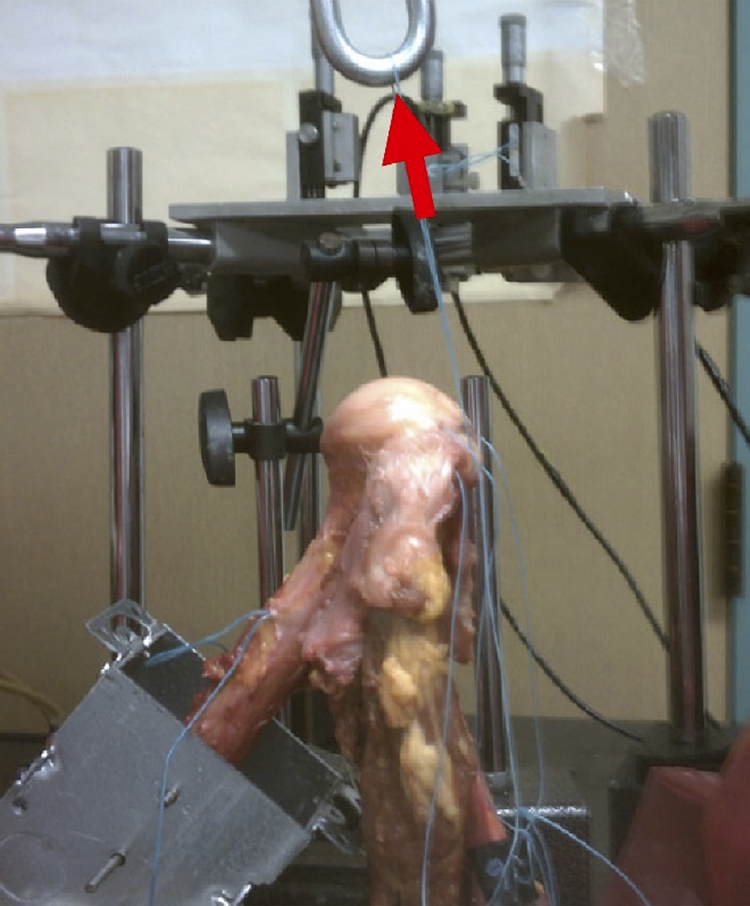
Experimental setup illustrating the load direction (arrow). Specimen fixation was performed in relation to the shown magnetic holders used as a reference for the mechanical testing frame.
A multistep loading method was used to test the construct load to failure. The construct was subjected to sets of 50 cycles. During each set, it was loaded from a base load of 25 N to a reference load. A reference load of 75 N was chosen for the first set of 50 cycles because it approximates the average force produced by the supraspinatus to support the weight of the arm and to stabilize the joint. 15 The reference load was increased by 25 N for each following set of 50 cycles. Cyclic displacement was applied at a rate of 5 mm/min. Load-displacement data were recorded at a frequency of 100 Hz and at 5-N load increments. Maximal load to failure was used to evaluate the mechanical performance of the 3 configurations.
Statistical Analysis
The failure load and distance between entry points were analyzed in R version 3.4.0 (R Foundation for Statistical Computing) for normality using the Shapiro-Wilk test. Differences in the failure load and distance between entry points among the 3 experimental angles were then analyzed using repeated-measures analysis of variance (ANOVA). ANOVAs that resulted in a significant difference were evaluated with post hoc paired t tests and the Bonferroni correction. The distance between entry points and ultimate failure load were evaluated using the Pearson correlation coefficient. The influence of the anatomic bone condition on the ultimate failure load was analyzed by comparing the failure loads between healthy and osteoporotic groups for each experimental angle using t tests. Statistical significance was set at P ≤ .05.
Results
Based on the evaluation of cadaveric shoulder specimens, 43% were classified as osteoporotic. The degree of osteoporotic changes ranged from moderate to severe.
The distance between entry points and failure load were normally distributed (P > .065). Therefore, parametric tests were used. Repeated-measures ANOVA highlighted differences in the distance between entry points (P < .01) and failure load (P = .05) among the 3 insertion angles.
The tunnels drilled perpendicularly to the longitudinal axis (90°) measured 13.86 ± 1.35 mm between entry points. This distance between entry points was significantly greater (P = .03) than the distance for tunnels drilled at 30° and 45°. These were not significantly different from each other (P = .99) and measured 7.29 ± 1.13 mm and 6.79 ± 1.88 mm, respectively (Figure 3). The highest mean failure load (167.51 ± 48.35 N) was achieved with tunnels drilled perpendicularly to the longitudinal axis (90°). Tunnels with 30° and 45° inclinations achieved mean failure loads of 137.90 ± 71.44 N and 104.88 ± 57.85 N, respectively (Figure 4). However, in light of the Bonferroni correction, these differences in the failure load were not statistically significant. Given the subjective methods used for bone quality classification and within the limits of this study, we could not identify a significant effect of bone quality on failure load, with P ≥ .38 (Table 1).
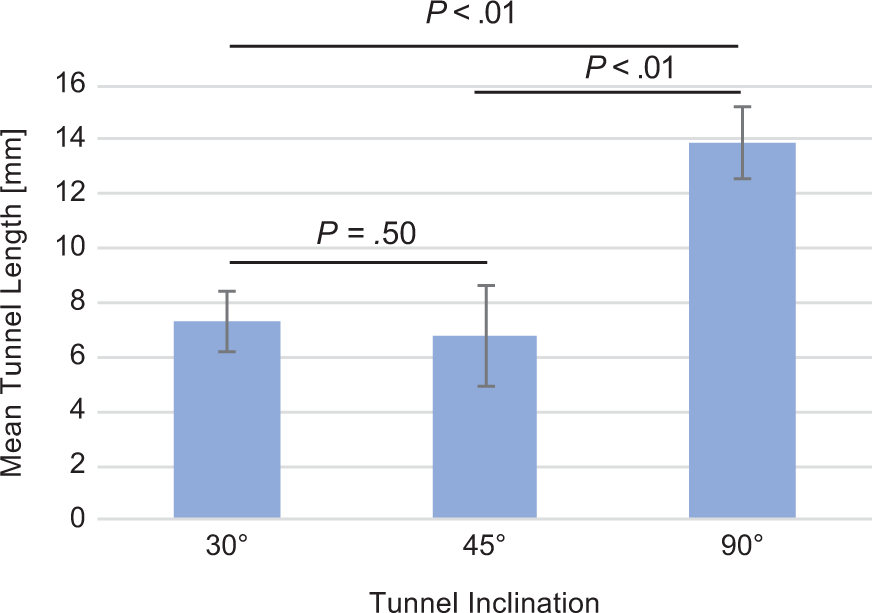
Mean distances between entry points and P values corrected using the Bonferroni correction for all tested humeri.

Mean loads to failure. P values corrected using the Bonferroni correction for all tested humeri.
Failure Loads for Each of the Tested Tunnel Inclinations for Healthy and Osteoporotic Bone a

a Data are reported as mean ± SD unless otherwise indicated.
bP value refers to the variability between healthy and osteoporotic bone.
Most of the failures occurred by suture breakage at the superior part of the lateral tunnel entry point, where cortical bone interfaced with the suture. Suture pullout through bone accounted for the remaining failures and was observed in 2 tests at 30° and 1 test at 90°.
The differences in failure loads also resulted in differences in the number of cycles to failure, which ranged from 268 ± 109 for 90° to a minimum of 146 ± 120 for 45°. The relationship of the distance between entry points and load to failure was poorly represented by a linear function, producing a Pearson correlation coefficient of 0.315 (Figure 5).

Plot comparing load to failure and distance between entry points. Applying a linear function produced a determination coefficient of 0.0918.
Discussion
Transosseous techniques are regaining popularity. They result in good postoperative scores 4,11,21 and now benefit from the lower infection risk associated with an arthroscopic approach. 39
A follow-up study of 109 arthroscopic transosseous repairs found excellent postoperative results at 38 months, with an average American Shoulder and Elbow Surgeons (ASES) score of 94.6 and 4 failures. 11 A study of 31 repairs (including 11 revision procedures) treated with the same technique found an average ASES score of 86.3 and 3 failures at 28 months follow-up. 4
Kummer et al 20 biomechanically compared a 2-tunnel transosseous repair technique to a suture anchor–based transosseous-equivalent technique and found no significant difference in strength. For pectoralis major tendon repair, Hart et al 16 also found no significant difference in strength between a suture anchor construct and a transosseous construct. Salata et al 34 compared a 2-tunnel transosseous construct, created using the same ArthroTunneler instrument utilized in the present study, to a transosseous-equivalent suture anchor construct. Transosseous repair was significantly weaker, with pullout loads of 291.7 ± 57.9 N versus 558.4 ± 122.9 N, respectively. 34 Of the aforementioned studies, none had evaluated the effect of tunnel inclination on the strength of the repair construct.
Previous studies have demonstrated the tendon-suture interface as one of the failure sites of the transosseous construct. 4,18,20 In the present study, we excluded the tendon because of the variable performance among various tendon-suturing techniques. 18,34,38 Rather, we focused on the bone-suture interface. We found no significant differences in failure loads among the tested tunnel inclinations. Failure occurred mostly because of suture breakage at the cortical bone and occasionally because of suture pullout through bone.
We also found that the distance between entry points is significantly greater for tunnels at 90° compared with 30° and 45°. This could have been interpreted as an influence of the distance between entry points on the failure load. We investigated the isolated relationship between the pullout load and distance between entry points and found a poor correlation. The increment in the failure load is independent of the distance between entry points.
In our study, we could not identify a significant effect of bone quality on pullout strength. Further studies might be needed to assess bone quality as described by Pietschmann et al, 33 in which the authors objectively measured bone quality and found significantly lower pullout loads in osteoporotic bone. Additionally, they tested a transosseous configuration that is drastically different from the bone tunnels used in our study. 33
The present study was not without other limitations, including a limited sample size. We utilized 10 specimens for a total of 30 tunnels. A limited comparison of our results can be made. Failure loads for a complete repair construct found by Salata et al 34 using similar tunneling methods are comparable with our results, considering that we tested single tunnels. Additionally, reproducibility of the tunnel inclinations was limited to ±2.5°, as determined by goniometer increments. However, this is equivalent to what is done in surgical practice. 1,2 Finally, we did not measure lengthening to failure because it would require the consideration of permanent deformation of the suture and sliding of the knots. Lengthening to failure is an important mode of construct failure, especially in softer, osteoporotic bone. Such bone quality may allow for greater suture lengthening via suture cutout.
It appears that physiological forces required for routine activities may put the transosseous construct at risk in the early postoperative period. A recent work found a peak load of 164 ± 27 N on the supraspinatus tendon for a participant turning a steering wheel while driving. 29 Gerber et al 15 estimated the maximal supraspinatus force required to support the weight of the arm and to stabilize the joint to be 130 N. Given a single-tunnel mean failure load of 121.39 N (for 30° and 45° inclinations) observed in our study, it is clear that transosseous repair strength must be improved to reduce failures. These data also support early postoperative protection of the repair construct.
Authors have proposed various techniques to strengthen the suture-tunnel construct. Caldwell et al 6 found increased ultimate pullout loads with tunnels that were placed farther from each other and with lateral holes placed more distal from the tip of the greater tuberosity. The strength was further increased by 1.9 times with the use of a polyethylene button to augment the suture-tunnel interface. 6 Other authors have used suture buttons subjectively to strengthen bone tunnels, especially in osteoporotic bone, with good postoperative results. 12,14 These results are consistent with our findings that most suture failures occur at the edge of the cortical bone.
In conclusion, based on the present biomechanical study, the tunnel angle does not affect the strength of the bone-suture interface in the transosseous rotator cuff repair construct. This technique is gaining popularity in recent years, given its arthroscopic use. However, based on our findings, we suggest that surgeons should not focus on the tunnel angle as a way to maximize repair strength.
Footnotes
Acknowledgment
The authors thank Alexander Meininger, MD, for assistance with developing the concept of the study and the laboratory experiments.
One or more of the authors has declared the following potential conflict of interest or source of funding: D.B. is a consultant for Smith & Nephew, Exactech, Arthrex, Liberty Surgical, Encore Medical, and Linvatec. B.G. is a consultant for Acumed, Iroko Pharmaceuticals, and Exactech. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.