
Abstract
Background:
The incidence of rotator cuff tears increases with age, and operative management is usually required in patients with persistent symptoms. Although several studies have analyzed the effect of age and comorbidities on outcomes after rotator cuff repair, no study has specifically examined the consequence of frailty.
Purpose:
To determine the best frailty/comorbidity index for predicting functional outcomes after arthroscopic rotator cuff repair.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
The authors conducted a retrospective cohort study of 340 consecutive patients who underwent unilateral arthroscopic rotator cuff repair at a tertiary hospital between April 2016 and April 2018. All patients had undergone arthroscopic double-row rotator cuff repair with subacromial decompression by a single fellowship-trained shoulder surgeon. Patient frailty was measured using the Modified Frailty Index (MFI), Clinical Frailty Scale (CFS), and Charlson Comorbidity Index (CCI), calculated through retrospective chart review based on case notes made just before surgery; patient age and sex were also noted preoperatively. Functional outcomes using the Oxford Shoulder Score (OSS), Constant Shoulder Score (CSS), University of California Los Angeles (UCLA) Shoulder Score, and visual analog scale for pain were measured preoperatively and at 3, 6, 12, and 24 months postoperatively.
Results:
The MFI was a consistent significant predictor in all functional outcome scores up to 24 months postoperatively (P < .05), unlike the CFS and CCI. Sex was also a significant predictor of postoperative OSS, CSS, and UCLA Shoulder Score, with male sex being associated with better functional outcomes. Patients with higher MFI scores had slower functional improvement postoperatively, but they eventually attained functional outcome scores comparable with those of their counterparts with lower MFI scores at 24 months postoperatively.
Conclusion:
The MFI was found to be a better tool for predicting postoperative function than was the CFS or CCI in patients undergoing arthroscopic rotator cuff repair. The study findings suggest that a multidimensional assessment of frailty (including both functional status and comorbidities) is important in determining functional outcomes after arthroscopic rotator cuff repair.
The incidence of rotator cuff tears increases with age 37 and has been mainly attributed to chronic attritional changes as part of the degenerative process of aging. 21 The operative management of rotator cuff tears is usually required in patients with persistent symptoms, despite physical therapy and analgesia. However, older patients often have comorbidities that may impair healing and complicate surgery. 40 They also tend to have more generalized medical issues and shoulder dysfunction, 16 which can adversely affect healing of the repaired tendon. Previous studies have shown a decrease in the healing rate related to advanced age and that impaired healing of the rotator cuff results in poorer functional outcomes after surgery. 6,13,40
Although several studies have analyzed the effect of age and comorbidities on outcomes after rotator cuff repair, no study has specifically examined the consequence of frailty. Frailty is defined as an aging-associated decline in multisystem physiologic reserve and function 44 that gives rise to vulnerability. 19 In general surgery, frailty has been shown to be an independent predictor of mortality 28 and adverse surgical outcomes, including increased postoperative complications and length of hospital stay. 19 The degree of frailty may differ significantly among patients of the same chronologic age, making frailty an important consideration when attempting to analyze the effect of age on postoperative outcomes. 34,39,44 There are currently several scoring systems available to assess frailty, including the Modified Frailty Index (MFI), Clinical Frailty Scale (CFS), and Charlson Comorbidity Index (CCI). However, the correlation and association between these scoring systems and postoperative functional outcomes after arthroscopic rotator cuff repair have yet to be studied.
The aim of this study was to determine the best frailty/comorbidity index for predicting functional outcomes after arthroscopic rotator cuff repair. We hypothesized that the MFI would be a better predictor of postoperative functional outcomes than would the CFS and CCI in patients undergoing arthroscopic rotator cuff repair, as it uses a multidimensional approach that takes into account both the functional independence and the comorbidities of patients.
Methods
Study Design and Patient Cohort
We conducted a retrospective cohort study of consecutive patients who underwent unilateral rotator cuff repair surgery at a tertiary hospital between April 2016 and April 2018. The study was approved by an institutional review board before commencement, with informed consent from all patients. Inclusion criteria were patients aged 21 years or older with a full-thickness supraspinatus tear documented on preoperative shoulder ultrasonography or shoulder magnetic resonance imaging and failure of conservative management. Patients with partial-thickness rotator cuff tears, traumatic tears, isolated subscapularis tears, or concomitant adhesive capsulitis or glenohumeral instability were excluded from this study.
All patients, while under general anesthesia, underwent arthroscopic double-row rotator cuff repair with subacromial decompression by a single fellowship-trained shoulder surgeon (D.T.T.L.). The presence of concomitant long head of the biceps tendon injury was treated with concomitant biceps tenodesis during the surgery. Their surgeries were performed in the beach-chair position using standard posterior, anterior, and lateral arthroscopic portals.
All patients underwent the same standardized and supervised postoperative rehabilitation protocol. They used an arm sling and started pendulum exercises. Use of the sling was discontinued at 4 weeks, and active shoulder range of motion (ROM) was started. Strengthening exercises were started at 8 weeks after surgery.
Outcome Measures
All patients underwent the relevant preoperative investigations including basic laboratory blood tests, electrocardiogram, and chest radiographs. Patient assessment was performed by an independent health care professional preoperatively and at 3, 6, 12, and 24 months postoperatively. Preoperative age, sex, American Society of Anesthesiologists (ASA) status, and presence of concomitant biceps pathology were recorded as predictors for the outcomes. These factors have been shown to be associated with poorer postoperative outcomes in patients undergoing arthroscopic rotator cuff repair. 6,13,16,31,40 Degrees of forward flexion and abduction of the affected shoulder were also measured. The Oxford Shoulder Score (OSS), Constant Shoulder Score (CSS), University of California Los Angeles (UCLA) Shoulder Score, and visual analog scale (VAS) for pain were used to assess patient-reported outcomes.
The OSS is a validated patient-based questionnaire designed to assess the outcome of all shoulder surgeries except for instability surgery. 24 The CSS, developed by Constant and Murley, 11 is a 100-point scale that consists of subjective and objective variables used to assess the function of the shoulder. These are divided into 4 subscales: (1) pain (15 points), (2) activities of daily living (20 points), (3) strength (25 points), and (4) ROM of the shoulder (40 points). The combined total score ranges from 12 to 60, with a higher score indicating a greater degree of disability. The UCLA Shoulder Score 4 is a combined subjective and objective patient survey that assesses 5 main domains: (1) pain, (2) function, (3) active forward flexion, (4) forward flexion strength, and (5) overall satisfaction. The VAS assesses pain in the involved shoulder on a scale ranging from 0 to 10, with 0 points representing no pain at all and 10 points representing the worst pain ever experienced.
Frailty Scores
The frailty indices for each patient were calculated using retrospective chart review based on preoperative case notes just before surgery. The MFI was calculated based on the Canadian Study of Health and Aging Frailty Index and validated using the American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP) database. 20,29 It uses an 11-factor scoring system based on the patient’s past medical history and functional status (Table 1). Scores are calculated by totaling the number of factors present in the patient and dividing the sum by the total number of factors (n/11). 32 Based on the MFI score, the patients were stratified into 5 groups: (1) 0 (0 factors), (2) 0.09 (1 factor), (3) 0.18 (2 factors), (4) 0.27 (3 factors), and (5) ≥0.36 (≥4 factors).
The 11 Factors of the Modified Frailty Index a

a COPD, chronic obstructive pulmonary disease; PCI, percutaneous coronary intervention; PCS, prior cardiac surgery.
The CFS is a descriptive ordinal score ranging from 1 (very fit) to 9 (terminally ill) (Table 2). The score can be further categorized into robust (scores 1-3), prefrail (score 4), and frail (scores 5-9) according to the primary study of Rockwood et al. 30
Clinical Frailty Score a
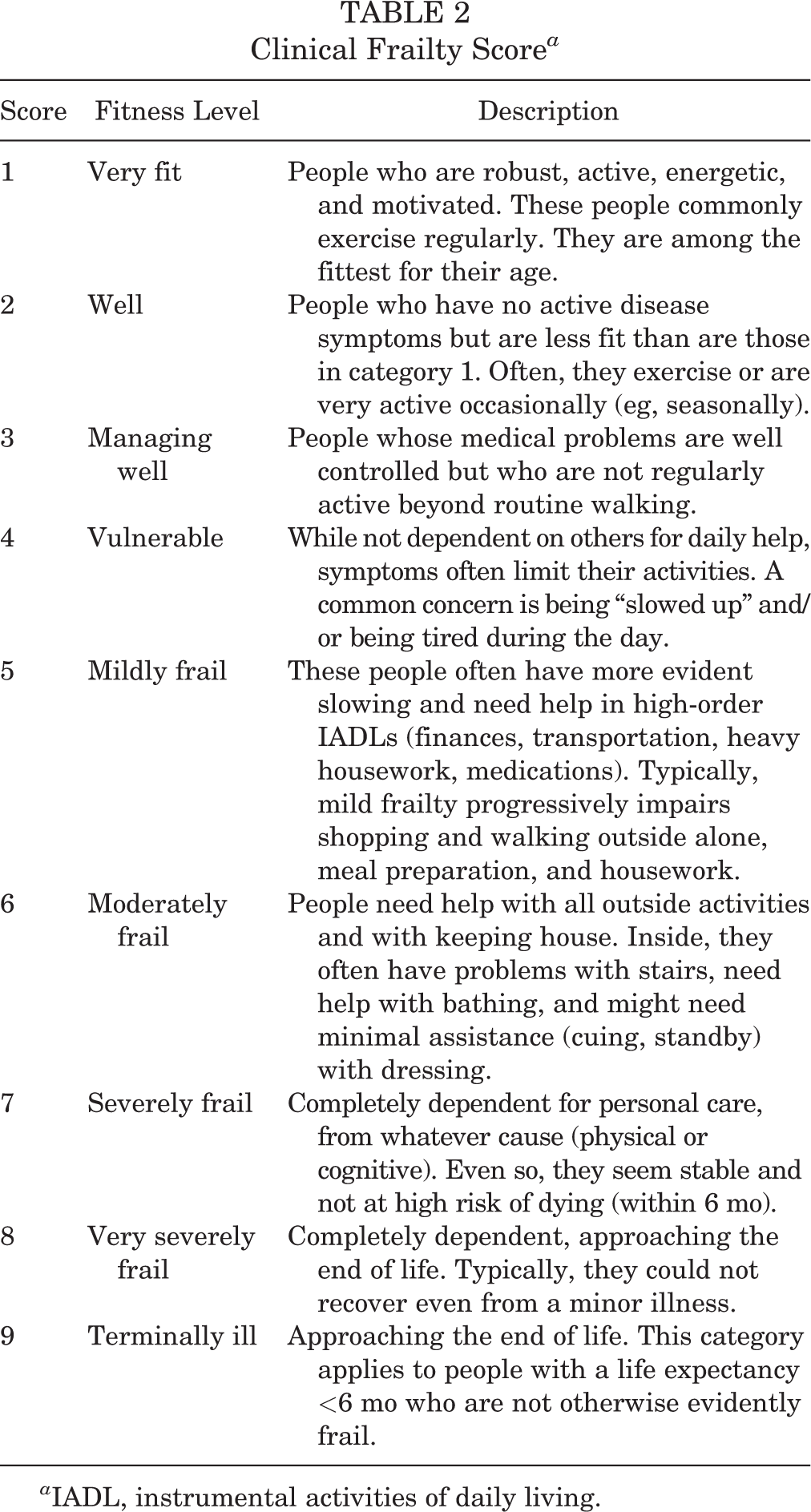
a IADL, instrumental activities of daily living.
The CCI 7 is a frailty scoring system that evaluates the patient base on the presenting comorbidities and was designed to help predict mortality. Each comorbidity is assigned different scores (Table 3) that are summed to obtain the final score. Patients were stratified into 1 of 4 groups based on their final CCI score: 0, 1, 2 or ≥3.
Charlson Comorbidity Index

Statistical Analysis
Statistical analysis was carried out using SPSS Version 19.0 (IBM Corp), and the level of significance was taken as α = .05 for all comparisons. One-way analysis of variance or an independent t test was used to analyze continuous variables including age, OSS, CSS, UCLA Shoulder Score, and VAS score, while the Pearson chi-square test was used to analyze categorical variables such as sex, ASA status, and side of surgery.
A linear regression analysis was used to analyze each individual preoperative variable on postoperative functional outcome scores. Covariates with P < .2 in the linear regression were entered into the final multiple linear regression analyses. The number of patients in each MFI group in the present study possessed >99% power with a type 1 error of .05. This analysis confirmed that the present study was adequately powered.
Results
Patient Characteristics
From the electronic medical record, there were 340 cases of arthroscopic rotator cuff repair between April 2016 and April 2018. The preoperative descriptive data, shoulder characteristics, and outcome scores of the study patients are shown in Tables 4 to 6. The majority of patients were women (55.3%), and the mean ± standard deviation age of the study group was 58.5 ± 11.6 years. Patients who had a higher MFI tended to be older and have a higher ASA status; lower ROM; and lower OSS, CSS, UCLA Shoulder Score, and VAS score preoperatively. Patients who were more frail based on CFS scoring tended to be older and have a higher ASA status, lower OSS, and lower UCLA Shoulder Score preoperatively. There was no significant difference in characteristics among the CCI groups. No patient died, and all patients completed follow-up.
Preoperative Characteristics of the Study Patients by Frailty and Comorbidity Scores a
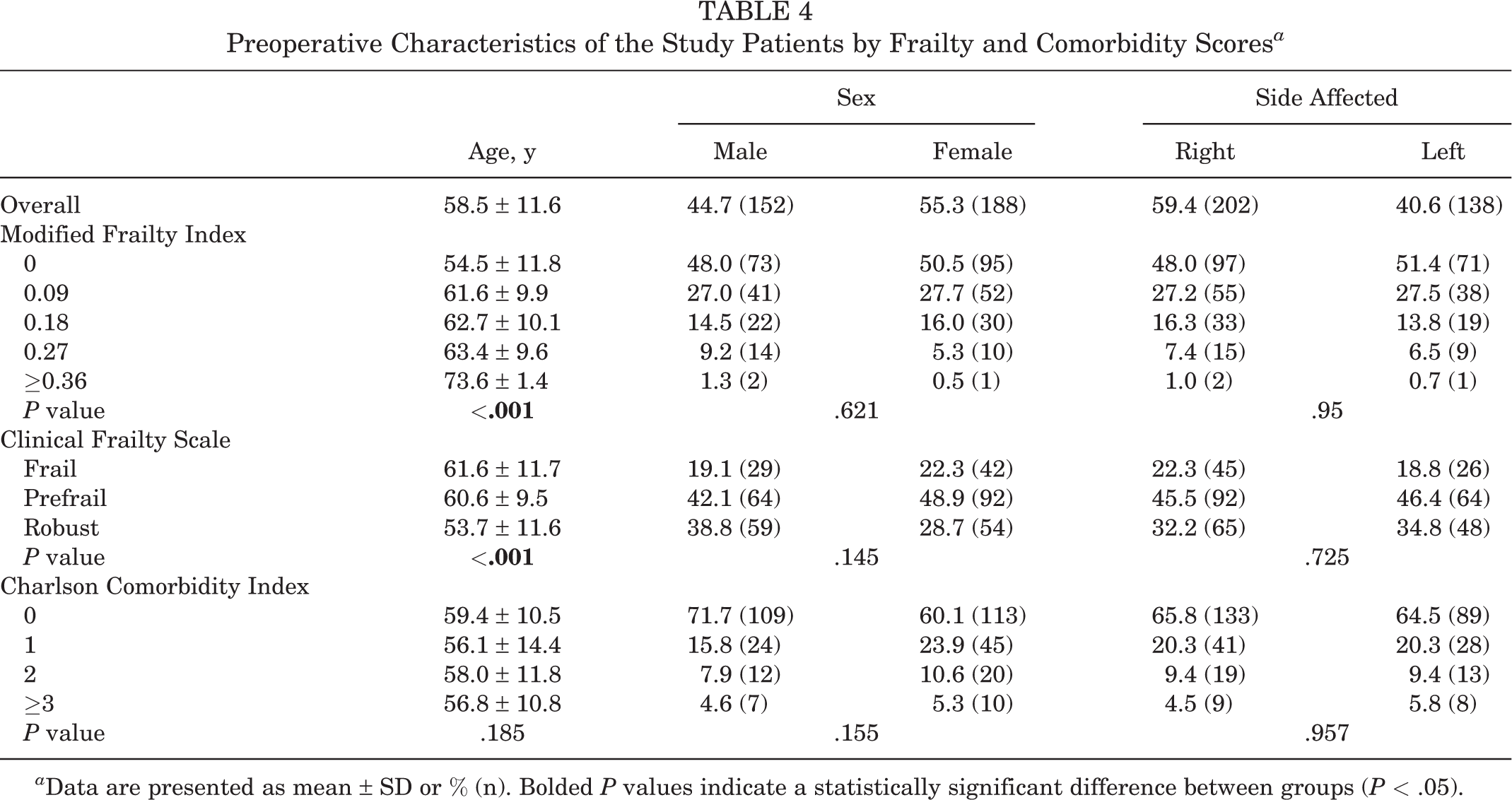
a Data are presented as mean ± SD or % (n). Bolded P values indicate a statistically significant difference between groups (P < .05).
Preoperative Shoulder Characteristics and ASA Status of the Study Patients by Frailty and Comorbidity Scores a

a Data are presented as mean ± SD or % (n). Bolded P values indicate a statistically significant difference between groups (P < .05). ASA, American Society of Anesthesiologists.
Preoperative Outcome Scores of Study Patients by Frailty and Comorbidity Scores a

a Data are presented as mean ± SD. Bolded P values indicate a statistically significant difference between groups (P < .05). CSS, Constant Shoulder Score; OSS, Oxford Shoulder Score; UCLA, University of California Los Angeles; VAS, visual analog scale for pain.
Predictors of Postoperative Functional Outcomes
The multiple linear regression analyses of significant predictors of functional outcomes are presented in Table 7. The MFI was a consistent significant predictor in all functional outcome scores up to 24 months postoperatively. The CFS was significant only in predicting the 1-year CSS, UCLA Shoulder Score, and VAS score. Furthermore, the unstandardized beta coefficient of the CFS showed lower association when compared with the MFI. The CCI was not a significant predictor in any of the multiple linear regression models. Sex was also significant in predicting postoperative OSS, CSS, and UCLA Shoulder Score functional outcome scores, with male sex noted to be associated with better functional outcomes. Age and ASA class were generally not significant in predicting postoperative functional outcome scores up to 24 months after arthroscopic rotator cuff repair.
Multiple Linear Regression Analysis of Predictive Factors on the Postoperative Functional Outcome Scores a

a Bolded values indicate statistical significance (P < .05). Dashes indicate independent variables with P > .2 in the single linear regression that were omitted from the multiple linear regression model. ASA, American Society of Anesthesiologists; CCI, Charlson Comorbidity Index; CFS, Clinical Frailty Scale; CSS, Constant Shoulder Score; MFI, Modified Frailty Index; OSS, Oxford Shoulder Score; UCLA, University of California Los Angeles; VAS, visual analog scale for pain.
When postoperative functional scores were compared across the 5 MFI groups (Table 8), there were significant differences among the groups at 6 and 12 months postoperatively in terms of OSS, CSS, UCLA Shoulder Score, and VAS pain score, with higher MFI scores being associated with poorer outcomes. When postoperative functional scores were compared between men and women (Table 9), there were significant differences between the groups in terms of OSS, CSS, and UCLA Shoulder Score, up to 24 months postoperatively, with male sex being associated with better functional outcomes.
Comparison of Postoperative Functional Scores Across Modified Frailty Index Groups a
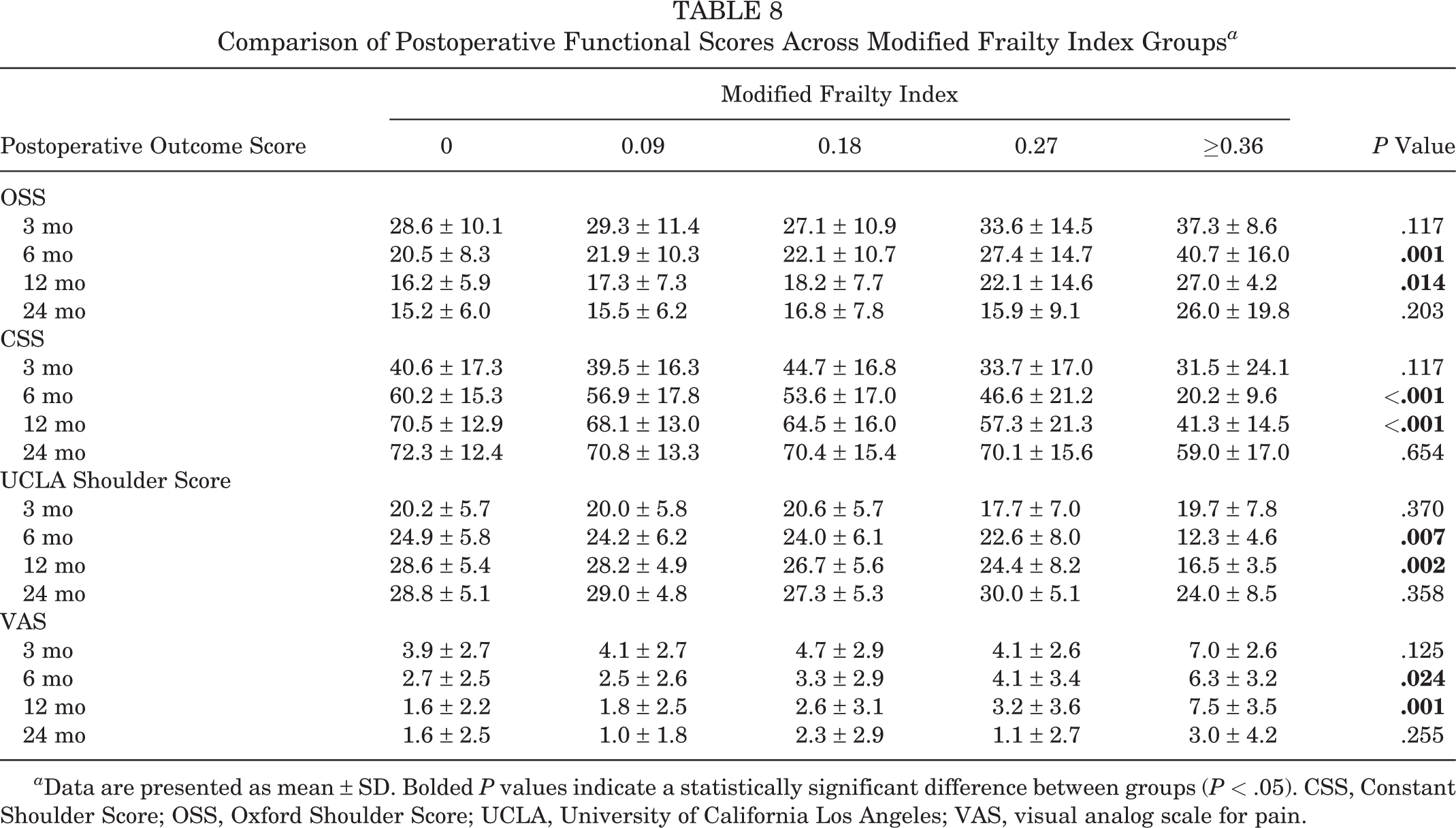
a Data are presented as mean ± SD. Bolded P values indicate a statistically significant difference between groups (P < .05). CSS, Constant Shoulder Score; OSS, Oxford Shoulder Score; UCLA, University of California Los Angeles; VAS, visual analog scale for pain.
Comparison of Postoperative Functional Scores Between Sexes a

a Data are presented as mean ± SD. Bolded P values indicate a statistically significant difference between groups (P < .05). CSS, Constant Shoulder Score; OSS, Oxford Shoulder Score; UCLA, University of California Los Angeles; VAS, visual analog scale for pain.
Discussion
This study was designed to evaluate the 3 frailty and comorbidity scores to identify the best predictor for postoperative functional outcomes after arthroscopic rotator cuff repairs. We found that the MFI was a better predictor for the majority of the postoperative functional outcome scores than were the CFS and CCI, which had low or no significant influence on the postoperative functional outcome scores. Male sex was also noted to be a significant predictor of better long-term functional outcome scores.
One explanation for the main finding in this study is the difference in the approaches among the MFI, CFS, and CCI in quantifying the frailty status of a patient. The MFI uses a multidimensional approach that takes into account both the functional independence and comorbidities of patients. 2 This provides a holistic assessment of a patient’s status and health and is currently recommended by the ACS NSQIP best-practice guidelines for frailty assessment before surgery. 10 Furthermore, the MFI has more categories than does the CCI, which allows for better risk stratification and differentiation of sicker patients with poorer prognosis. In contrast, the CFS uses a disability approach, 2 while the CCI focuses only on the number and type of coexisting medical problems 7 and has fewer categories than does the MFI. In addition, the CCI assigns acquired immunodeficiency syndrome a weighted score of 6, which may be overstating comorbidity if the patient is receiving antiviral treatment. Our present findings suggest the importance of a holistic assessment of frailty and that both functional status and comorbidities of patients play a role in influencing outcomes of rotator cuff repair. Better preoperative functional status and overall health would allow the patient to start postoperative rehabilitation earlier or perform the exercises more effectively, thus allowing better functional recovery and ROM postoperatively. 15 Conversely, poorer preoperative functional status and health would increase recovery time, and frailer patients might take longer to recover. This knowledge will be useful for predicting patient prognosis and individualized counseling on the expected postoperative recovery time.
Our results suggest that advanced age is a poor indicator of postoperative functional outcomes. Recent studies have shown that patients >75 years have excellent postoperative outcomes after arthroscopic rotator cuff repairs, comparable with their younger counterparts. 26,42 Frailty, as measured using the MFI, was a much stronger predictor of functional outcomes after rotator cuff repair. Given this, the MFI appears to be a better risk stratification tool than is chronologic age. This is consistent with the findings of recent studies demonstrating the effectiveness of the MFI in risk-stratifying patients undergoing surgery for femoral neck fractures 25 or distal radial fractures, 41 spine surgery, 3 and total hip and knee arthroplasty. 5
Traven et al 38 found that the 5-factor MFI was a significant predictor of medical complications, hospital admission, length of stay, discharge to a rehabilitation facility, and mortality after arthroscopic rotator cuff repair. However, the study did not consider any functional outcomes of rotator cuff repair, which is crucial for patient satisfaction and quality of life after surgery. 36 Furthermore, the 5-factor MFI only accounts for 5 of the comorbidities from the original MFI score: diabetes mellitus, hypertension requiring medication, chronic obstructive pulmonary disease, congestive heart failure, and functional status 2 (not independent). 35 A study by Holzgrefe et al 18 of 9861 patients aged 50 years or older undergoing total shoulder arthroplasty also found that the MFI was an effective risk-stratifying tool that predicted postoperative complications, readmission, reoperation, and adverse hospital discharge, further supporting the use of the MFI in predicting outcomes after shoulder surgery.
However, there remains a paucity in literature on risk stratification of patients undergoing arthroscopic rotator cuff repair. Advanced age and larger number of medical comorbidities have been shown to predict complications after arthroscopic rotator cuff repair, 33 leading authors to conclude that patient factors and preoperative status are more important in risk stratification. 17,33 To our knowledge, the present study is the first to evaluate the association between key frailty/comorbidity scores and postoperative functional outcomes of patients undergoing arthroscopic rotator cuff repair.
Furthermore, the differences in each of the functional scores among the MFI groups were generally greater than the minimal clinically important difference at 12 and 24 months postsurgery. The minimal clinically important differences of the OSS, CSS, and UCLA Shoulder Score were taken as 3.3, 6.7, and 3.0, respectively, at 12 months and 2.7, 6.3, and 2.9, respectively, at 24 months. 43 As such, stratifying patients based on MFI scores and predicting postoperative functional outcome using MFI scores is clinically significant and relevant.
However, the differences in functional outcome scores using the MFI disappeared at 24 months of follow-up. This finding suggests that the patients with high MFI scores ultimately attained functional outcomes comparable with those of their counterparts with low MFI scores, but they just took longer to achieve those results. Patient-related factors such as diabetes mellitus and other comorbidities (as taken into account by the MFI) have been shown to affect the rate of tendon healing and rehabilitation after arthroscopic rotator cuff repairs. 1
In the present study, male sex was also a significant predictor of better long-term functional outcome scores and ROM after rotator cuff repair. This is consistent with the findings of recent studies that have reported sex-associated differences in outcomes of arthroscopic rotator cuff repair. 9,22 In a prospective study of 78 patients who underwent repair of full-thickness rotator cuff tear, Oh et al 22 also found that male sex was associated with better postoperative functional outcomes and recovery in terms of Simple Shoulder Test scores. Similarly, Cho et al 9 found that men had less pain and faster recovery of the shoulder than did women during the early postoperative period after rotator cuff repair. Women had higher postoperative VAS pain scores and significantly lower forward flexion and external rotation than did men at early follow-up. The authors suggested that this observation was likely because women have a lower pain threshold and less tolerance for postoperative pain than do men. 14,27 Appropriate postoperative pain management for patients undergoing rotator cuff repair is considered a major issue that can influence the effectiveness of treatment and rehabilitation in the early postoperative period. 8,23 Furthermore, it is an important factor influencing postoperative satisfaction with rotator cuff repair. 9
The present study has strengths. First, the data represent patients on whom a single surgeon operated, thus reducing heterogeneity in surgical technique and postoperative rehabilitation. Second, our robust follow-up protocol allowed for serial measurement of functional outcome scores at fixed intervals postoperatively.
However, this study also has several limitations. First, there are inherent selection and observer biases, as the data represent patients from a single tertiary institution. Second, the scoring of the CFS in this study does not represent how the score would be used in actual practice, where it would be assessed by a health care professional in contact with the patient. Nonetheless, it has been suggested that a retrospectively assigned CFS score based on medical chart review could be reliable if the necessary components of the score are present in the charts. 12 The present study also did not parse out specific factors from the frailty scores or consider the severity or control of the comorbidities, which could have also influenced postoperative functional outcomes. Third, this study is also limited by the small number of patients in the higher frailty groups.
Conclusion
This study indicated that the MFI is a better tool for predicting postoperative function than is the CFS or CCI in patients undergoing arthroscopic rotator cuff repair. Patients with higher MFI scores had slower functional improvement postoperatively but eventually attained functional outcome scores comparable with those of their counterparts with lower MFI scores at 24 months postoperatively. The findings from our study suggest that a multidimensional assessment of frailty (including both functional status and comorbidities) is important in determining functional outcomes after arthroscopic rotator cuff repair.
Footnotes
Final revision submitted January 29, 2021; accepted February 25, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: This work was supported by an Academic Medicine Research Grant (AM/TP005/2018 [SRDUKAMR18T5] to B.F.H.A.). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the SingHealth Centralised Institutional Review Board (ref. CIRB 2019/2777).