
Abstract
Background:
Studies have reported that opening wedge high tibial osteotomy (OWHTO) without bone grafting has outcomes that are similar to or even better than those of OWHTO with bone grafting, especially after use of a locking plate. However, a consensus on managing the gap after OWHTO has not been established.
Purpose:
To determine the degree of gap healing achieved without bone grafting, the factors associated with gap healing, and whether additional gap healing would be obtained after plate removal.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
This retrospective study included 73 patients who underwent OWHTO without bone grafting between 2015 and 2018. Patients in the study were divided into 2 groups based on the correction angle: small correction group (<10°; SC group) and large correction group (≥10°; LC group). The locking plate used in OWHTO was removed at a mean of 13.5 months after surgery in 65 patients. Radiographic indexes were measured: gap filling height, gap vacancy ratio (GVR), and osteotomy filling index. The acceptable gap healing was defined as an osteotomy filling index ≥3. The factors related to gap healing around the osteotomy site were selected after multicollinearity analysis.
Results:
Although both groups achieved acceptable gap healing regardless of the correction angle, the SC group showed higher and earlier gap healing than did the LC group (gap healing rate 81.4% in the SC group vs 41.7% in the LC group at 3 months postoperatively). The GVR was 8.6% in the SC group and 15.3% in the LC group at 12 months after surgery (P = .005). Both the amount of time that elapsed after surgery and the correction angle were associated with gap healing (P < .05). Additional gap healing was observed after plate removal, as the GVR decreased 2.7% more in the patients with plate removal than in patients who did not have plate removal (P = .012).
Conclusion:
All patients achieved acceptable gap healing without bone graft. The degree of gap healing was higher in the SC group and increased over time. Gap healing was promoted after plate removal. Considering the results of this study, a bone graft is not necessary in routine OWHTO in terms of gap healing.
Medial opening wedge high tibial osteotomy (OWHTO) is a reliable treatment option for medial compartment osteoarthritis with varus deformity in relatively young patients. 3,11,17,20 Because the osteotomy gap is related to complications such as loss of correction, it is important to manage the gap appropriately. 3 Autograft is considered the most effective graft for gap healing, 8,16,24 but autograft can cause additional morbidities at the donor site. Some surgeons prefer to use allograft, but it has theoretical risks of disease transmission and immunologic reaction. The use of bone substitutes adds cost, and there have been reports of delayed union or nonunion. 8,11,20 Because studies have reported successful gap healing without the use of grafts, 5,25 there is doubt about whether bone graft is necessary. Lansdaal et al 10 reported that bone grafts were not required if the amount of correction was <10°. A previous study 18 also reported that a no-graft group showed better clinical outcome than a graft group, and studies have shown that the bone substitute may interfere with natural bone healing. 16,18 Therefore, no consensus exists regarding the method of managing the osteotomy gap after OWHTO.
Several factors have been identified as affecting the degree of gap healing after OWHTO. Smoking, obesity, lateral hinge fracture, and large correction are considered to adversely affect gap healing. 6,13,21,22 However, for some factors such as smoking and obesity, their effects on gap healing after OWHTO are controversial. 6
Although improved fixation strength of the locking plate has reduced concern about loss of correction after OWHTO, it is possible that excessive fixation strength can interfere with bone healing. 1,2,15,19 If sufficient gap healing does not occur because of the excessive fixation strength of the locking plate, plate removal may be unnecessarily delayed. In contrast, if additional bone healing could occur by removing the locking plate, it could be removed without concern about correction loss. However, no study has reported whether additional bone healing occurs after removal of the plate.
The purpose of this study was to determine the degree of gap healing without bone grafting and to determine the factors associated with gap healing. We also wanted to determine whether additional gap healing would be obtained after plate removal. We hypothesized that acceptable gap healing could occur without bone grafting in OWHTO and that the degree of gap healing would be better with a smaller correction angle. We also hypothesized that factors such as smoking, obesity, and lateral hinge fracture would affect gap healing. Finally, we hypothesized that additional gap healing could occur in the medial void after removal of the locking plate.
Methods
Study Design and Population
This retrospective study included 86 patients who underwent OWHTO without bone grafting between 2015 and 2018. Institutional review board approval was obtained before pursuing the retrospective review of data; the need for informed consent was waived because of the retrospective study design. Inclusion criteria were (1) medial compartment osteoarthritis with pain that did not respond to nonoperative treatment and (2) varus alignment of the lower limb (mechanical axis of the lower limb ≥5° varus and medial proximal tibial angle <90°). Exclusion criteria were (1) medial compartment osteoarthritis with bone attrition (Ahlbäck grade ≥3), (2) severe varus alignment of the lower limb (mechanical axis of the lower limb >15° varus), (3) patellofemoral joint or lateral compartment arthritis (Kellgren-Lawrence grade ≥3), (4) flexion contracture ≥15° or further flexion ≤90°, and (5) rheumatoid arthritis. After we excluded 13 patients according to the criteria, 73 patients were ultimately included in the study (Figure 1).

Selection of the patients for study. OWHTO, open wedge high tibial osteotomy.
Patients were divided into 2 groups according to the criteria used in a previous study 4 : a group with a small correction (SC group), defined as a correction angle <10°, and a group with a large correction (LC group), defined as a correction angle ≥10°. No significant differences were seen in baseline characteristics between the 2 groups except for mean age and body mass index (BMI) (Table 1).
Descriptive and Radiographic Data a

a Data are reported as mean ± SD unless otherwise indicated. Bolded P values indicate statistically significant difference between groups (P < .05). LC, large correction (≥10°); SC, small correction (<10°). Obesity was defined as body mass index was more than 30.
b Chi-square test.
c Mann-Whitney test.
Surgical Procedure and Follow-up
Full-limb standing anteroposterior radiographs were used to make preoperative plans and measure postoperative radiographic outcomes. The target or Fugisawa point was 62.5% from the medial side of the joint. Before osteotomy, all patients were evaluated via arthroscopy to assess for associated pathologies. About 4 cm below the knee joint line, a longitudinal incision was made at the anteromedial side of the proximal tibia. The pes anserinus was retracted, and the superficial medial collateral ligament was detached at the distal portion. Guidewires were inserted toward the tip of the fibular head. After the neurovascular bundles were protected using a blunt retractor, biplanar osteotomy was performed. Valgus force was applied gradually using 3 chisel techniques to achieve the target point. After the target correction angle was achieved, the osteotomy site was fixed using a locking plate (TomoFix; Synthes) without bone grafting. A long-leg splint was applied to all patients until postoperative day 2.
Considering their age, the patients who underwent OWHTO may need further surgical treatment in the future such as total knee arthroplasty. Therefore, after stability around the osteotomy site was assessed, plate removal was recommended for all of the patients. Among the patients, 65 (91.5%) underwent plate removal at a mean of 13.5 months postoperatively. These patients were evaluated at 3 months after plate removal.
Patients were instructed to perform knee range of motion exercises after drain and splint removal. Partial weightbearing was permitted for 6 weeks postoperatively. Patients were instructed to visit the outpatient department at the following intervals: 6 weeks, 3 months, 6 months, and 12 months postoperatively.
Data Collection
Three radiologic indexes were evaluated to assess gap healing: gap filling height (GFH) (Figure 2A), gap vacancy ratio (GVR) (Figure 2B), and osteotomy filling index (OFI). GFH was defined as the maximal height of the bone filled at the end of the newly filled bone. GVR was defined as the length of the bone defect based on the length of the osteotomy. 19 OFI was evaluated by dividing the total osteotomy length by 20% into 5 zones 4 (Figure 2C).

The 3 radiologic indexes used to assess gap healing. (A) Gap filling height was defined as the maximal height of bone healing (double arrowhead). (B) Gap vacancy ratio was defined as the length of bone defect, a, divided by the length of the osteotomy, b. In the image, c = gap filling height and d = initial opening gap width. (C) Osteotomy filling index, evaluated by dividing the total osteotomy length by 20% into 5 zones.
Gap healing was evaluated on knee anteroposterior radiographs, and acceptable gap healing was considered to be obtained if the OFI was zone ≥3. 4 The initial opening gap width was measured to calculate the ratio of gap healing by comparing it with GFH (termed the GFH ratio). The heights of the zone 3 area from 40% to 60% of the initial opening gap width were calculated by multiplying the initial opening gap width by 0.4 and 0.6, respectively. Lateral hinge fracture was diagnosed when discontinuity or a callus on the lateral cortex of the osteotomy site was found on postoperative conventional radiographs. The incidence of lateral hinge fracture was 23.3%, and there was only 1 case of Takeuchi type 2 fracture in the LC group (Table 1).
To determine interobserver reliability, all radiographic parameters were measured twice at intervals of 2 weeks by 2 orthopaedic surgeons (H.J.P., M.J.C.) who were blinded to the data of each other. For intraobserver reliability, 1 orthopaedic surgeon (H.J.P.) measured twice at an interval of 2 weeks.
Statistical Analysis
The independent-samples t test and Mann-Whitney test were used to compare the mean values of demographic data between the 2 groups. The Wilcoxon signed rank test and repeated-measures analysis of variance were used to determine whether additional gap healing would be obtained after removal of the locking plate. A generalized estimating equation was used to analyze the factors related to gap healing. After considering multicollinearity, we selected correction angle, BMI, smoking, lateral hinge fracture, and passage of time as independent variables in the generalized estimating equation.
The reliability of measurements was assessed using the intraclass correlation coefficient. The intraclass correlation coefficients for interobserver and intraobserver reliability for all parameters were >0.8, indicating excellent agreement. The statistical power to compare the gap healing between 2 groups was 0.64, and the statistical power to evaluate the effectiveness of plate removal on gap healing was 0.95. We performed the power analysis after including several variables: not only correction angle but also sex, BMI, time, and lateral hinge fracture. The power analysis was done using NCSS software, and the statistical analysis was performed using SPSS Version 26 (SPSS Inc., IBM Corp). P values of <.05 were considered statistically significant.
Results
The GVRs of the SC and LC groups were 8.6% and 15.3%, respectively, at 12 months postoperatively (P = .005) (Table 2). Although both groups achieved acceptable gap healing regardless of the correction angle, the SC group showed higher and earlier gap healing than did the LC group (Tables 2 and 3). Acceptable gap healing was found in only 22.7% of all patients at 6 weeks postoperatively, and this value increased to 74.6% at 3 months. In the subgroup analysis, although the incidence of acceptable gap healing was lower in the LC group than the SC group at 3 months postoperatively, the LC group also obtained acceptable gap healing at 6 months (Table 3).
Radiographic Indexes for Assessing Gap Healing a
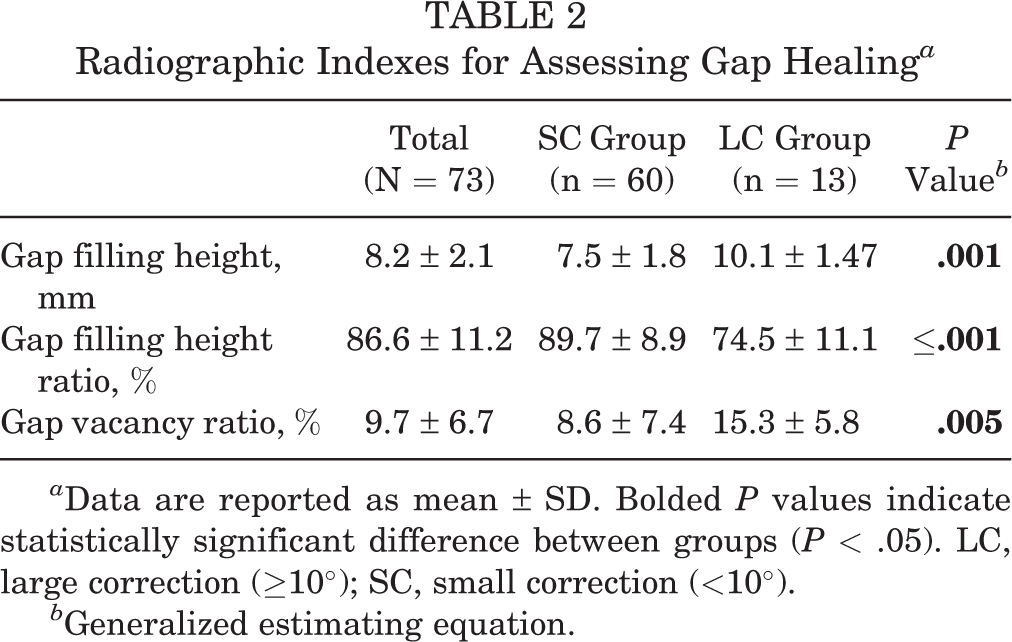
a Data are reported as mean ± SD. Bolded P values indicate statistically significant difference between groups (P < .05). LC, large correction (≥10°); SC, small correction (<10°).
b Generalized estimating equation.
Ratio of Acceptable Gap Healing According to Postoperative Time Point a
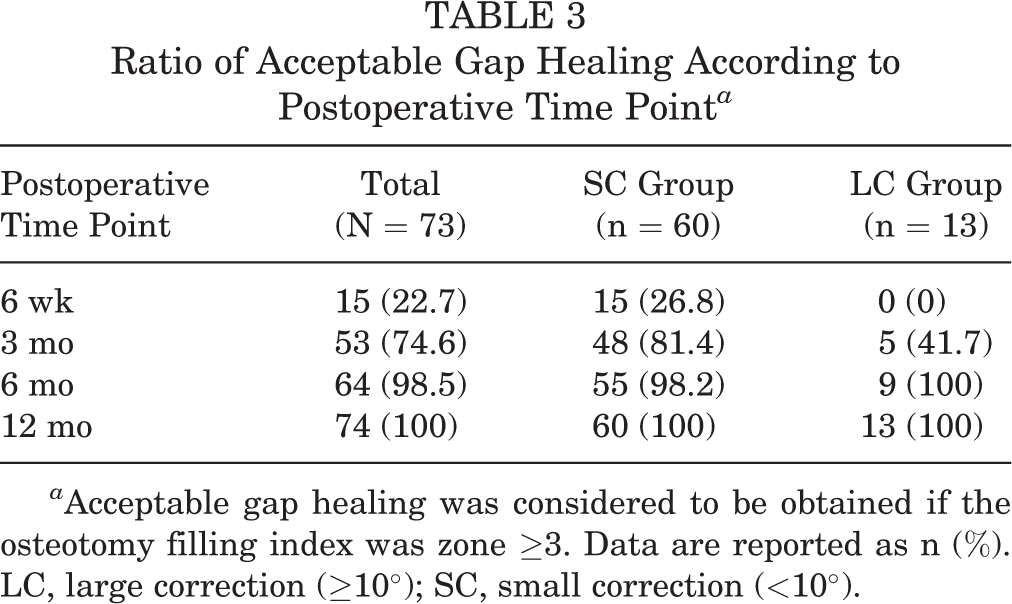
a Acceptable gap healing was considered to be obtained if the osteotomy filling index was zone ≥3. Data are reported as n (%). LC, large correction (≥10°); SC, small correction (<10°).
Time after surgery and correction angle were the only factors associated with gap healing, as indicated by the GFH ratio and GVR. Both the GFH ratio and GVR showed significant time and group × time effects (Table 4). However, smoking, BMI, and lateral hinge fracture did not affect gap healing in our study.
Factors Associated With Gap Healing a

a Bolded P values indicate statistical significance (P < .05).
b Generalized estimating equation.
Additional gap healing was observed in the 65 patients after plate removal. In these patients, the GVR decreased by an additional 2.7% (from 9.1% ± 8.1% to 4.1% ± 6.3%) compared with in those without plate removal (from 10.4% ± 6.0% to 8.1% ± 7.2%) (P = .012) (Table 5).
Radiographic Indexes for Assessing Gap Healing According to Passage of Time and Plate Removal a
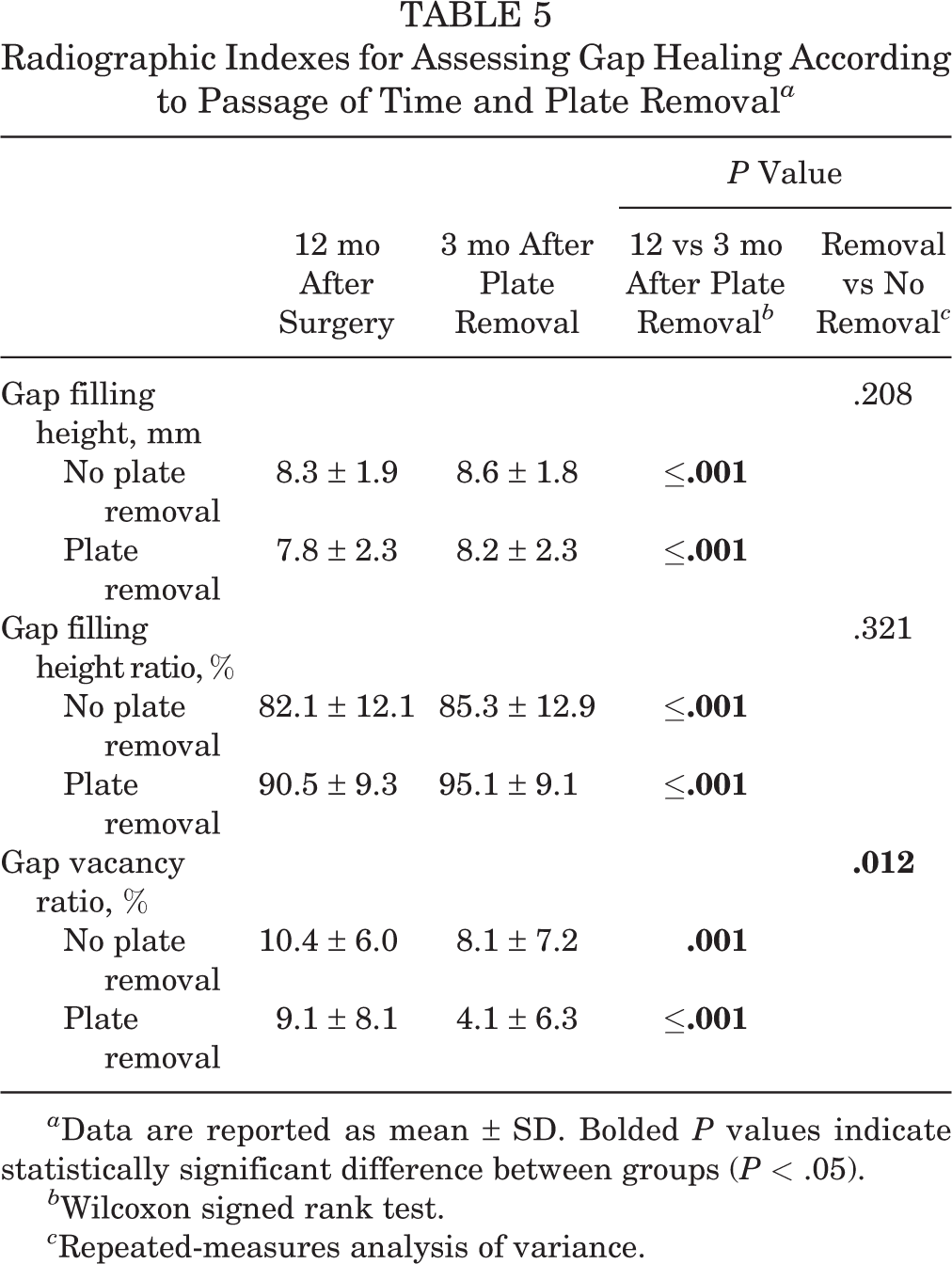
a Data are reported as mean ± SD. Bolded P values indicate statistically significant difference between groups (P < .05).
b Wilcoxon signed rank test.
c Repeated-measures analysis of variance.
Discussion
The principal findings of our study were that all patients obtained acceptable gap healing without bone grafting and that gap healing was greater in the SC group. Furthermore, gap healing was not affected by smoking, obesity, or lateral hinge fracture, but it was promoted by removal of the locking plate.
Our findings confirmed the first part of our hypothesis that acceptable gap healing could be obtained without bone grafting. Brosset et al 4 reported that only 4% (2/51) of patients showed delayed union after OWHTO without bone grafting. Zorzi et al 25 reported that there was no difference in the average times to bone union (bone graft group, 12.4 weeks; no-graft group, 13.7 weeks; P = .13). The results of our study support the findings from the aforementioned investigations. All patients in our study obtained acceptable healing around the osteotomy site. Therefore, considering the complications related to bone grafting, it is reasonable to perform OWHTO without bone grafting in terms of gap healing.
After we compared the degree of gap healing between 2 groups, our findings supported the second part of our hypothesis that gap healing would be promoted if the correction angle were smaller. The time to bone union after OWHTO has previously been reported as 12.4 to 18 weeks. 4,5 Because our study was organized retrospectively, accurate time to bone union could not be assessed. However, we found that 74.6% (53/73) of all patients achieved acceptable gap healing by 3 months postoperatively. Among them, the SC group showed greater acceptable gap healing ratio than the LC group (81.4 % and 41.7%, respectively). Therefore, orthopaedic surgeons should consider the possibility that inadequate gap healing is achieved even at 3 months postoperatively, especially if the correction angle is >10°.
We observed that smoking, BMI, and lateral hinge fracture were not associated with gap healing in our study, contrary to our hypothesis. Smoking and obesity are commonly known factors related to postoperative complications. 12 –14 However, the effect of those factors on gap healing has been controversial. 6 Smoking affects local vasoconstriction, hypoxia on the cellular level, and the process of bone union. For this reason, smoking was considered a relative contraindication to all osteotomies, and OWHTO was not recommended in patients who smoke. 12,23 Obesity has been known to cause delayed healing because it increases motion at the osteotomy site. 14,24 Meidinger et al 13 reported that the rate of obesity (BMI >30) was higher in patients with nonunion than in those with union. However, Floerkemeier et al 6 reported that smoking and obesity did not affect the degree of gap healing at midterm follow-up (mean, 3.6 years). Our findings support the result reported by Floerkemeier et al, which might be explained by 3 factors. The first and most important factor is that the locking plate provided stability around the osteotomy site, 12,23 which in turn provided the appropriate environment for a callus to form. The second factor is that the incidence of smokers (12.3%) and obese patients (21.9%) was lower compared with the incidence in the Meidinger et al study (24.7% and 62.3%, respectively). The third factor is that the patients who were smokers (7/9; 77.8%) and obese (10/16; 62.5%) needed SC in our study. For these reasons, although there was a difference in BMI (3.9) between 2 groups, it might not affect gap healing after OWHTO in our study.
Lateral hinge fracture did not affect gap healing in our study. Meidinger et al 13 reported that 60% of patients with nonunion showed lateral hinge fracture compared with 24.4% of patients with union. Nondisplaced lateral hinge fracture is a minor complication that does not need additional surgical treatment. 9 The incidence of lateral hinge fracture in our study (23.3%) was comparable with that in other studies (2.5%-26.3%, according to the presence of displacement). 9,13,14,21 There was only 1 case of Takeuchi type 2 fracture in the LC group. Although the patient’s correction angle decreased 2.8° (from 10.8° to 8°) and the gap healing was low (GVR, 18.4%; ratio of GFH, 65.8%) compared with other patients, the patient obtained acceptable gap healing. There were no other cases of correction loss in our study. Our findings indicate that nondisplaced lateral hinge fracture does not require further surgical treatment. However, orthopaedic surgeons should carefully follow a patient with Takeuchi type 2 fracture.
The results of our study also confirmed our hypothesis that additional gap healing would occur after plate removal. Studies have found that bone healing can be delayed because the stiffness of the locking plate suppresses interfragmentary movement. 1,2,15,19 In our study, although a significant difference in GVR was found depending on whether the plate was removed, there was no statistical difference in the GFH ratio. Gap healing was achieved in a 3-dimensional plane, not in a 2-dimensional plane. In addition, at the stage where gap healing was almost complete, there was no significant difference in the ratio of change in maximal height of newly filled bone (GFH ratio). However, gap healing was still achieved around the middle portion of the newly filled bone around the osteotomy site. These factors might have contributed to the difference in radiographic indexes between the SC and LC groups. Considering these findings, we believe that additional gap healing was achieved from plate removal. Gap healing around the osteotomy site might be influenced by the stress shielding effect. 19 Because the Young modulus of the locking plate (titanium) is higher than that of cortical bone, most stress is transferred via the locking plate. Most patients achieved acceptable stability after OWHTO using locking plate. 4,16 Moreover, additional gap healing might be expected after plate removal. In light of these 2 findings, there may be no clinical or economic advantage of using bone grafting in OWHTO.
There were several limitations in our study. The study had a retrospective design, and patients who needed large correction (≥13°) were not included; therefore, we cannot generalize our results to all cases of OWHTO. In addition, the differences in demographic data such as age and BMI between the 2 groups might have affected the gap healing around the osteotomy site. However, a previous study reported that age did not have an adverse effect on radiologic outcomes after OWHTO. 7 The difference in age between the SC and LC groups in our study (59.4 and 53.5 years, respectively) was less than that in the study by Goshima et al 7 (68.7 and 56.2, respectively). Therefore, although there was a difference in age between the 2 groups, we believe it did not significantly affect gap healing after OWHTO. Another limitation is that gap healing might have been underestimated. We evaluated gap healing using anteroposterior radiographs. Although gap healing at the osteotomy site takes place in 3 dimensions, we could evaluate gap healing in only 2 dimensions on the radiographs. A 3-dimensional modality, such as computed tomography, would be needed for a more accurate measurement. However, such a modality might expose patients to unnecessary radiation and is not a practical method for assessing gap healing in the clinical setting. Furthermore, the locking plate was usually placed on the anteromedial side of the proximal tibia, which did not allow us to properly evaluate the gap healing on radiographs. Finally, our study results were based on radiographic indexes rather than clinical symptoms. We might have found different outcomes if a clinical evaluation had been included.
Conclusion
All patients achieved acceptable gap healing without bone graft. The degree of gap healing was higher in the SC group and increased over time. Gap healing was also promoted after plate removal. Considering the results of this study, bone graft is not necessary in routine OWHTO in terms of gap healing.
Footnotes
Final revision submitted October 25, 2020; accepted December 15, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was supported by the Bio & Medical Technology Development Program of the National Research Foundation (NRF), funded by the Korean government (MSIT) (2017M3A9D8063538). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Seoul National University Boramae Medical Center (No. 30-2019-76).