
Abstract
Purpose
After high tibial osteotomy, the patella may change position and osteoarthritis of the patellofemoral joint (PFJ) may occur. It was hypothesized that the course of PFJ degeneration would differ between open wedge high tibial osteotomy (OWHTO) and hybrid closed wedge high tibial osteotomy (hybrid HTO). Accordingly, this study aimed to evaluate the qualitative changes in PFJ articular cartilage, during the early postoperative period after OWHTO and hybrid HTO.
Methods
This was a retrospective observational study of 75 knees that underwent OWHTO (N = 37) or hybrid HTO (N = 38) for medial knee osteoarthritis. OWHTO and hybrid HTO were indicated for corrections of less than 10° and more than 10°, respectively. MRI of all knees was performed before and 6 months after surgery to evaluate patellar cartilage in sagittal images for T2 mapping. Three regions of interest (medial, middle, and lateral facets) were defined in the articular cartilage, and T2 values were measured. Patellar tilting angle, lateral shift ratio, and patellar height were compared before and after surgery.
Results
There was no significant change in arthroscopic findings of PFJ articular cartilage between the OWHTO and hybrid HTO groups. In the OWHTO group, the mean T2 value of medial and middle facets increased significantly (lateral, 43.0 ± 3.9 to 43.7 ± 3.5; middle, 44.2 ± 3.9 to 46.2 ± 3.8; medial 41.0 ± 4.3 to 42.4 ± 4.0). Conversely, no significant change was observed in the hybrid HTO group (lateral, 41.1 ± 4.0 to 42.3 ± 4.0; middle, 43.6 ± 4.2 to 44.5 ± 4.3; medial, 40.7 ± 4.1 to 41.5 ± 4.5). Patellar height decreased and increased in the OWHTO and hybrid HTO groups, respectively, and patellar tilt decreased in the OWHTO group. Lateral shift ratio decreased significantly in both groups.
Conclusions
OWHTO with a small correction angle may result in qualitative changes in PFJ articular cartilage from an early stage, while hybrid HTO with a relatively large correction angle is unlikely to affect PFJ articular cartilage.
Keywords
Introduction
High tibial osteotomy (HTO) is a joint-preserving surgery for early osteoarthritis (OA) and spontaneous osteonecrosis of the knee (SONK). Since the 2000s, locking plates have been introduced as the internal fixation material for osteotomies, allowing early postoperative weight bearing, with reportedly good clinical outcomes.1-3 HTO mainly consists of medial open wedge high tibial osteotomy (OWHTO) to open the medial side of the tibia, and lateral closed wedge high tibial osteotomy (CWHTO) to close the lateral side.4,5 In OWHTO, osteotomy is performed proximal to the tibial tubercle, and the medial side is opened to correct the lower extremity to the valgus alignment. As a result, the tibial tubercle and patella are moved distally, thereby increasing pressure on the patellofemoral joint (PFJ). A large correction has been reported to result in postoperative osteoarthritis of PFJ. 6 In recent years, OWHTO has been indicated for patients requiring minimal correction, but it is unclear whether this approach has a subsequent effect on the PFJ.
In contrast, hybrid HTO was developed to avoid the disadvantages of conventional CWHTO. The hinge point is set at two-thirds or half of the osteotomy line from the lateral side of the tibia, which is then resected in a wedge shape and closed to set the lower limb to the valgus alignment, allowing for large correction. 7 In addition, because the tibial tubercle is moved proximally, hybrid HTO can be indicated in patients with OA of the PFJ. 8 However, prior reports have indicated that OA of PFJ progresses with large alignment correction, 9 and the effect of hybrid HTO on PFJ is controversial. Clarification of the impact of these techniques on PFJ may provide important knowledge for selecting and devising techniques to minimize the impact on PFJ.
T2 mapping, an MRI imaging method, can reveal qualitative changes in the articular cartilage by assessing changes in collagen alignment and water content.10-19 Using T2 mapping, the influences of OWHTO and hybrid HTO on PFJ can be assessed early. With respect to the above information, we hypothesized that the course of PFJ degeneration would differ between OWHTO and hybrid HTO. Thus, this study aimed to evaluate the qualitative changes in the PFJ articular cartilage during the early postoperative period following OWHTO and hybrid HTO.
Materials and methods
This retrospective observational study was performed in accordance with a protocol approved by the Institutional Review Board of our hospital (Approval No. ERB-21-03) based on the principles of the Declaration of Helsinki and its later amendments or comparable ethical standards.
Subjects
Seventy-five knees that underwent OWHTO (N = 37; 14 male, 23 female) or hybrid HTO (N = 38; 11 male, 27 female) at our hospital from August 2017 to November 2019 were enrolled. The inclusion criteria were as follows: medial OA, SONK of the medial femoral condyle, pre- and post-operative MRI T2 mapping, and follow-up until hardware removal. The exclusion criteria were as follows: Kellgren-Lawrence grade 4 of PFJ, preoperative MRI at another hospital prior to referral to our hospital, and patients who declined to undergo postoperative MRI. In the OWHTO and hybrid HTO groups, the observation periods were 12.3 ± 3.0 and 13.8 ± 4.5 months (mean 13.0 ± 3.7), respectively. For preoperative planning, full-length standing anteroposterior radiographs of the legs were plotted using digital planning software (Ortho Planner Pro; Toyo Technica, Osaka, Japan). To achieve suitable realignment of the lower limb resulting in valgus correction, the target mechanical axis (%MA) was set at 62.5% from the medial edge of the tibial plateau to its entire length (Fujisawa point). OWHTO was selected for patients with correction angles <10°, and hybrid HTO was selected for patients with correction angles ≥10°, flexion contracture > 10°, or anterior knee pain.20,21
Radiological evaluation
Simple radiographic images of the knee joint were evaluated preoperatively and before hardware removal. The hip-knee-ankle angle (HKAA) and medial proximal tibial angle (MPTA) were measured using the full-length standing images (Figure 1).22,23 The tilting angle of patella (TA), sulcus angle (SA), lateral shift ratio, and congruence angle (CA) were measured by Merchant imaging (knee joint flexion 45°) to evaluate the PFJ.24,25 The Insall-Salvati ration (IS ratio) and Blackburne-Peel (BP) ratio were measured at 30° knee joint flexion to evaluate the patellar height.26,27 Patellofemoral osteoarthritis was evaluated using Kellgren and Lawrence grading.
28
(a) Method used to measure the hip-knee-ankle angle (HKAA) and medial proximal tibial angle (MPTA). (b) Method used to measure the Insall-Salvati ratio (②/①) and Blackburne-Peel ratio (④/③). (c) Method used to measure the tilting and congruence angles.
MRI T2 mapping
All knees underwent 1.5 T MRI (Brivo MR355 Inspire; GE Healthcare, Chicago, USA) pre-operatively and at 6 months post-operatively. The imaging protocol included turbo spin echo (TSE); multi-echo time (TE); repetition time (TR), 1200 msec; TE, 7.5/15/22.5/30/37.5/45/52.5/60 msec; field of view (FOV), 160 mm; slice thickness, 3.0 mm; slice gap, 0.6 mm; slices, 15 slices; NEX, 2; bandwidth, 31.25 kHz; scan time, 5 min 22 s; and a 224 × 224 matrix. T2 mapping images were calculated and generated from multiple images.
To assess the effects of OWHTO and hybrid HTO on the PFJ, the axial plane in the center of the patella was examined in T2 mapped images. Patellar width was divided into three equal parts, establishing three regions of interest (ROI): the medial, middle, and lateral (Figure 2). The depth of each ROI was set to cover the superficial and middle layers of the patellar cartilage, but with a margin of a few pixels away from the articular cartilage surface to avoid partial volume effects. The pre- and post-surgery T2 values were compared to ascertain the effect on cartilage degeneration. The mean T2 values were calculated using OsiriX imaging software (OsiriX Foundation, Switzerland).
29
All measurements were performed blindly and independently by two orthopedic surgeons specializing in knee surgery with 7 and 14 years of experience, respectively. Axial image of the center of the patella. The depth of the region of interest in the articular cartilage was set to encompass the superficial and intermediate layers.
Surgical procedure
The International Cartilage Repair Society (ICRS) grades were determined by arthroscopy before osteotomy.
30
OWHTO and hybrid HTO were performed according to previous reports.7,20 During the OWHTO procedure, the osteotomy line was set 35 mm distal to the articular surface, and after biplane osteotomy, the medial side was opened and filled with artificial bone (Olympus Terumo Biomaterials Co., Japan) (Figure 3(a)). In hybrid HTO, this line was set 40 mm from the articular surface after resection of 20 mm from the center of the fibula. The length of the osteotomy line was divided in a 1:3 ratio to determine the hinge point, and osteotomy was made in a wedge shape for the correction angle, closed, and then fixed with a lateral plate for hybrid HTO (Olympus Terumo Biomaterials Co.) (Figure 3(b)). After 1 week of unloading, the patient was started on 1/2 partial load followed by 2/3 PWB, depending on pain. Full weight bearing was allowed two weeks after surgery. Representative postoperative radiographs. (a) OWHTO. (b) hybrid HTO.
Statistical analysis
Reliability for evaluating radiological and MRI findings.

Results
Patient characteristics.

BMI body mass index, K/L Kellgren-Lawrence *p < 0.05.
Change in knee alignment after open wedge high tibial osteotomy and hybrid high tibial osteotomy.
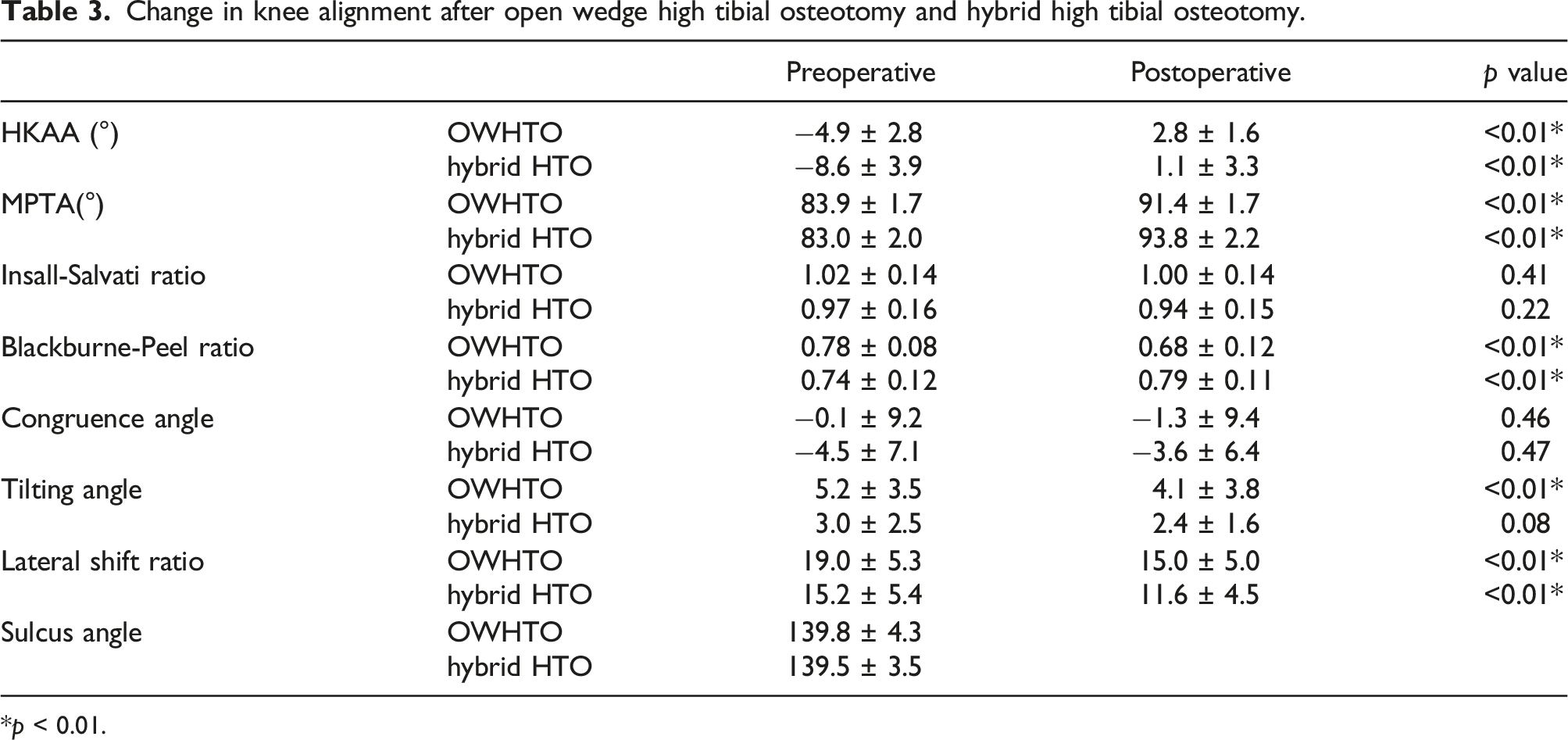
*p < 0.01.
Gross evaluation of the patellofemoral cartilage.

Change in T2 values before and after OWHTO.
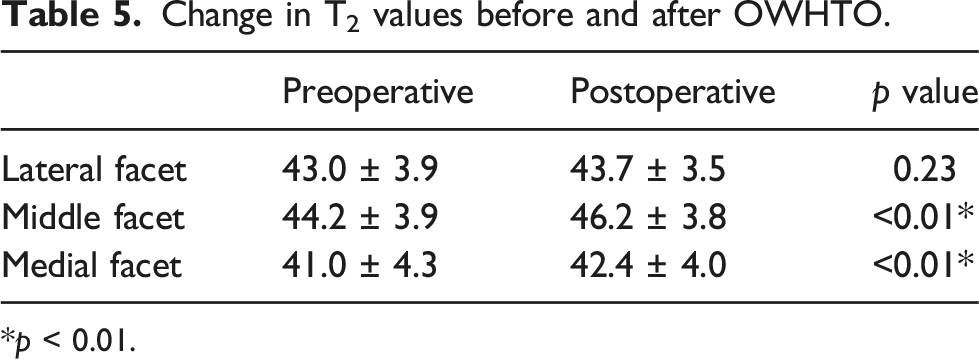
*p < 0.01.
Change in T2 values before and after hybrid HTO.

Representative cases
MRI T2 mapping of a 43-year-old man (BMI 19.8) revealed T2 values of 42.8, 45.4, and 45.9 for articular cartilage in the medial, middle, and lateral facets, respectively (Figure 4(a)). A correction of 5° was performed with OWHTO. At 6-months post-surgery, the T2 values of the articular cartilage were 45.9, 53.2, and 46.3 for the medial, middle, and lateral facets, respectively (Figure 4(b)).

Imaging results of a representative patient who underwent OWHTO. (a) Preoperative MRI. (b) Postoperative MRI with increased T2 values in the middle facet.
MRI T2 mapping of a 66-year-old woman (BMI 24.1) showed that the T2 values of articular cartilage were 35.7, 44.2, and 35.9 for the medial, middle, and lateral facets, respectively (Figure 5(a)). A correction of 11° was performed with hybrid HTO. The T2 values of the articular cartilage were 35.6, 43.5, and 33.7 for the medial, middle, and lateral facets, respectively (Figure 5(b)).

Imaging results of a representative patient who underwent hybrid HTO. (a) Preoperative MRI. (b) Postoperative MRI showed no significant increase in T2 value.
Discussion
The most important finding of this study is that at 6 months after surgery, the OWHTO group showed degeneration of the articular cartilage of the medial and middle facets with decreased patellar height and a reduction of TA, while the hybrid HTO group showed no degeneration of the articular cartilage of the patella.
In the case of OWHTO, even a minor correction may result in subsequent deleterious PFJ effects, suggesting that other techniques may need to be considered, or the technique should be modified. Because of the different surgical indications for OWHTO and hybrid HTO in this study, patients who underwent hybrid HTO were older and had a significantly greater degree of varus deformity than those who underwent OWHTO. Therefore, it is difficult to compare the degeneration of the PF joints between the two groups. However, the natural history of the qualitative changes in the PFJ in each surgery was revealed to be different for the first time by T2 mapping.
OWHTO is joint-preserving surgery for medial knee osteoarthritis and SONK, and good clinical results have been obtained. However, adverse effects on PFJ due to decreased postoperative patellar height and increased PFJ contact pressure have been reported. Prior biomechanical studies have indicated changes in patellar height results from postoperative movement of the tibial tuberosity distally and the pulling down of the patella.31-33 Tanaka et al. reported that PFJ cartilage damage tends to progress following OWHTO in patients with medial open gap
Biomechanical studies of CWHTO have shown that the tibial tubercle moves proximally following surgery. 32 Hybrid HTO involves biplanar osteotomy of the tibial tubercle, resulting in internal rotation of distal bone fragments and anterior migration of the tibial tubercle.7,37 Otsuki et al. reported that hybrid HTO improved TT-TG distance and the medial joint space of PFJ. 38 Therefore, this surgery is effective when the correction angle is relatively large or when there is a problem with the PFJ. 8 In contrast, PFJ cartilage degeneration has been reported to progress with large correction, even in hybrid HTO. Song et al. reported that >10° correction in hybrid HTO poses a risk of progression of PFJ cartilage degeneration. 9 In the present study, hybrid HTO was selected for patients with ˃10° correction or PFOA symptoms. A mean of 12.6° correction was performed, but there was no significant change in the patellar height, patellar tilt, or the T2 values of the patellar cartilage. Therefore, we suggest that hybrid HTO with an appropriate amount of correction may avoid OA progression in PFJ.
This study has several limitations that should be noted, with the most notable one being its retrospective design. Furthermore, the patients’ background and the indications for surgery differed between the two groups, making comparison impossible. Third, the short follow-up period prevented investigation of potential long-term degeneration of the PFJ cartilage.
Conclusions
In this study, we evaluated patellar cartilage degeneration at 6 months post-surgery in patients who underwent OWHTO or hybrid HTO. MRI T2 mapping revealed that OWHTO may cause cartilage degeneration of the patellofemoral joint, even with a small correction, while hybrid HTO may avoid such cartilage degeneration, even with a relatively large correction. This study provides new insights into the selection of surgical techniques and presents new information to help minimize deleterious post-operative impacts on the patellofemoral joint.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.