
Abstract
Background:
There is no consensus on the ideal treatment for partial articular supraspinatus tendon avulsion (PASTA) lesions without tendon damage.
Purpose:
To introduce a novel “retensioning technique” for arthroscopic PASTA repair and to assess the clinical and radiologic outcomes of this technique.
Study Design:
Case series; Level of evidence, 4.
Methods:
A retrospective analysis was performed on 24 patients whose PASTA lesion was treated using the retensioning technique between January 2011 and December 2015. The mean ± SD patient age was 57.6 ± 7.0 years (range, 43-71 years), and the mean follow-up period was 57.6 ± 23.4 months (range, 24.0-93.7 months). Sutures were placed at the edge of the PASTA lesion, tensioned, and fixed to lateral-row anchors. After surgery, shoulder range of motion (ROM) and functional scores (visual analog scale [VAS] for pain, VAS for function, American Shoulder and Elbow Surgeons [ASES] score, Constant score, Simple Shoulder Test, and Korean Shoulder Score) were evaluated at regular outpatient visits; at 6 months postoperatively, repair integrity was evaluated using magnetic resonance imaging (MRI).
Results:
At 12 months postoperatively, all ROM variables were improved compared with preoperative values, and shoulder abduction was improved significantly (136.00° vs 107.08°; P = .009). At final follow-up (>24 months), the VAS pain, VAS function, and ASES scores improved, from 6.39, 4.26, and 40.09 to 1.00, 8.26, and 85.96, respectively (all P < .001). At 6 months postoperatively, 21 of the 24 patients (87.5%) underwent follow-up MRI; the postoperative repair integrity was Sugaya type 1 or 2 for all of these patients, and 13 patients showed complete improvement of the lesion compared with preoperatively.
Conclusion:
The retensioning technique showed improved ROM and pain and functional scores as well as good tendon healing on MRI scans at 6-month follow-up in the majority of patients. Thus, the retensioning technique appears to be reliable procedure for the PASTA lesion.
Keywords
Partial-thickness rotator cuff tear (PTRCT) is a commonly encountered condition in patients who have shoulder pain. Since PTRCT was first described by Codman 3 in 1934, its prevalence has increased because of advances in imaging and shoulder arthroscopy techniques. In 1990, Ellman 6 classified this lesion according to anatomic location (articular, bursal, and intratendinous) and the depth of the tear (grade 1, <3 mm; grade 2, 3-6 mm; grade 3, >6 mm). Articular-side tear is the most common tear among the PTRCTs 7,17,18 and was termed partial articular supraspinatus tendon avulsion (PASTA) by Millstein and Snyder 15 in 2003. The cause of the PASTA lesion is degeneration due to aging, microtrauma, or overuse. 10 Treatment of grade 1 or 2 PASTA lesion is nonoperative. However, for patients with grade 3 PASTA lesion who are not responsive to nonoperative treatment or who have >50% involvement of the thickness of the tendon, surgical treatment is indicated. 27
Many studies about repair techniques for the PASTA lesion have been published. ‡ The 2 major surgical methods for this lesion are tear-completion repair and transtendon repair. However, there is still no consensus on surgical treatment of the PASTA lesion. 2,11,21 Tear-completion repair is an easy technique and has shown good clinical results, but it damages healthy rotator cuff tendon and can cause retear of the tendon. 23 Lo and Burkhart 12 first introduced transtendon repair, 12 and others have reported good results with this technique. 10 , 26 However, transtendon repair is technically difficult, 11 and normal tissue can be damaged when the anchor is placed through the supraspinatus tendon. 12 Some studies have reported that transtendon repair was more likely to result in postoperative stiffness because of overtensioning of the repair. 19,28
The PASTA lesion entails detachment of the articular side of the supraspinatus tendon, and the elongation of the footprint weakens the tension of the supraspinatus tendon. 1 The weakening of tension in PASTA lesions can be inferred by supraspinatus muscle atrophy or fatty infiltration on sagittal oblique view on magnetic resonance imaging (MRI) scans. 1 This is similar to the “failure with continuity” concept proposed by McCarron et al. 13 It means that the repaired rotator cuff tendon retracts in the early postoperative period with or without defect.
We present our surgical method of arthroscopic PASTA repair—the “retensioning technique.” This technique focuses on restoring the tension of the torn tendon. It is similar to double-row suture bridge repair but with no medial anchor. The medial anchor is replaced by an inverted mattress suture, and the suture is tightened using a lateral knotless anchor. This restores the tension of the supraspinatus tendon and compresses the articular tear site to its footprint.
The purpose of this study was to introduce the retensioning technique for arthroscopic PASTA repair. Furthermore, we evaluated clinical and radiologic outcomes of this technique. Our aim was to show, using postoperative range of motion (ROM), functional scores, and MRI scans, that the retensioning technique is an appropriate and reliable method for the patient with PASTA lesion.
Methods
This institutional review board–approved study was a retrospective chart review that used prospectively collected data for analysis. The requirement for informed consent was waived owing to the retrospective design of the study. All surgical procedures were performed by a single senior surgeon at our institution (J.C.Y).
Patient Selection
Between 2011 and 2015, a total of 207 patients underwent surgery for supraspinatus PTRCT. We included PASTA lesions refractory to rehabilitation or involving >50% of the tendon treated via the retensioning technique. The exclusion criteria were previous shoulder surgery, preoperative frozen shoulder (global loss of motion: ≤100° of forward flexion [FF], ≤10° of external rotation [ER] with the arm at the side, and internal rotation [IR] not beyond the L5 cephalad level), bursal-side tears, completion to full-thickness tear, and <2 years of follow-up. Patients with large subscapularis tendon tear (type ≥3 according to the Yoo et al 30 classification), suprascapular neuropathy, and concomitant shoulder surgery including labral repair were excluded; 2 patients were excluded for having global loss of motion, 165 patients were excluded for having bursal-side tear, and 14 patients were excluded for having completion of the tear because of poor bursal-side tendon quality. We excluded 1 patient for having suprascapular neuropathy and 1 patient for having <2 years of follow-up. Ultimately, 24 patients (24 shoulders) were included.
Clinical Assessment
Clinical assessments, including comprehensive physical examination and functional scores, were performed regularly preoperatively and postoperatively at 2 months, 5 months, 1 year, and 2 years or more at outpatient visits. Physical examination included shoulder passive ROM and scaption strength. Shoulder passive ROM was evaluated using a goniometer. ROM included FF, abduction (ABD), ER with the arm at the side, and IR behind the back. IR was measured via the ability to reach the vertebral spinous process with the tip of the thumb and was based on contiguously numbered groups: 0 to greater trochanter of the proximal femur, 1 to buttock, 2-6 to fifth to first lumbar vertebrae, and 7-15 to twelfth to fourth throacic vertebrae. Scaption strength was measured with the patient sitting with the arm in 90° of scaption through use of a portable, handheld Shimpo Myometer (Nidec-Shimpo Co). Functional scores included the pain visual analog scale (PVAS), functional visual analog scale (FVAS), and American Shoulder and Elbow Surgeons (ASES) scores 14 ; Constant score 4 ; Simple Shoulder Test (SST) 20 ; and Korean Shoulder Score (KSS). 25 For patients who did not return to the clinic at 2 years postoperatively, the PVAS, FVAS, and ASES scores were reported via telephone survey.
MRI Evaluation
All patients underwent preoperative MRI (3.0-T Gyroscan Intera Achieva scanner; Philips Medical Systems), and a T2-weighted image was used to evaluate the PASTA lesion. The diagnosis of PASTA lesion was made when there was increased signal intensity and thinning of the tendon between the articular-side supraspinatus insertion to the greater tuberosity. At 6-month follow-up, the patients were reevaluated using MRI to assess repair integrity. Oblique coronal, oblique sagittal, and axial T2-weighted images were assessed, and the Sugaya classification of repair integrity was analyzed. 24 In this study, Sugaya type 4 (presence of a minor discontinuity) and 5 (presence of a major discontinuity) were considered retears. We also evaluated supraspinatus tendon healing and attachment to the greater tuberosity using preoperative and postoperative MRI scans. The degree of healing was assessed as no improvement, incomplete improvement, and complete improvement. Postoperative MRI scans for rotator cuff integrity were evaluated independently by 2 trained shoulder fellows (S.C.K. and J.H.J.) who were blinded to the preoperative MRI results.
Arthroscopic Evaluation
This procedure was performed with the patient in lateral decubitus position as per the senior surgeon’s preference. A standard posterior portal was established for evaluation of the glenohumeral joint. Glenohumeral articular cartilage, glenoid labrum, biceps tendon and pulley, subscapularis tendon, and supraspinatus tendon were evaluated. The PASTA lesion revealed fraying and degeneration at the insertion of the supraspinatus tendon. Careful observations were made to determine the size of the lesion and whether there was a full-thickness tear connected to the subacromial space (Figure 1).
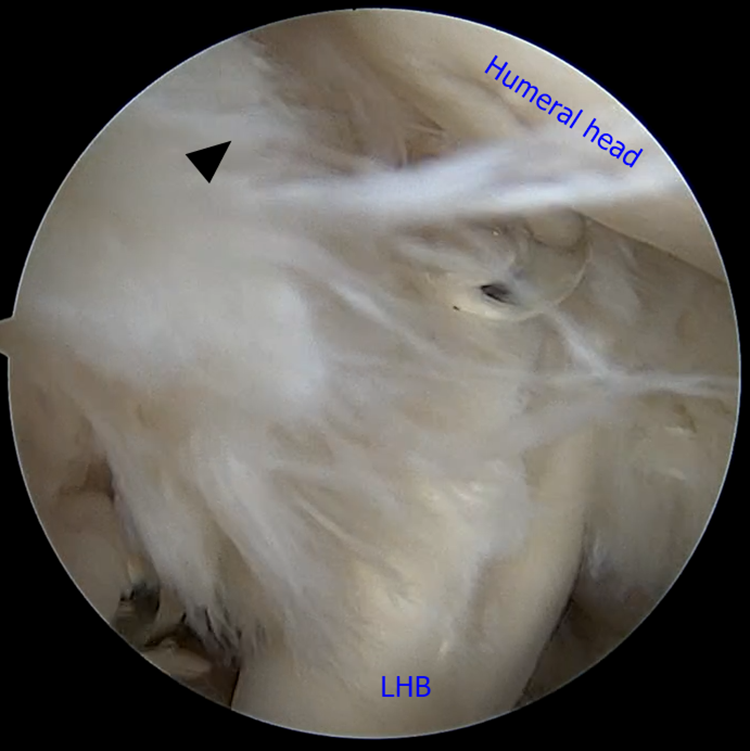
Intra-articular image of the partial articular supraspinatus tendon avulsion lesion (black arrowhead) using a standard posterior viewing portal. LHB, long head of the biceps.
Arthroscopic Procedure
After glenohumeral joint examination, an anterior portal through the rotator interval was established using the outside-in technique superior to the subscapularis tendon. If a patient had stiffness (FF ≤120°, ER ≤30°, or IR ≤L1) before surgery, anterior or pan-capsular release was done using electrocautery or arthroscopic scissors through anterior and posterior portals. If there was a type 2b subscapularis tendon tear, then the subscapularis tendon was tagged by a nonabsorbable suture using a suture hook through the anterior portal. If biceps fraying was observed, arthroscopic suprapectoral biceps tenodesis was performed for patients younger than 65 years. In patients older than 65 years, biceps tenotomy was performed. After prior procedures, a shaver was introduced through the anterior portal and passed under the biceps tendon if present. The PASTA lesion was debrided until the fresh tendon appeared. When fresh tissue did not appear, PASTA lesion was converted to full thickness tear. After the PASTA lesion was debrided, a bone bleeding procedure using a microfracture awl from the anterior portal was performed to expose the greater tuberosity bone bed in all cases (Figure 2).
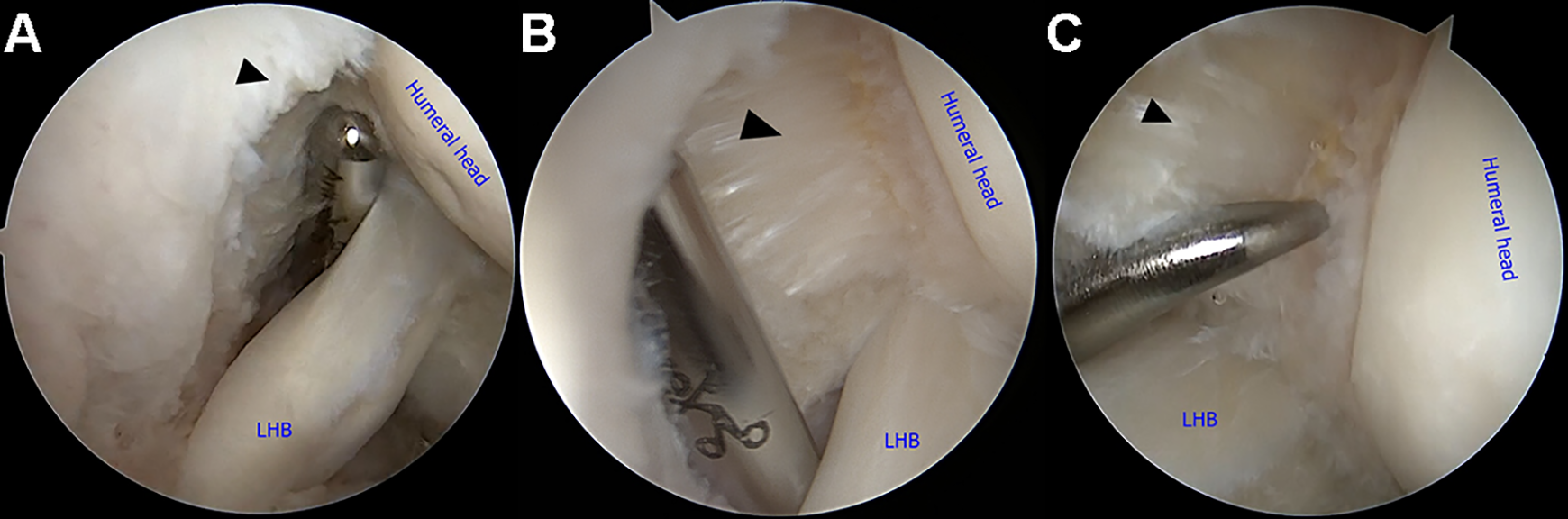
(A) The partial articular supraspinatus tendon avulsion lesion (black arrowhead) was debrided by shaving, using the standard anterior portal. (B) Complete debridement was performed to obtain fresh cuff tissue (black arrowhead). (C) Via the anterior portal, a bone bleeding procedure (black arrowhead) using a microfracture awl was performed to promote tendon healing. LHB, long head of the biceps.
When retensioning was performed, the surgeon used 2 spinal needles, 1 nylon strand (Ethilon No. 1; Ethicon, Johnson & Johnson), and 1 Monosyn strand (Monosyn No. 1; B. Braun Surgical). First, the nylon strand was passed through a spinal needle to create a loop. Then both ends of the nylon loop were pinched using curved mosquito forceps (Figure 3). While observing the inside of the joint through the posterior portal, the surgeon inserted the spinal needle with the nylon loop (SN1) alongside the anterolateral acromial corner. The skin penetration angle was 90°, allowing the spinal needle to pass perpendicular to the supraspinatus tendon. An empty spinal needle without a loop (SN2) was inserted 1 to 2 cm posterior to the SN1 and lateral to the lateral acromial border. The skin and supraspinatus tendon were penetrated perpendicularly (Figure 4A). As a result, the SN1 passed the anterior margin of the PASTA lesion, and the SN2 passed the posterior margin of the PASTA lesion (Figure 4B).

Two spinal needles were used in this technique. One spinal needle (SN1) was used to make a loop with the nylon strand. Both ends of the nylon strand were pinched using the mosquito forceps. Another spinal needle (SN2) was used to pass the Monosyn strand (B. Braun Surgical).
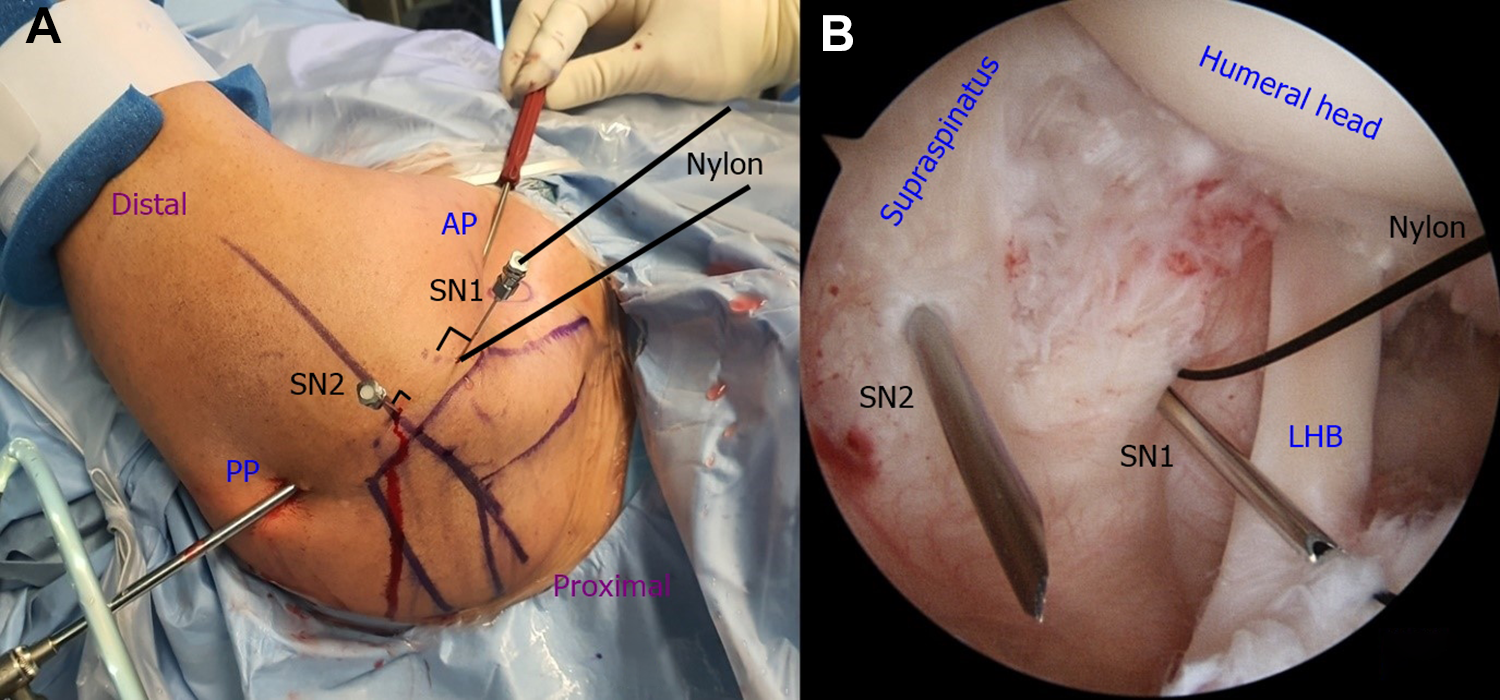
(A) Outside view of the shoulder in the lateral decubitus position. The standard posterior portal (PP) and anterior portal (AP) were used to perform the retensioning procedure. The spinal needle with a nylon loop (SN1) penetrated the skin at the anterolateral corner of the acromion at 90°. An empty spinal needle (SN2) penetrated the skin 1 to 2 cm posterior to SN1 and lateral to the lateral acromial border at a perpendicular angle. (B) Intra-articular view of the partial articular supraspinatus tendon avulsion (PASTA) lesion. SN1 penetrated the anterior edge of the PASTA lesion, and SN2 penetrated the posterior edge of the PASTA lesion. LHB, long head of the biceps.
The Monosyn strand was inserted into the SN2 to reach the joint space. The grasper was inserted through the anterior portal, passed the nylon loop, and was used to retrieve the Monosyn strand (Figure 5). Holding the opposite side of the Monosyn strand at the outside, the surgeon carefully removed the SN1. Then, the Monosyn strand in the joint was passed through the anterior side of the PASTA lesion, and the SN2 was removed. Finally, the Monosyn strand was positioned at anterior and posterior edges of the PASTA lesion, and 2 free ends were passed outside through the skin (Figure 6). The Monosyn strand was then used to shuttle the nonabsorbable strand.

(A) After the spinal needles were positioned, the Monosyn strand (B. Braun Surgical) passed the hole of SN2 from outside to the glenohumeral joint. The grasper was inserted from the anterior portal (AP) toward the intra-articular space. (B) The Monosyn strand was passed through the nylon loop and was pulled by the grasper from the AP. LHB, long head of the biceps; PP, posterior portal; SN1, spinal needle with loop; SN2, spinal needle without loop.
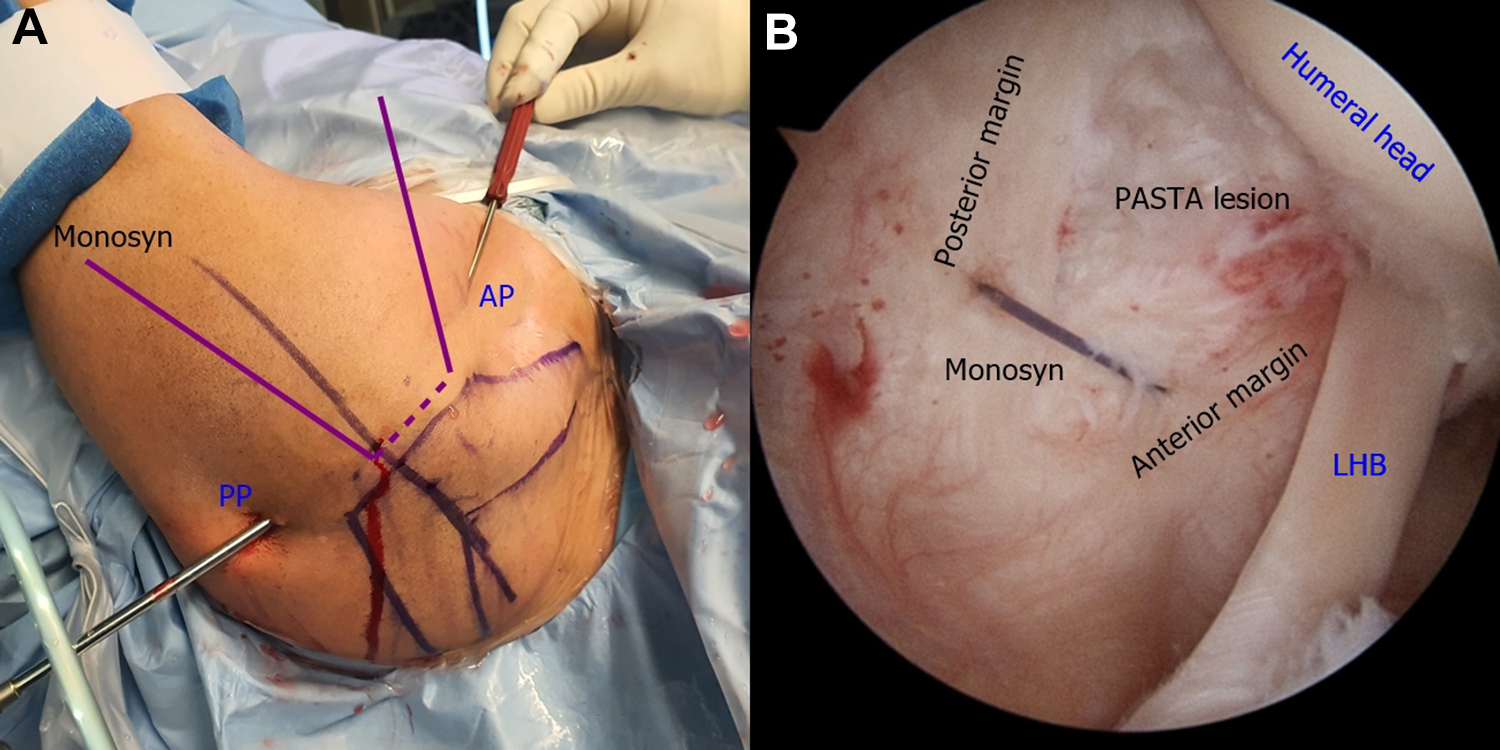
The Monosyn strand (B. Braun Surgical) from the empty spinal needle was held by hand, and the spinal needle with a nylon loop was removed carefully. The Monosyn strand from the anterior portal (AP) was passed through the anterior edge of the partial articular supraspinatus tendon avulsion (PASTA) lesion. The other spinal needle was removed. (A) External profile of a shoulder and the Monosyn strand. (B) The Monosyn strand passed the anterior and posterior margin of the PASTA lesion in a reverse mattress suture pattern. LHB, long head of the biceps; PP, posterior portal.
If the PASTA lesion was >1 cm, the procedure was performed twice using 2 strands. One nonabsorbable strand passed the anterior one-third and posterior margin of the PASTA lesion, and another nonabsorbable strand passed the posterior one-third and anterior margin of the lesion. Thus, the 2 strands were crossed at the middle of the lateral side of the PASTA lesion in a pattern that entailed a vertical mattress suture behind a horizontal mattress suture (Figure 7).

In case of a large lesion (>1 cm width), double nonabsorbable strands were used in a pattern that entailed a vertical mattress suture behind a horizontal mattress suture. A spinal needle with nylon loop was inserted in the same manner as that shown in Figure 4; another spinal needle for passage of a Monosyn strand (B. Braun Surgical) penetrated through the posterior one-third and medial side of the lesion. The Monosyn strand was passed through the spinal needle and nylon loop, and the spinal needle with the nylon loop was removed. The Monosyn strand was then used to shuttle the nonabsorbable strands. Another nonabsorbable strand was positioned at the posterior margin, anterior one-third, and medial side of the lesion in the same manner. LHB, long head of the biceps.
The arthroscope was then moved to the subacromial space. The usual subacromial portals were made: posterior, anterior, lateral, and posterolateral portals. Coracoacromial ligament, acromial shape, and acromial spur were assessed after debridement of the subacromial bursa. If there was evidence of external impingement (coracoacromial ligament fraying or curved acromion), the surgeon performed subacromial decompression to prevent any future external impingement. After subacromial decompression, the nonabsorbable strands were retrieved to the lateral portal by use of a retriever. A probe was introduced through the lateral portal to evaluate the bursal side of the PASTA lesion. The nonabsorbable strands were used as a guide to confirm the location of the PASTA lesions. If the tendon did not feel elastic when pressed with a probe, the tendon was judged to be of poor quality. In such cases, the surgeon performed tear completion to the full-thickness tear and then repair using the double-row with a suture-bridge or small-window technique. 29 If the supraspinatus tendon was healthy and did not need tear completion, the retensioning repair technique was performed.
Each strand from the medial mattress suture was passed through a hole at the end of the lateral knotless anchor device. The surgeon created a hole for the lateral anchor 2 cm distal from the lateral edge of the greater tuberosity. While holding both ends of the strand with both hands, the surgeon alternately pulled both ends to apply enough tension to compress the supraspinatus tendon to the footprint, and the lateral anchor was driven into the hole and engaged (Figure 8).
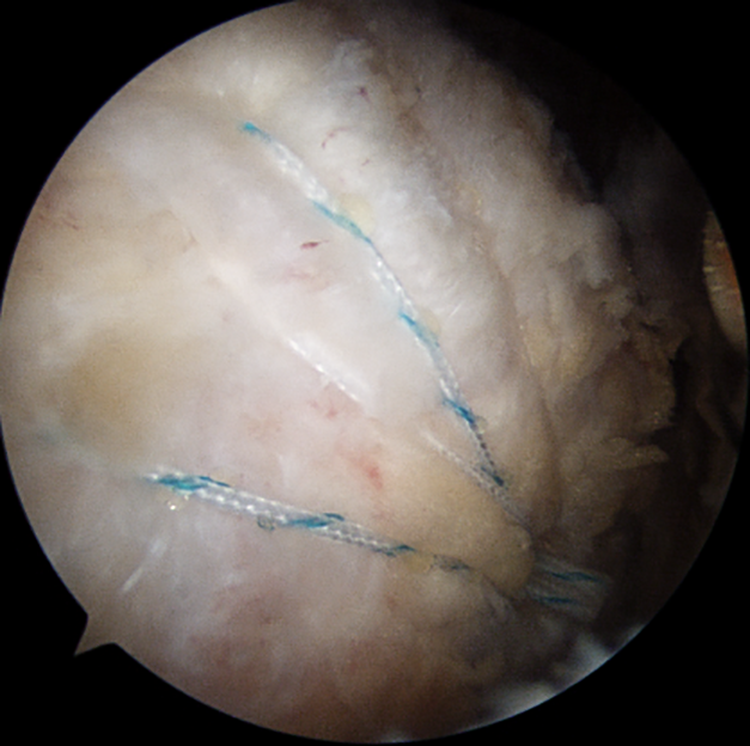
View of the subacromial space from the standard posterolateral viewing portal. The nonabsorbable strands were retrieved to the lateral portal. A hole was created for the lateral knotless anchor 2 cm distal from the lateral edge of the greater tuberosity to engage the anchor. This shows the last view after anchor insertion.
Rehabilitation
The rehabilitation protocol was the same for all patients. After surgery, patients wore a brace for 4 weeks with ABD fixed at 20° to 30°, with allowance for elbow and finger exercise. Beginning the day after surgery, passive ROM exercises were performed 2 or 3 times a day for 30 minutes each using a continuous passive motion (CPM) machine for FF and a stick for rotation. The arc of motion of the CPM and stick exercises was allowed to be as wide as possible without discomfort. At 4 weeks after surgery, the ABD brace was removed, and active ROM exercises were initiated. Rotator muscle strengthening exercises using elastic bands were started at 8 weeks postoperatively. During the first 6 postoperative months, patients were prohibited from any heavy overhead lifting and aggressive activity that required acceleration of the arm. In case of osteoporosis (T score < –2.5), the CPM and stick exercises were delayed for 2 postoperative weeks.
Statistical Analysis
To compare preoperative and postoperative continuous variables, the paired t test was performed for parametric variables. The Wilcoxon signed rank test was used for nonparametric variables, and generalized estimating equations were used to analyze scaption power. The interobserver agreement between the 2 raters for the postoperative MRI evaluation was quantified by using Cohen kappa coefficient (κ). The values of κ <0.4, 0.4 ≤ κ < 0.75, and κ ≥0.75 were considered marginal, good, and excellent reliability, respectively.
SAS Version 9.4 (SAS Institute) was used for all statistical analysis with a CI of 95%. A P value of <.05 was considered statistically significant.
Results
The mean follow-up period in this study was 57.62 ± 23.43 months, and the mean age of patients at operation was 57.58 ± 6.95 years. Postoperative 1-year outpatient follow-up with comprehensive physical examination was performed for 20/24 patients (83.3%), and final follow-up including telephone survey was performed for 23/24 patients (95.8%). The details of patient characteristics are presented in Table 1. One patient had sports-related injury, and the remaining 23 patients had overuse injury. Among the patients with overuse injury, 9 patients performed sports activities, 14 patients did not participate in sports activities, and 8 patients performed heavy labor. Preoperative calcific tendinitis was observed in the supraspinatus tendon in 2 patients, with the deposits being <4 mm. Both patients underwent calcific deposit debridement during surgery.
The concomitant surgical procedures are listed in Table 1. Only 7 patients, all with subscapularis tear type 2b, underwent subscapularis repair. We found that 3 patients had no biceps tendon, and biceps tenotomy and tenodesis were performed in 8 patients each. There were 5 patients who had a PASTA lesion of <1 cm after debridement and underwent single-strand PASTA retensioning repair. The other patients, who had a PASTA lesion >1 cm, underwent double-strand repair.
Descriptive Dataa

a PASTA, partial articular supraspinatus tendon avulsion.
b According to Yoo et al. 30
Clinical Assessment
Table 2 shows pre- and postoperative ROM, functional scores, and scaption power. Shoulder ROM and scaption power were evaluated at 1 year postoperatively and functional scores were evaluated at final follow-up (>2 years postoperatively). After arthroscopic PASTA retensioning repair, the patients showed improvement in ROM at 1 year postoperatively. Improvements in ABD were statistically significant. We found that 2 patients had <120° of FF at 1 year postoperatively; however, 1 patient had 130° of FF at final follow-up. Another patient did not visit the outpatient clinic after 1 year postoperatively. The patient was surveyed via telephone, and the PVAS, FVAS, and ASES scores were 0, 7, and 77, respectively. All functional scores at final follow-up were significantly improved compared with preoperative scores except for the Constant score. Mean scaption power improved from 8.75 ± 4.92 to 11.94 ± 4.29 ft-lb at 1 year postoperatively, which was statistically significant (P = .002).
Preoperative and Postoperative Shoulder Range of Motion, Functional Scores, and Scaption Power a

a Data are presented as mean ± SD. Bolded P values indicate statistically significant difference between groups (P < .05). ABD, abduction; ASES, American Shoulder and Elbow Surgeons; ER, external rotation; FF, forward flexion; FVAS, functional visual analog scale; IR; internal rotation; KSS, Korean Shoulder Score; PVAS, pain visual analog scale; ROM, range of motion; SST, Simple Shoulder Test.
b ROM and power were evaluated at postoperative 1 year, and functional scores were evaluated at final follow-up >2 years postoperatively.
c 0 to greater trochanter of the proximal femur, 1 to buttock, 2-6 to fifth to first lumbar vertebrae, and 7-15 to twelfth to fourth throacic vertebrae.
Repair Integrity
The 6-month follow-up MRI was carried out for 21 of the 24 patients (87.5%). Preoperatively, all PASTA lesions were assessed as Sugaya type 2 or 3. Postoperative repair integrity for all patients was Sugaya type 1 or 2, indicating no retear. In terms of the degree of tendon healing, 13 patients showed complete improvement according to both raters, 3 patients showed incomplete improvement according to both raters, and no patient showed no improvement (Table 3; Figure 9). The interrater reliability was good for all evaluations.
Preoperative and Postoperative MRI Evaluation by Raters a

a Three of the study participants did not undergo follow-up magnetic resonance imaging (MRI). Intrarater reliability was as follows: κ = 0.58 for preoperative Sugaya type; κ = 0.40 for postoperative Sugaya type; κ = 0.43 for change in lesion (good reliability for all). Dashes indicate the 3 study participants who did not undergo follow-up magnetic resonance imaging (MRI).
b Assessed as no improvement, incomplete improvement, or complete improvement.
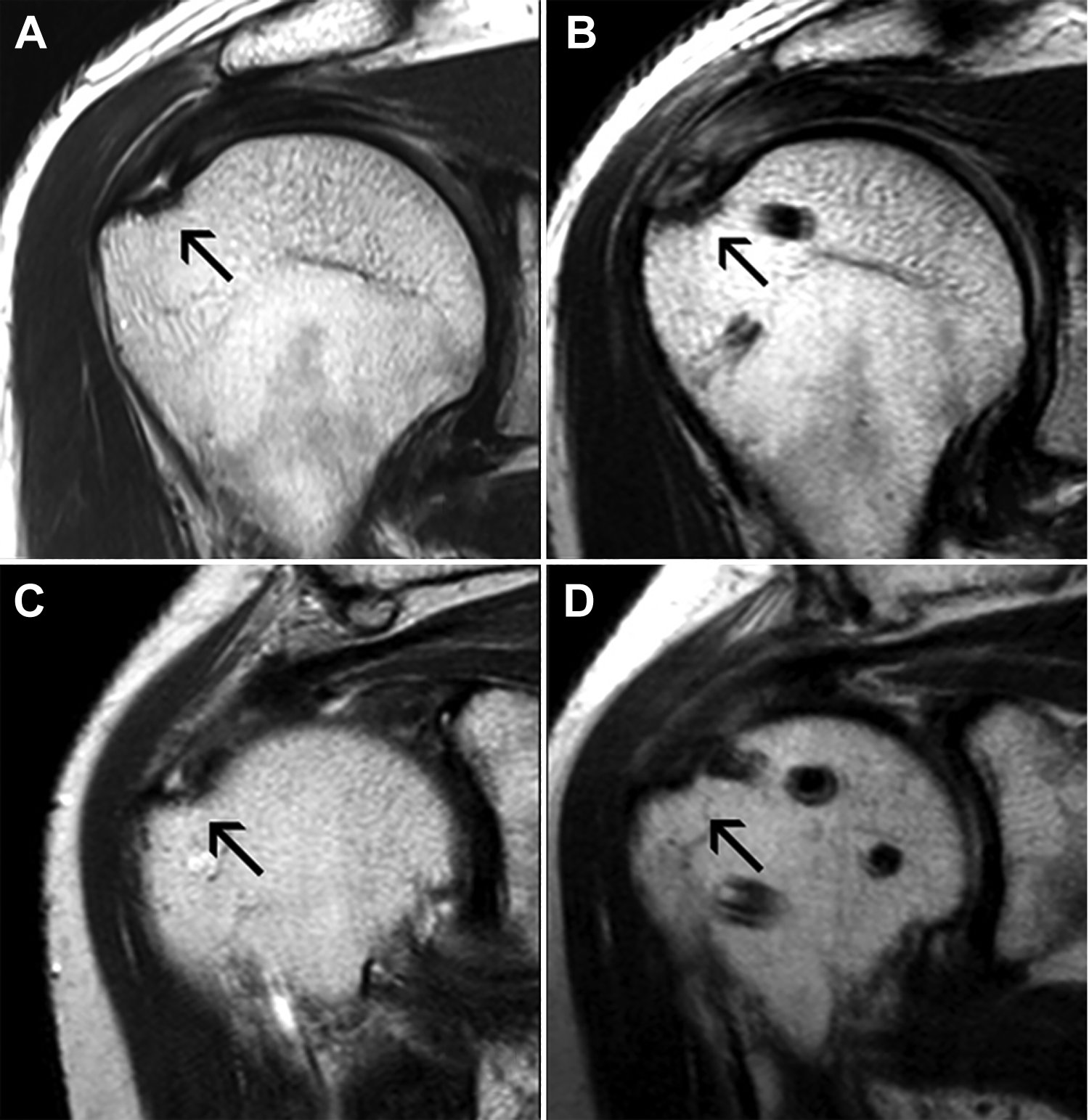
Preoperative and postoperative magnetic resonance imaging (MRI) scans of partial articular supraspinatus tendon avulsion lesions with retensioning. (A) Preoperative MRI scan showed supraspinatus articular-side tear with high signal intensity (black arrow, Sugaya type 3). (B) After retensioning, the torn tendon showed incomplete improvement (black arrow, good continuity with high signal intensity, Sugaya type 2). (C) Preoperative MRI scan showed supraspinatus articular-side tear with high signal intensity (black arrow, Sugaya type 3). (D) After retensioning, the torn tendon showed complete improvement (black arrow, good continuity without high signal intensity, Sugaya type 1).
Analysis of Patient With Unsatisfactory Results
Poor results were seen in 1 patient, a woman who was 57 years old. She performed heavy labor and did not play any sport. She had undergone total thyroidectomy for papillary thyroid cancer 6 years previously and was taking thyroid hormone medication. Before and after the surgery, her thyroid hormone level was at times below the normal range. Symptom duration before surgery was 12 months, and she reported night pain. Her FF, ER, and ABD before surgery were 140°, 50°, and 80°, respectively. Her preoperative IR was only to the buttock. Her preoperative function was poor, with PVAS, FVAS, ASES, Constant, KSS, and SST scores of 7, 3, 20, 23, 25, and 0, respectively. During surgery, she underwent anterior capsular release, subacromial decompression, and biceps tenotomy. The PASTA lesion was repaired via 2 strands using the retensioning technique. Her subscapularis tendon was intact.
After surgery, the patient reported persistent shoulder pain for up to 1 year. At postoperative 1 year, her FF, ER, IR, and ABD were poor at 140°, 20°, L5, and 130°, and her PVAS, FVAS, ASES, Constant, KSS, and SST scores were 7, 5, 33, 42, 50, and 5, respectively. However, at postoperative 6 months, her MRI scan showed complete cover of the supraspinatus footprint with homogeneous signal intensity. Therefore, we decided to perform reoperation. Arthroscopic pancapsular release and bursectomy without rotator cuff repair were performed. At 3 years after reoperation, the patient’s shoulder outcomes were subjectively unsatisfactory. However, her ROM was good (FF, ER, IR, and ABD of 160°, 60°, T10, and 160°, respectively), although her functional scores were poor (PVAS, FVAS, ASES, Constant, KSS, and SST scores of 4, 6, 50, 56, 55, and 6, respectively). Other patients did not develop complications during or after surgery.
Discussion
We performed a novel arthroscopic retensioning technique for PASTA lesions refractory to rehabilitation or involving >50% of the tendon for patients who had no concomitant bursal-side tears. Patients were followed for at least 2 years, and all but 1 patient had satisfactory clinical results. At postoperative 6 months, follow-up MRI was performed for 21 of 24 (87.5%) patients, and all of them had good tendon healing (Sugaya classification 1 or 2) without retear.
Partial tear of the supraspinatus is common; however, there is no consensus regarding surgical treatment for this injury. Currently, 3 major surgical techniques are used: tear-completion repair, transtendon repair, and debridement. Tear-completion repair damages the normal rotator cuff tissue, and transtendon repair is technically demanding and also damages the normal tissue. The surgeon’s choice of technique may depend on his or her familiarity with a technique or the condition of the lesion.
In rotator cuff repair, torn and retracted rotator cuff tendon can be tensioned using a knotless anchor. Some studies have reported upper subscapularis tendon repair techniques using knotless suture anchors. 5,16 These techniques entail the use of free strands to pass the subscapularis tendon and then fix it at the lessor tuberosity using knotless anchors. Heffernan et al 9 reported a PASTA repair technique using a knotless anchor. Those investigators used a spinal needle, but the angle of the needle was 30° relative to the skin surface in a wrist-to-shoulder direction. They tried to pass the nonabsorbable suture anteromedial and posteromedial to the PASTA lesion by using 1 spinal needle. If biceps pathology was present, Heffernan et al used a second nonabsorbable strand to pass the biceps and transverse humeral ligament simultaneously for biceps soft tissue tenodesis. They blindly tied the strands in the subacromial space to establish side-to-side tear closure. After tying, they fixed the strands using a lateral knotless anchor. Unlike Heffernan et al, we used 2 spinal needles simultaneously, one to create the loop and another to pass the loop. To pass the supraspinatus tendon vertically, we inserted the spinal needle near the anterolateral acromial corner at a vertical angle to the skin. We did not tie the strands in the subacromial space and thus did not make a side-to-side tear closure.
Gerber et al 8 reported the use of continuous musculotendinous traction to restore muscle changes in sheep. In their experimental study, the investigators cut the infraspinatus tendon of the sheep and 4 months later applied percutaneous muscle traction of 1 mm/d. After that, the investigators repaired the tendon and evaluated tendon quality using MRI scans, macroscopic dissection, histology, and electron microscopy. They found that elongation of the muscle can lead to restoration of normal muscle architecture in a tendon with a chronic tear. Therefore, degenerative muscle change after rotator cuff tear is highly associated with a decrease in tension.
In our technique, we restored the decreased tension of the intra-articular tendon portion by pulling the tendon to the lateral side. This might prevent degenerative muscle changes. The lateral anchor was positioned distal to the greater tuberosity, and the nonabsorbable strands compressed the PASTA lesion to the greater tuberosity, similar to the double-row transosseous tendon repair technique. Pulling from the medial side of the lesion can induce reattachment of the PASTA lesion to the footprint without obstacles. Although transtendon repair involves inserting the anchor just medial to the footprint, it can damage the normal footprint, and the anchor strands between the tendon and footprint can interfere in the healing process. 10 Moreover, with our procedure, the healthy bursal-side supraspinatus tendon was preserved without damage. If the spinal needle is placed accurately, it is an easy technique. Moreover, the number of anchors can be reduced.
Previous authors have reported good clinical results of transtendon repair for PASTA lesion. Rossi et al 21 analyzed 62 cases of transtendon repair for PTRCT and reported good long-term outcomes: FF, 172.2° ± 2°; PVAS score, 1.6 ± 1; and ASES score, 85.1 ± 5. Vinanti et al 26 performed a retrospective review of 100 patients with transtendon repair and good minimum 2-year outcomes: FF, 172.2° ± 8°; ER, 82° ± 14°; and PVAS score, 0.72 ± 1.33. In our study, we reported similar functional scores and lower ROM compared with previous studies: FF, 151.50° ± 20.33°; ER, 48.50° ± 17.55°; PVAS score, 1.00 ± 1.35; and ASES score, 85.96 ± 11.44. However, our study cannot be compared directly with previous studies because of differences in study design, such as sample size, follow-up duration, preoperative patient characteristics, and concomitant procedures.
Our study had several limitations. The sample size of this study was relatively small (24 patients). In addition, the follow-up duration was short (minimum 2 years), and many patients were contacted via telephone at final follow-up to collect functional scores. However, at postoperative 1-year follow-up, the number of comprehensive physical examinations was high (20/24; 83.3%). Moreover, we evaluated the postoperative 6-month MRI scans in 21 in 24 (87.5%) patients. Despite the high rate of telephone follow-up, the patients showed good functional scores at final follow-up, so we can cautiously report good ROM results at latest follow-up. Longer follow-up with physical examination will be necessary to clarify the clinical results of our procedure.
Another limitation was that despite good clinical outcomes, there were confounders in our results. During the operation, capsular release, subacromial decompression, subscapularis repair, and calcific deposit removal were performed concomitantly in 21, 18, 7, and 2 patients, respectively. Biceps tendon tenotomy and tenodesis were performed in 8 patients each. It was not clear whether good results were due to PASTA retensioning or additional procedures. However, PASTA lesions combined with other pathologies or symptoms, including external impingement and frozen shoulder, are generally observed. 22 That is a limitation of a retrospective study; hence, a prospective study comparing PASTA debridement and retensioning without concomitant procedures is needed.
There may be concerns regarding the integrity of the tendon portion healing to the footprint because we did not use an anchor and tying procedure. As the arm moves into ABD, the site will be detached and will not heal. We cannot argue against this possibility in patients without bracing or during early postoperative motion. However, in our study, patients wore a brace for at least 4 weeks postoperatively and were prescribed exercises with the arm limited to 20° to 30° of ABD while the brace was worn, so this could explain why we did not see such issues.
Conclusion
The retensioning technique in arthroscopic PASTA lesion repair showed improved ROM, pain, and functional scores and good tendon healing at the postoperative 6-month MRI follow-up in majority of patients. Thus, the retensioning technique can be a viable option for the treatment of the PASTA lesion. However, all other shoulder pathologies were addressed at the time of surgery.
Footnotes
Notes
Final revision submitted August 3, 2020; accepted August 18, 2020.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
This study was approved by the institutional review board at the Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Republic of Korea (2020-03-046-001).