
Abstract
Background:
The best surgical treatment option for symptomatic moderate- to high-grade articular-sided partial-thickness rotator cuff tears (PTRCTs) is still controversial.
Purpose/Hypothesis:
The purpose of this study was to evaluate patient-reported and clinical outcomes and tendon integrity after arthroscopic debridement or repair for PTRCTs at a minimum of 2 years postoperatively. We hypothesized that the overall outcomes would be positive, showing pain relief, good shoulder function, and high tendon integrity.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
We evaluated 30 patients (16 men, 14 women; mean age, 51 years) who underwent arthroscopic treatment for symptomatic PTRCTs (Ellman grades 2 and 3). Debridement was performed in 15 patients, and arthroscopic tendon repair was performed in the remaining 15 patients. Patients completed the Constant score; American Shoulder and Elbow Surgeons (ASES) shoulder score; Western Ontario Rotator Cuff Index; Simple Shoulder Test; and visual analog scale (VAS) for pain, function, and satisfaction. In addition, patients were examined clinically (range of motion, impingement tests, rotator cuff tests, and tests for the long head of the biceps tendon), and morphologic assessment of rotator cuff integrity was performed using direct magnetic resonance arthrography and was classified according to Sugaya.
Results:
The mean follow-up period was 55 months. The patient-reported outcome measures showed high patient satisfaction, reduction in persistent pain, and good shoulder function. Linear regression analysis showed that the debridement group had significantly better results on the Constant (bias-corrected and accelerated [BCa] 95% CI, 4.20-26.30), ASES (BCa 95% CI, 5.24-39.26), and VAS (pain: BCa 95% CI, 0.13-3.62; function: BCa 95% CI, 1.04-4.84; satisfaction: BCa 95% CI, 0.14-6.28) scores than did the repair group. At follow-up, there was no significant difference between the groups in clinical testing results. Good supraspinatus tendon integrity was seen in most patients: Sugaya classification grade 1 in 13 patients, grade 2 in 11 patients, and grade 3 in 6 patients.
Conclusion:
Midterm results after arthroscopic debridement and repair for PTRCTs showed high patient satisfaction, good shoulder function, and high tendon integrity for both procedures. Patients who underwent arthroscopic debridement had higher Constant, ASES, and VAS scores compared with patients who underwent tendon repair.
Partial-thickness rotator cuff tears (PTRCTs) are a common clinical entity and a frequent cause for shoulder pain and dysfunction. Ellman 6 described a classification system for PTRCTs according to lesion location (A, articular-sided; B, bursal-sided; C, intratendinous) as well as depth (grade 1, <3 mm [<25% of tendon thickness]; grade 2, 3-6 mm [25%-50% thickness]; and grade 3, >6 mm [>50% thickness]). Articular-sided PTRCTs occur more frequently than do bursal-sided PTRCTs. 9 In most cases, by tradition, the primary treatment is nonoperative and consists of physical therapy with strengthening of the intact rotator cuff, activity modification, avoidance of overhead tasks, nonsteroidal anti-inflammatory drugs, and subacromial corticosteroid injections. 7
If the conservative treatment fails, surgical treatment is often considered because progression of symptomatic PTRCTs to full-thickness rotator cuff tears can occur. 17,21 The arthroscopic debridement with or without subacromial decompression of low- and moderate-grade PTRCTs (Ellman grades 1 and 2, respectively) is a widely accepted procedure. 4,7,20,24,30 For high-grade PTRCTs (Ellman grade 3), an arthroscopic tendon repair is the favored surgical method. 27,30
Two different current techniques have been described to repair the latter rotator cuff tears: an in situ transtendon repair (partial articular supraspinatus tendon avulsion [PASTA] repair) 5,22,26,28,34 and a tear completion before repair of the tendon. 12,25 Some authors 23 prefer the tear completion technique in cases of nearly full-thickness (>90% of tendon thickness) rotator cuff tears. Biomechanically, the in situ transtendon repair technique has shown better results than has the tear completion technique for articular-sided partial supraspinatus tears. 10 Several recent studies have compared the clinical results of both techniques for high-grade PTRCTs. 2,8,14 In their randomized clinical trial, Castagna et al 2 described good results for both techniques without statistically significant differences. Comparable results were also found in a recent systematic review of Katthagen et al 14 and in a 3-year comparative prospective study of Franceschi et al. 8 The best surgical treatment option for symptomatic moderate- to high-grade articular-sided PTRCTs (Ellman grades 2-3) is debated, and the evidence is sparse. 3
The aim of this study was to evaluate the patient-reported outcomes (PROs), clinical examination results, and tendon integrity after arthroscopic treatment for symptomatic moderate- and high-grade articular-sided PTRCTs at a minimum of 2 years postoperatively. We hypothesized that (1) the midterm outcome after arthroscopic treatment of PTRCTs would show pain relief, good shoulder function, and high tendon integrity, and (2) the results of the tendon repair technique would be superior to those after debridement.
Methods
Patients
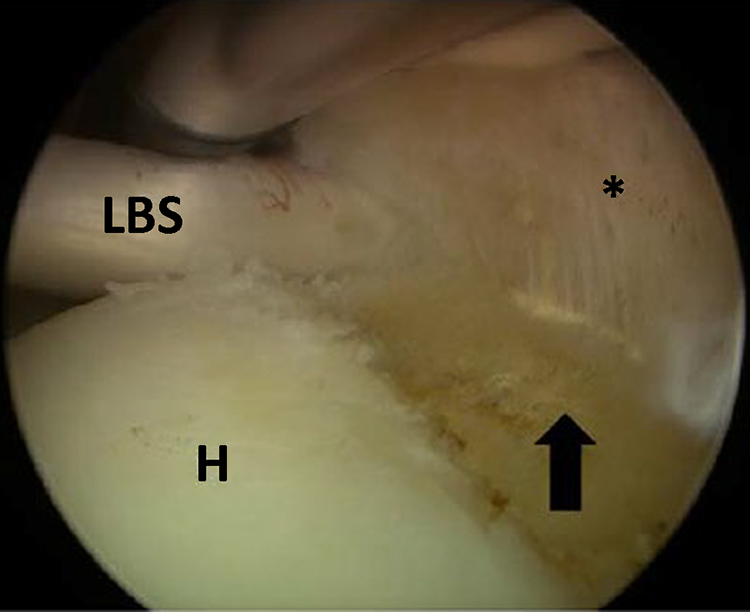
A total of 30 patients who underwent arthroscopic treatment for symptomatic PTRCTs in our institution were included in this retrospective study. The surgical treatment was indicated by the failure of nonoperative treatment for more than 12 weeks. Inclusion criteria were degenerative, articular-sided partial-thickness tears of the supraspinatus tendon (Ellman grade 2 or 3) confirmed arthroscopically (Figures 1 and 2) as well as arthroscopic treatment by tendon debridement or tendon repair (transtendon repair or tear completion before repair) (Figures 3 and 4). Exclusion criteria were Ellman grade 1 partial-thickness tear, bursal-sided partial-thickness tear, full-thickness rotator cuff tear, septic arthritis, adhesive capsulitis, previous shoulder surgery, history of trauma, or open rotator cuff repair. Relevant secondary diagnoses and associated procedures were extracted from the surgical report. A minimum follow-up period of 2 years was defined. This study was approved by the regional ethics committee, and written informed consent was obtained from all included patients.

Arthroscopic view from a posterior portal of a right shoulder showing a partial-thickness tear of the supraspinatus tendon (Ellman grade 2) (arrow). The asterisk indicates the supraspinatus tendon. H, humeral head; LBS, long head of the biceps tendon.

Arthroscopic view from a posterior portal of a right shoulder showing a partial-thickness tear of the supraspinatus tendon (Ellman grade 3) (arrow). The asterisk indicates the supraspinatus tendon. H, humeral head.
Arthroscopic view from a posterior portal of a right shoulder showing the footprint of the supraspinatus tendon after debridement of a partial-thickness tear (arrow). The asterisk indicates the supraspinatus tendon. H, humeral head; LBS, long head of the biceps tendon.
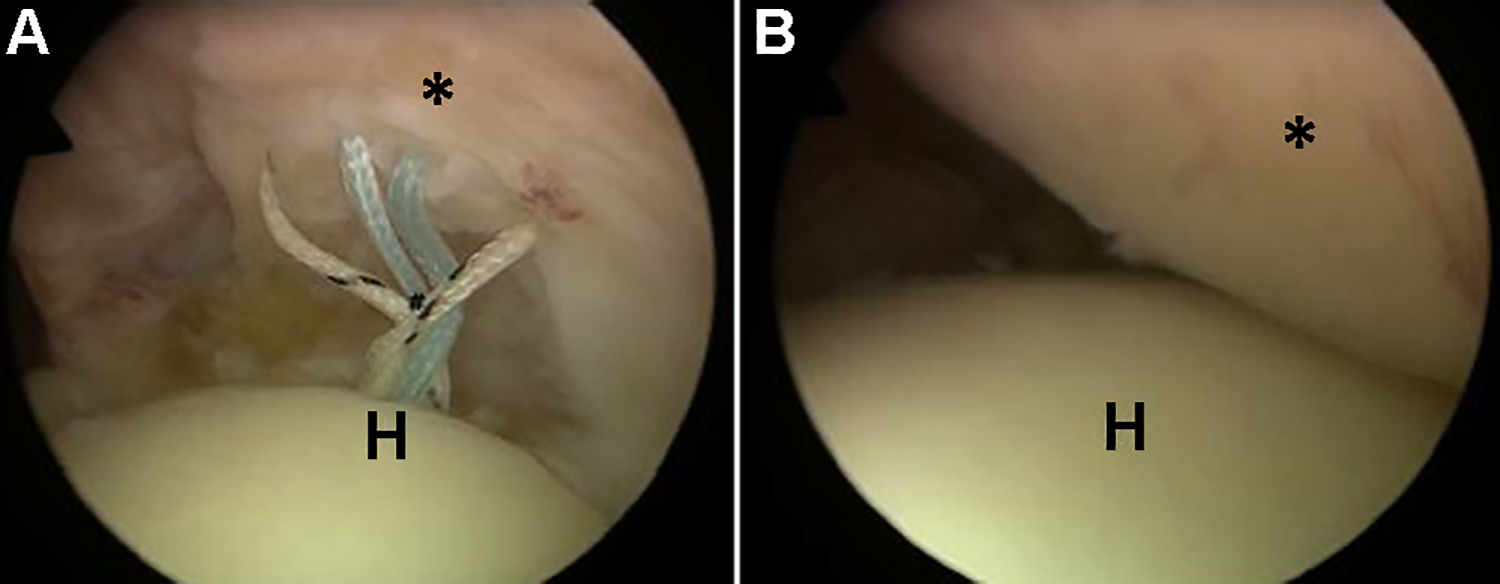
Arthroscopic view from a posterior portal of a right shoulder showing a PASTA (partial articular supraspinatus tendon avulsion) repair of a partial-thickness tear of the supraspinatus tendon (Ellman grade 3). (A) The sutures of a double-loaded anchor placed at the transition to the chondral surface of the humeral head (H) were shuttled through the intact supraspinatus tendon (*). (B) By tying the knots from the subacromial space, the supraspinatus tendon is adapted completely to its footprint.
Surgical Technique
Arthroscopic debridement was performed in 15 patients, and arthroscopic tendon repair was performed in 15 patients. All surgical procedures were performed with the patient in a beach-chair position under general anesthesia by the same surgeon (O.L.), who was specialized in shoulder arthroscopy. The following surgical technique was used consistently in all cases.
A standard posterior portal was used to perform the diagnostic arthroscopy and to detect concomitant pathologies. An additional anterior working portal was created in the rotator interval. An examination probe was introduced to evaluate the footprint of the articular-sided supraspinatus tendon and to measure the mediolateral tear size. The arthroscope was placed in the subacromial space to exclude a bursal-sided tear of the rotator cuff. Arthroscopic debridement of the supraspinatus tendon in cases of Ellman grade 2 PTRCTs was performed by introducing an arthroscopic soft tissue resector or an electrothermic device via the anterosuperior portal. The torn and frayed fibers of the tendon were resected, and the intact part of the tendon was preserved (Figure 3). For Ellman grade 2 lesions in patients evaluated with a positive preoperative 0° starter test (active abduction movement in 0° abduction position against resistance, pain, and weakness) and Jobe test (pain and weakness) as well as Ellman grade 3 lesions (>6 mm), arthroscopic repair was performed using either an in situ transtendon suture (PASTA repair) or, in cases of subtotal tears (>10 mm), a completion of the tear before repair.
For the in situ repair, 1 to 2 double-loaded bioresorbable suture anchors (5.5-mm Bio-Corkscrew; Arthrex) were placed transtendinous at the transition from the supraspinatus footprint to the chondral surface of the humeral head after preparation of the bony footprint. The sutures were shuttled through the intact supraspinatus tendon using a suture lasso (Figure 4A). The knots were tied from the subacromial space via an additional lateral portal. The refixation of the supraspinatus tendon to its footprint was checked again from an intra-articular view (Figure 4B). For the tear completion before repair, the PTRCT was completed to a full-thickness tear, and the supraspinatus footprint was debrided by using a shaver. The tendon repair was performed in a comparable fashion using same the anchor that was used for the in situ transtendon repair.
Associated procedures were performed if indicated. The indications for arthroscopic subacromial decompression with acromioplasty were positive preoperative impingement tests and additional arthroscopic findings as visible marks and/or osteophytes on the anterolateral undersurface of the acromion. After a subacromial bursectomy, the anterolateral surface of the acromion was planed, and any osteophytes were resected using a bur. Pathologies of the long biceps tendon (tendinitis, partial tear, instability, pulley lesions) were addressed using biceps tenotomy or tenodesis. In cases of labral lesions, labral debridement or repair was performed. Arthroscopic distal clavicle resection was performed for symptomatic arthritis of the acromioclavicular joint. Additional lesions of the subscapularis tendon were debrided or repaired if clinically symptomatic.
Postoperative Rehabilitation
All patients performed physical therapy for a minimum of 3 months postoperatively. The patients who underwent an arthroscopic tendon debridement were allowed to improve the range of shoulder motion, adapting for pain adapted without any limits. They were asked to avoid overhead tasks for 12 weeks postoperatively. The patients who had an arthroscopic tendon repair used a shoulder abduction brace for 6 weeks postoperatively. Within this time period, the range of motion was trained passively with a limit of 90° of abduction and flexion and 20° of external rotation. Afterward, the loading was increased with active assistance of the patients without limits for the range of motion. The full loading capacity of the shoulder was achieved between 3 and 6 months postoperatively.
PRO Measures
At follow-up, patients completed the following PRO measures: Constant score; American Shoulder and Elbow Surgeons (ASES) shoulder score; Western Ontario Rotator Cuff Index; Simple Shoulder Test; and visual analog scale (VAS) for pain, function, and satisfaction.
Clinical Examination
A clinical shoulder examination of the patients was performed at follow-up and included range of motion, impingement tests, rotator cuff tests (0° starter, Jobe, Patte, and lift-off tests), and tests for the long head of the biceps tendon (O’Brien test, palm-up test).
Tendon Integrity on Magnetic Resonance Arthrography
The structural integrity of the supraspinatus tendon was evaluated at follow-up via direct magnetic resonance (MR) arthrography (1.5-T MR image, Magnetom AERA; Siemens; contrast agent, Artirem). It was classified according to Sugaya et al 31 by 2 independent raters (M.B., O.L.) using oblique coronal, oblique sagittal, and transverse views of T2-weighted images (Table 1 and Figure 5).
Evaluation of Postoperative Rotator Cuff Integrity According to Sugaya Classification 31


Postoperative direct MR arthrography of 3 right shoulders (T2-weighted coronal views) showing (A) Sugaya type 1, (B) Sugaya type 2, and (C) Sugaya type 3. MR, magnetic resonance.
Statistical Analysis
Descriptive statistics for the quantitative analysis are reported as means ± SDs and ranges. The chi-square test and Fisher exact test were used for comparison of qualitative patient characteristics, and the unpaired t test and Mann-Whitney U test were used for the comparison of quantitative patient characteristics. The intraclass correlation coefficient was used to analyze the interobserver reliability of the 2 raters for the MR arthrography evaluation. All P values are 2-sided, and the level of significance was set at P <.05.
Linear regression analysis with bias-corrected and accelerated (BCa) CIs was performed to analyze the PRO score results at follow-up. Bootstrapping was conducted to fulfill model assumptions. All statistical analyses were performed using Microsoft Excel 2010 (Microsoft Corp) and IBM SPSS Statistics Version 24 (IBM Corp).
Results
Patients
The 30 study patients consisted of 16 men and 14 women with a mean age of 50.7 years. The mean follow-up period was 54.6 months. In 20 patients, an Ellman grade 2 partial-thickness tear of the supraspinatus tendon was diagnosed; the remaining 10 patients had a grade 3 partial-thickness tear. Further patient characteristics are shown in Table 2. Relevant secondary diagnoses included subacromial impingement (n = 20), pathologies of the long head of the biceps tendon (n = 15), labral lesion (n = 9), arthritis of the acromioclavicular joint (n = 7), partial-thickness subscapularis tear (n = 5), and pulley lesion (n = 3). The following associated procedures were performed: acromioplasty (n = 26), biceps tenotomy (n = 6), biceps tenodesis (n = 9), labral repair or debridement (n = 4), distal clavicle resection (n = 7), and subscapularis debridement or repair (n = 6).
Patient Characteristics of the Entire Cohort: Debridement versus Repair Subanalysis a
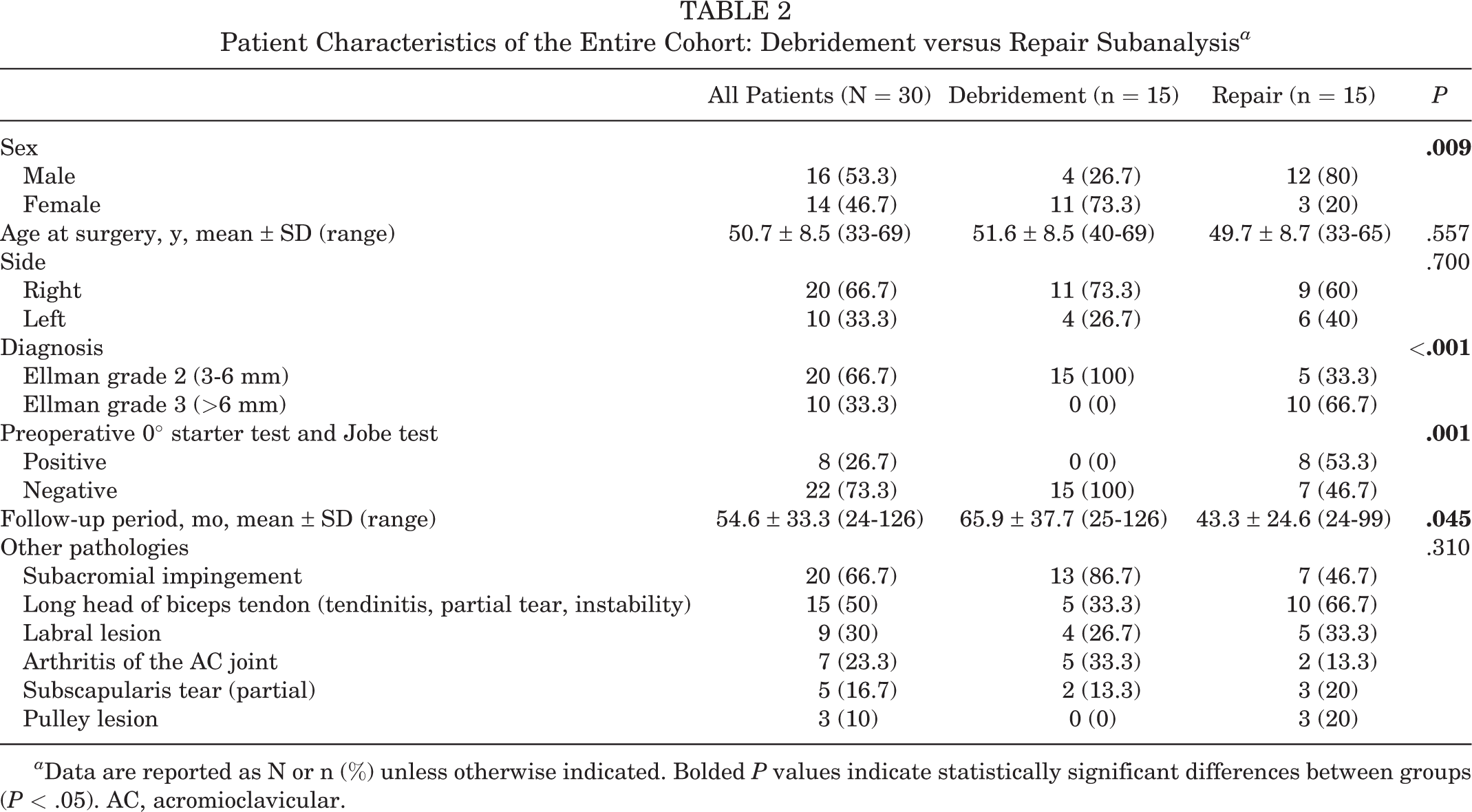
a Data are reported as N or n (%) unless otherwise indicated. Bolded P values indicate statistically significant differences between groups (P < .05). AC, acromioclavicular.
PRO Measures
At follow-up, the PRO scores showed overall improvement, with high patient satisfaction, reduction in persistent pain, and good shoulder function in both groups. One patient in each group had poor outcomes (Figure 6).

Patient-reported outcome results at follow-up: (A) Constant; (B) American Shoulder and Elbow Surgeons (ASES); (C) Western Ontario Rotator Cuff (WORC) Index; (D) Simple Shoulder Test (SST); and (E) visual analog scale (VAS) for pain, function, and satisfaction scores. The beginning and the end of the boxes were defined by the upper and lower quartile (25%). The line in the box shows the median (50%). The whiskers represent the minimum and maximum. The dots and numbers 10 and 30 indicate outliers.
The linear regression analysis was adjusted for the significant between-group differences in sex (P = .009) and follow-up period (P = .045). Analysis showed that the debridement group had significantly better results on the Constant score (BCa 95% CI, 4.20-26.30), the Constant score subsections for pain (BCa 95% CI, 1.21-6.25) and abduction strength (BCa 95% CI, 1.09-7.43), the ASES score (BCa 95% CI, 5.24-39.26), the Western Ontario Rotator Cuff Index score subsection A (BCa 95% CI, 2.92-221.95), and the VAS scores (pain: BCa 95% CI, 0.13-3.62; function: BCa 95% CI, 1.04-4.84; satisfaction: BCa 95% CI, 0.14-6.28).
Clinical Examination
The results of the clinical examination are shown in Figure 7. At follow-up, there was no significant difference between the groups in clinical testing results.

Results of the clinical examination at follow-up.
Tendon Integrity on MR Arthrography
There were 24 intact rotator cuffs, 6 partial-thickness tears, and no full-thickness tears of the rotator cuff on MR arthrography (Table 3). The interobserver reliability between the 2 raters was high (intraclass correlation coefficient, 0.94) showing strong agreement in the MR arthrography evaluation.
Tendon Integrity at Follow-up a

a Data are presented as N or n (%). SSP, supraspinatus.
b According to Sugaya classification. 31
Discussion
The most important results of this study were a high patient satisfaction as seen on PRO scores, good shoulder function in the clinical examination, and high tendon integrity on MR arthrography at midterm follow-up after arthroscopic treatment of PTRCTs (Ellman grade ≥2). A subanalysis revealed better results for some PROs in patients who underwent an arthroscopic debridement; however, there were no significant differences between the debridement and repair groups regarding clinical examination results or tendon integrity on MR arthrography.
Some evidence could be found in the current literature that PTRCTs had a low potential for spontaneous healing. Yamanaka and Matsumoto 37 and Kim et al 17 described a tear progression for PTRCTs after conservative treatment. Moreover, this is supported by the results of histological studies 9,36 showing no evidence for a repair process of the injured tendon. Therefore, it is reasonable to indicate an arthroscopic treatment for symptomatic PTRCTs if the nonoperative treatment fails. Following the discussion in the literature about the best surgical treatment of symptomatic PTRCTs, there is still no consensus, and the evidence is limited. 3 The current recommendation for PTRCTs involving <50% of the tendon thickness is to perform an arthroscopic debridement, 4,20,24,30,35 and an arthroscopic repair (transtendon repair or tear completion before repair) is favored in cases of PTRCTs involving >50% of the tendon thickness. 5,14,27,28,30,34
Liem et al 20 found good to excellent clinical results in the midterm to long term after subacromial decompression and debridement without repair for Ellman grades 1 and 2 articular-sided PTRCTs. The present study showed the results of arthroscopic debridement for Ellman grade 2 articular-sided PTRCTs, and they were in line with those results showing high patient satisfaction and good shoulder function in the midterm. In our study, an additional arthroscopic acromioplasty was performed in almost all (26/30) patients. The outcome for arthroscopic debridement of PTRCTs involving >50% of the tendon thickness is worse and inferior to the results for PTRCTs involving <50% of the tendon thickness. Weber 35 analyzed the clinical results of arthroscopic debridement and subacromial decompression in patients with high-grade PTRCTs (Ellman grade 3) and described poorer results for bursal-sided compared with articular-sided tears. Cordasco et al 4 and Kartus et al 13 also reported poorer results for bursal-sided compared with articular-sided PTRCTs (Ellman grade 1 or 2). In contrast to this, Park et al 24 found better results for bursal-sided compared with articular-sided PTRCTs. In addition to those clinical results, Kartus et al 13 showed further degeneration of the rotator cuff using ultrasound evaluation in the long term after arthroscopic debridement and acromioplasty in patients with PTRCTs. Therefore, it might be questionable whether a tendon debridement with or without acromioplasty could have a positive effect on the degenerative process of the rotator cuff. In contrast to that, a recent study of Kong et al 19 showed that tear progression is not as common as described in previous studies and that some tears healed or reduced in size. The results of this study also showed no relevant further degeneration of the rotator cuff with progress to full-thickness tears in the midterm after tendon debridement and acromioplasty for PTRCTs involving <50% tendon thickness.
The findings of the current study are in line with previous studies. 2,5,16,22,26,32,33 Kim et al 16 reported significant functional improvements after arthroscopic repair of both articular-sided and bursal-sided PTRCTs, with no significant difference between groups. Ostrander et al 22 found reliable tendon healing and excellent functional outcomes for the transtendinous repair of PTRCTs. Our clinical examination results are in line with those of Ranalletta et al, 26 Vinanti et al, 33 and Vap et al, 32 all of whom reported excellent clinical outcomes at midterm follow-up for patients undergoing arthroscopic repair of PTRCTs. Castagna et al 2 compared the clinical outcome after transtendon repair with the results of tear completion before repair. In their randomized clinical trial, they found good results with improvement of function and pain reduction at a minimum follow-up period of 2 years. Both techniques did not show statistically significant differences. In contrast to our study, the morphologic integrity of the rotator cuff was not analyzed at follow-up. Other studies 8,14,18,27 have also confirmed these good clinical results. Duralde and McClelland 5 described reliable improvements in pain and function for patients who underwent a transtendinous repair for grade 3 articular-sided PTRCTs. Kim et al 15 found comparable to superior postoperative functional results for bursal-sided PTRCTs compared with those for articular-sided PTRCTs after arthroscopic conversion to a full-thickness rotator cuff tear.
In contrast to the hypothesis of the study, the tendon repair showed no significant difference for the clinical testing results and for the tendon integrity in direct MR arthrography at follow-up compared with the tendon debridement. Furthermore, the debridement group had better results on the Constant, ASES, and VAS scores compared with the repair group. This underlines that tendon debridement in cases of moderate-grade PTRCTs (Ellman grade 2) is a reasonable and adequate treatment option. In clinical practice, we tend to perform a tendon repair for PTRCTs (Ellman grade 2) with a positive preoperative Jobe test and 0° starter test, especially in cases of PTRCTs that are borderline Ellman grade 3 lesions, but this is not supported by the results of our study.
The diagnostic accuracy of MR imaging (MRI) for detecting PTRCTs is limited. A recent study 1 showed a sensitivity of 51.6% and a specificity of 77.2%. Direct MR arthrography provides higher accuracy compared with native, noncontrast MRI. 11,29 In order to achieve the most valid morphologic results, this study evaluated the integrity of the rotator cuff at follow-up using direct MR arthrography. Other studies that analyzed the repair integrity of the rotator cuff after arthroscopic treatment for PTRCTs have used ultrasound 13,15,20,22 or noncontrast MRI. 8,15,27 Therefore, the accuracy of those results is limited. The present study showed a high tendon integrity after arthroscopic debridement and repair of PTRCTs via direct MR arthrography.
Limitations
There are several limitations to this study. First, it was a retrospective study design. Preoperative data on the PROs and the MR arthrography were not available. Therefore, it remains unclear if the patients significantly improved from preoperative to postoperative status. In addition, it is also not known if the integrity of the rotator cuff improved, worsened, or remained the same. Second, the number of included patients was limited. However, compared with other recent studies, the number of patients (n = 30) was sufficient and acceptable to answer the research question. A post hoc power analysis showed a large effect (Cohen r 2 > 0.260) for all statistically significant group differences regarding the PROs (Constant score, r 2 = 0.315; ASES score, r 2 = 0.310; VAS pain score, r 2 = 0.274; VAS function score, r 2 = 0.286) except for VAS satisfaction (r 2 = 0.229). The small groups made cohort comparisons difficult and a high likelihood of type 2 error possible. Third, the 2 treatment groups differed significantly with respect to sex and the follow-up period in months. Interestingly, women were represented more in the debridement group. Therefore, the linear regression model was adjusted to those parameters. Nevertheless, the comparability of both groups is limited not least because of a different distribution of Ellman grade 2 and grade 3 lesions. Fourth, the results of the study represent the midterm outcome after arthroscopic treatment for PTRCTs; long-term results are lacking and should be the focus of further research. Fifth, it is unknown how much of the clinical outcome is due to the arthroscopic treatment of PTRCTs separate from the treatment of the other shoulder pathology. An additional arthroscopic acromioplasty was not performed in all patients.
The strengths of this study are the conclusive methods used including the use of reliable shoulder scores, a detailed clinical examination, and a high accuracy for the detection of the tendon integrity via direct MR arthrography. The follow-up was performed at a minimum of 2 years postoperatively, and the mean follow-up time was 55 months, representing the midterm outcome. To the best of our knowledge, this is the first study to analyze the tendon integrity after arthroscopic debridement or tendon repair for symptomatic PTRCTs via direct MR arthrography, providing a higher diagnostic accuracy compared with ultrasound or native MRI. The results were in line with current treatment recommendations to perform an arthroscopic tendon debridement for symptomatic PTRCTs involving <50% of the tendon thickness (Ellman grade 2) and an arthroscopic tendon repair for symptomatic PTRCTs involving >50% of the tendon thickness (Ellman grade 3). Both procedures resulted in high patient satisfaction, good shoulder function, and high tendon integrity on MR arthrography at midterm follow-up.
Conclusion
Midterm results after arthroscopic debridement and repair for PTRCTs showed high patient satisfaction, good shoulder function, and high tendon integrity for both procedures. Patients who underwent arthroscopic debridement had higher Constant, ASES, and VAS scores compared with patients who underwent tendon repair.
Footnotes
Final revision submitted September 1, 2020; accepted September 10, 2020.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Saarland Medical Association (identification No. 72/15).