
Abstract
Background:
Juvenile idiopathic arthritis (JIA) is a heterogeneous group of chronic arthritides presenting in patients aged ≤16 years, with a prevalence of 16 to 150 per 100,000. Juvenile osteochondritis dissecans (OCD) is an idiopathic disease of articular cartilage and subchondral bone, has an onset age of 10 to 16 years, and often affects the knee, with a prevalence of 2 to 18 per 100,000. Currently, there are few studies that have evaluated the relationship between JIA and OCD.
Hypothesis:
OCD is more prevalent in children with JIA, and when diagnosed in such patients, OCD often presents at an advanced state.
Study Design:
Case series; Level of evidence, 4.
Methods:
The medical records of patients with diagnoses of both JIA and OCD treated between January 2008 and March 2019 at a single children’s hospital were retrospectively reviewed. Associations between timing of diagnoses, number and types of corticosteroid treatments, category of arthritis, timing of diagnoses, and lesion stability were examined with Spearman correlation coefficients.
Results:
A total of 2021 patients with JIA were identified, 20 of whom (19 female, 1 male) had OCD of the knee and/or talus for a prevalence of 1 in 100 or 1000 in 100,000, or approximately 50 to 500 times that of the general population. These 20 patients had a total of 28 OCD lesions: 43% (9 femur, 3 talus) were radiographically stable over time, 50% (10 femur, 2 patella, 2 talus) were unstable at initial diagnosis, and 7% (2 femur) were initially stable but progressed to unstable lesions despite drilling. Twelve patients (60%) underwent surgery: 4 (20%) with stable femoral lesions for persistent symptoms despite prolonged nonoperative treatment and 8 (40%) for treatment of their unstable lesions (femoral and patellar). Within our study design, we could identify no significant associations between lesion stability and timing of diagnoses, number of joint injections, or limb deformities, nor were there associations between timing of JIA and OCD diagnoses and category of arthritis.
Conclusion:
In our population of patients with JIA, OCD lesions were found to be 50 to 500 times more prevalent when compared with published rates in the general population and often presented at an advanced state, with instability or delayed healing requiring surgery for stabilization or resolution of symptoms.
Keywords
Juvenile osteochondritis dissecans (OCD) is a disorder of subchondral bone in skeletally immature patients of unclear cause that may include repetitive microtrauma, a vascular insult, or a genetic predisposition. 9 OCD lesion instability can lead to separation of the subchondral bone segment from the articular surface, leading to mechanical symptoms and potentially premature osteoarthritis. The distal femur is the most commonly involved site, although the talus and capitellum are also common sites for OCD. 12,13 The prevalence of knee OCD may be lie between 2 and 18 per 100,000, depending on age and sex. 13 Boys are more commonly affected than girls, with ratios of 2:1 to 4:1, respectively, depending on the population studied. 13,17
Juvenile idiopathic arthritis (JIA) is a heterogeneous group of chronic arthritides in children ≤16 years of age, with a prevalence of 16 to 150 per 100,000. 23 JIA is divided into several mutually exclusive categories, each with different genetic factors, presentations, and manifestations; however, the cause of JIA remains unknown. Treatment of JIA includes disease-modifying antirheumatic drugs (eg, methotrexate), corticosteroids (oral or intra-articular), and targeted biological agents. While JIA remains a clinical diagnosis, in recent years, efforts to improve both the quality and utility of the imaging of the synovium and articular cartilage have been made. Ultrasonography offers a low-cost means to assess for synovitis and cartilage thickness, 18 as well as to identify erosions of bone, while magnetic resonance imaging (MRI) confers a specific advantage in patients with JIA in evaluating synovitis, cartilage, and early pre-erosive bone lesions. Hence, it is more clinically informative than plain radiography or ultrasound. Current practice frequently involves the use of ultrasound as well as MRI for the diagnosis and monitoring of JIA progression. 4,7,8
In the evaluation of joint pain in patients with JIA, OCD lesions have recently been identified as more common and often more severe than typically seen in the general population. 11,15,16 Further understanding of the prevalence and presentation of OCD in patients with JIA may improve monitoring plans and treatment recommendations for affected patients. 15 We hypothesized that OCD is more prevalent in children with JIA than published rates in children in the general population, and when diagnosed in such patients, OCD is often first identified in an advanced state.
Methods
Patient Selection
Institutional review board approval was obtained before the initiation of this retrospective study. Medical records dating from between January 2008 and March 2019 in the departments of rheumatology, orthopaedics, and radiology at a single tertiary-care institution were queried to identify patients diagnosed with JIA and OCD using the International Classification of Diseases, 9th and 10th Revision codes. Cross-referencing the 2 lists was performed to identify the 20 patients included here. Included were patients diagnosed with or treated for JIA by rheumatologists, treated in orthopaedics for OCD confirmed by radiologists, and 21 years of age or younger. Patients who were diagnosed with JIA or OCD after March 2019 or diagnosed with OCD but not JIA were excluded.
Our institution is 1 of 2 medical centers specializing in the care of children across a 5-state area. Rheumatologists and orthopaedists see patients in regional clinics in each of these states, with records and surgical care performed at our main hospital campus. Patients with JIA have not routinely undergone a skeletal survey, nor have they universally undergone radiographic imaging of symptomatic joints. Only records of patients with JIA diagnosed with OCD by radiologists and confirmed by orthopaedists were reviewed by the study team. All patients except 1 were long-standing patients in our rheumatology clinics referred to orthopaedics for additional care. Given our position as a tertiary referral center for a multistate region, no estimates of the prevalence of JIA or OCD in our community were made from our populations of patients; we have referred to published rates for both.
Data Collection
Data collected from the electronic medical record (EMR) included patient information, age at JIA diagnosis, arthritis category, corticosteroid use, and age at OCD diagnosis. OCD lesion site, stability, surgery performed, time to healing or further treatment, and concurrent potentially related diagnoses (limb deformities, discoid meniscus, other) were determined from reviews of patient EMRs and picture archiving and communications system imaging files. A retrospective assessment of lesion stability was performed by the lead author (A.H.) and confirmed by the senior author (G.A.S.) using modified MRI criteria 5,6,14,24,25 with lesions categorized as likely stable or likely unstable. Lesions were classified as likely unstable when high T1 or T2 signals were present at the fragment interface and/or cystic lesions were noted beneath the fragment. This method was more sensitive in characterizing lesion stability in a pediatric cohort, 14 in particular when T2 sequences of the progeny-parent interface and T1 sequences focusing on the articular cartilage were both taken into consideration. Unstable lesions displayed a high T2-signal intensity line surrounding the lesion with either the same signal intensity as the surrounding synovial fluid, a high T2-signal intensity rim, or several subchondral bone breaks; a fluid-filled cartilage defect; the presence of subchondral cysts or a cyst larger than 5 cm; and a T1-signal break in the articular cartilage surface. As unstable lesions herald a poorer prognosis for the knee than stable lesions, including a low likelihood of healing without surgery and a higher likelihood of early arthritis, 9 we termed lesion instability a sign of severe disease.
Treatments and outcomes were reviewed, including time to healing and whether radiographic evidence of healing was present at the most recent patient follow-up. The presence of concurrent pathologies, including genu valgum, discoid meniscus, torn meniscus, or the loss of cartilage elsewhere, was also noted, and all data were recorded in an Excel (Microsoft) file.
Statistical Analysis
Descriptive statistics were used to summarize the differences between types of JIA. Associations between lesion stability and timing of diagnoses, number of corticosteroid joint injections, or limb deformities, and category of arthritis and timing of diagnoses were examined with Spearman correlation coefficients. P ≤.05 was considered significant. All analyses were performed using Stata (Version 14.0; StataCorp).
Results
During the period of interest, 2021 patients diagnosed with JIA were identified. Of these, 19 girls and 1 boy were found to have symptomatic OCD lesions, yielding an approximate prevalence of 1000 in 100,000. Given the accepted prevalence of OCD in all boys and girls aged 6 to 19 years to be 2 to 18 per 100,000, 13 it follows that the prevalence of OCD in children with JIA in our sample of patients with JIA is approximately 50 to 500 times that of children overall, as reported in the literature. The mean age (±SD) of these 20 patients at the time of the JIA diagnosis was 6.5 ± 3.7 years. Six had oligoarticular JIA (<5 involved joints), 7 had extended oligoarticular JIA (<5 joints involved in the first 6 months after diagnosis followed by extension to 5 or more joints after the first 6 months), 4 had polyarticular JIA (>5 joints involved in the first 6 months after diagnosis), and 3 had enthesitis-related JIA (inflammation at multiple joints and tendon insertions) (Tables 1 and 2). The mean age of the patients at the time of OCD diagnosis was 12.4 years (range, 7.2 to 19.3 years). The mean time between JIA and OCD diagnoses was 6 years (range, –3.7 to 17.4 years; 1 patient was diagnosed with OCD before JIA). Three of the 20 patients were skeletally mature at the knee at the time of their OCD diagnosis, although given their age at diagnosis and the degree of progression toward instability of lesions seen, the onset of OCD for each was undoubtedly before skeletal maturity.
Patient Characteristics a
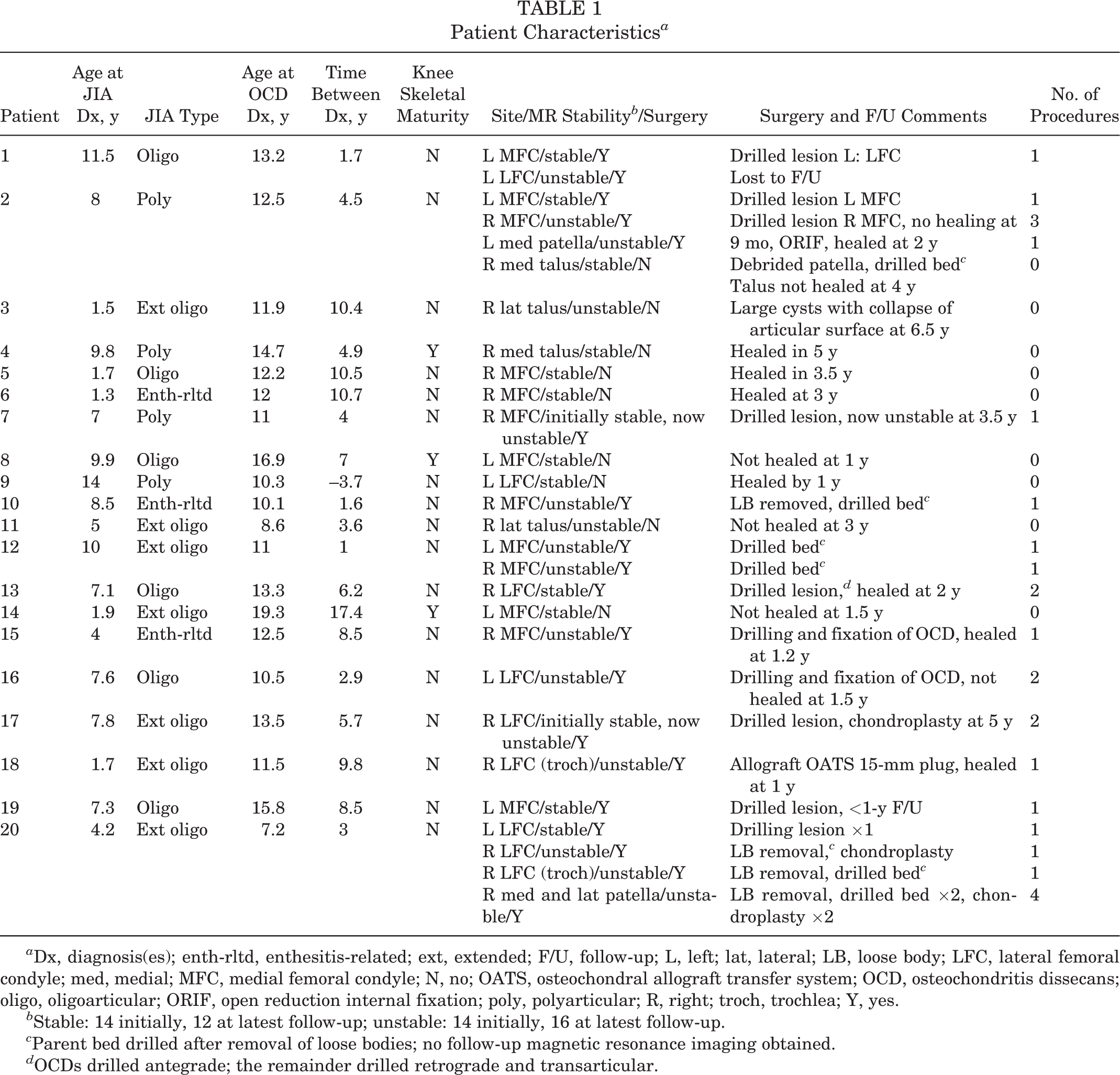
a Dx, diagnosis(es); enth-rltd, enthesitis-related; ext, extended; F/U, follow-up; L, left; lat, lateral; LB, loose body; LFC, lateral femoral condyle; med, medial; MFC, medial femoral condyle; N, no; OATS, osteochondral allograft transfer system; OCD, osteochondritis dissecans; oligo, oligoarticular; ORIF, open reduction internal fixation; poly, polyarticular; R, right; troch, trochlea; Y, yes.
b Stable: 14 initially, 12 at latest follow-up; unstable: 14 initially, 16 at latest follow-up.
c Parent bed drilled after removal of loose bodies; no follow-up magnetic resonance imaging obtained.
d OCDs drilled antegrade; the remainder drilled retrograde and transarticular.
Characteristics and Stability of OCD Lesions by Type of Arthritis a

a Data are presented as number or mean ± SD. JIA, juvenile idiopathic arthritis; OCD, osteochondritis dissecans.
These 20 patients had a total of 28 OCD lesions: 43% (9 femoral, 3 talar) were radiographically stable over 1 to 5 years, 50% (10 femoral, 2 patellar, 2 talar) were unstable at initial diagnosis, and 7% (2 femoral) were initially stable and progressed to unstable despite drilling over 1 to 5 years (Figure 1). Twelve patients (60%) underwent surgery: 4 (20%) with stable femoral lesions for persistent symptoms despite prolonged nonoperative treatment and 8 (40%) for treatment of their unstable lesions (femoral and patellar). Of these 12 patients, 3 underwent 2 or more surgeries for OCDs, and 3 were treated with hemiepiphysiodesis for concomitant genu valgum. We could not identify any significant associations between JIA category and stability of lesions, nor between times of JIA or OCD diagnosis and stability of lesions (Spearman ρ = –0.37; P = .11).

Distribution of lesions by location and stability.
Patients received varying doses and routes of steroids over the course of the disease, including intravenous methylprednisolone pulses (range, 0-62), oral prednisone either as tapers for flares (range, 0-4 bursts) or as daily oral prednisone (range, 0-105 days), and intra-articular steroids (range, 0-5 times). There were no associations between instability of lesions and number of doses of steroids by any of these 3 routes (Spearman ρ = 0.20; P = .44).
Discussion
The results of this study confirm prior reports indicating that the prevalence and severity of OCD in JIA are likely higher than in the general population. 11,16 As such, JIA should be considered a risk factor for the development of OCD. In the general population, OCD displays a higher incidence in men, and knee lesions are reported almost 4 times more often in pediatric male than female patients. 13 In this study, the prevalence of juvenile OCD in patients with JIA was 50 to 500 times that reported for the general population when compared with the published rates, 13 and nearly all of the patients were female (19/20). The higher frequency of female patients with JIA and OCD (9/13) was also seen in the report by Kroger et al 15 and has been reported by others as well. 11 In their case series of 13 patients with JIA and OCD, Kroger et al reported symptomatic joints without evidence of synovitis yet unstable lesions or mechanical symptoms leading to surgery in 7 (54%) of their patients. 15 Jackson et al, 11 in their case series of 10 patients, reported that 6 (60%) underwent surgery for mechanical symptoms or instability, similar to the 60% operative rate for persistent symptoms or unstable lesions in this study. Kubo et al 16 also found a proportionally higher prevalence of unstable lesions in patients with JIA in an age-matched study of OCD in patients with and those without JIA. Unlike previous studies, our review allowed us to establish a prevalence of OCD among 1 institution’s population of patients with JIA.
While the cause of OCD is unknown, genetic factors, trauma, and ischemia have all been proposed. 9,17 Prior reports also suggest that cartilage thinning is evident in JIA. 1,18,22 It is unclear what predisposes patients with JIA to thinning of the cartilage, as this was not dependent on disease duration; however, a synergistic effect between the processes of chronic inflammation and thinning of cartilage may be hypothesized. 18,22 Chronic injury to articular cartilage due to ongoing or intermittent inflammation may predispose patients with JIA to the higher incidence of OCD, as thinned cartilage may be less resistant to minor trauma, ischemia, or abnormal joint mechanics. 11 Recent veterinary medicine studies suggest that these lesions likely have an early onset in animals as a result of focal failure of cartilage canal blood supply that produces ischemic necrosis. 19 –21 A similar cause may follow in humans, though a connection between systemic inflammation and localized vascular insults in developing bone is not clear.
Within the limitations of our study, we were unable to detect any significant associations between the stability of lesions and exposure to steroids or category of JIA, although no patients with psoriatic or systemic JIA were found to have OCD. The hazards of intra-articular injection of steroids to articular cartilage have been shown in animal models, 2,3 although others have suggested that these injections in arthritis patients result in clinical improvements without negatively affecting vascularity in periarticular tissues. 10 Again, studies by Olstad et al 19 –21 suggest that the initiation of OCD may occur early in joint development, long before the initiation of steroid treatments.
Although we found no association between time of JIA diagnosis and OCD stability, the high number of unstable lesions suggests that the diagnoses of OCD were often made late. We believe that earlier diagnosis would likely lead to a greater probability of detection at a stage of lesion stability, which would be a better prognostic sign for long-term health of the knee. 9 Retrospective MRI classification of OCD lesions indicated a relationship between those lesions classified as likely unstable and their eventual need for surgical intervention. With the understanding of the clinical relationship between OCD and JIA, the use of imaging modalities more suited for OCD diagnosis and classification may indicate surgical intervention in patients previously treated medically. 7 This study demonstrates the importance of thorough assessment of joint pain in patients with JIA, particularly those with pain yet a lack of signs of current inflammation, as noted by Kroger et al 15 and Jackson et al. 11 Early detection would more likely identify patients with stable lesions, conferring a better prognosis for the long-term health of the knee.
Limitations
This review assumes that all patients with JIA and OCD underwent radiographic imaging that revealed their OCD lesions. However, this would be a confirmation bias that would lead us to potentially underestimate the true prevalence of OCD in our cohort of patients with JIA. We did not examine radiographs of every patient diagnosed with JIA, and, in addition, we reviewed only the records of those patients with OCD who were seen in both the rheumatology and orthopaedics departments. Patients with JIA do not routinely undergo skeletal surveys; only symptomatic joints are typically imaged, which, again, may lead to an underestimation of the prevalence of OCD in JIA.
Patients with JIA may also undergo more routine radiographic imaging than the general population, suggesting potential underestimation of the true background prevalence of OCD in the population at large, as previously published. 13 In addition, we have made no attempt to estimate the prevalence of OCD or JIA in our local population, choosing to refer to previously published rates. As a tertiary referral center, our population of patients is likely not a fair representation of children throughout the Pacific Northwest. Kessler et al 13 would provide a better estimate of the prevalence of OCD in children, as their sample included all patients treated over a 4.5-year period at Kaiser Permanente of Southern California, an integrated health system serving more than 3.5 million patients. Were OCD to be more prevalent in the Pacific Northwest than in the population described by Kessler et al, 13 our estimate of increased rates of OCD in patients with JIA would be exaggerated. As we did not review steroid exposure in patients with JIA free of OCD, we were unable to assess whether steroid exposure increased the risk of OCD in patients with JIA; we examined only whether high oral or intravenous steroid exposures were associated with lesion instability. Within the limitations of our study, no associations were found.
Conclusion
In our population of patients with JIA, OCD lesions were found to be 50 to 500 times more prevalent when compared with published rates in the general population and often presented at an advanced state, with instability or delayed healing requiring surgery for stabilization or resolution of symptoms. Increased commitment to early imaging in the context of joint pain in patients with JIA may lead to early diagnosis of OCD lesions, improved quality of care, and better outcomes.
Footnotes
Final revision submitted August 5, 2020; accepted August 10, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: S.S. is on the advisory board for Novartis and the adjudication committee for Pfizer. M.T. has received consulting fees from Siemens Medical. M.G.S. has received grant support from DJO, research support from Arthrex, and education payments from Arthrex and Smith & Nephew. G.A.S. has received education payments from Arthrex and SIGN Fracture Care International. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Seattle Children’s Hospital (ID 00001718).