
Abstract
Background:
The occurrence of rapid chondrolysis after partial lateral meniscectomy is rare. The pathophysiology, risk factors, and outcomes of treatment have not been established.
Purpose:
The primary aim of this study was to perform a scoping review of the literature to determine the potential risk factors and pathogenesis of rapid chondrolysis. The secondary objective was to report outcomes of treatment.
Study Design:
Systematic (scoping) review.
Methods:
A scoping review of the literature was conducted in accordance with the framework of Arksey and O’Malley. A search strategy based on the terms “chondrolysis” AND “knee,” “chondrolysis” AND “meniscus,” and “chondral damage” AND “lateral meniscus” was applied to the PubMed database on March 31, 2020. All relevant studies were included. Patient demographics and clinical data were extracted from these studies and analyzed in order to investigate the potential risk factors, pathogenesis, and outcomes of treatment for rapid chondrolysis.
Results:
Five articles (22 cases) featuring rapid chondrolysis in the lateral compartment after partial lateral meniscectomy were identified and included. The condition occurred most frequently in patients who were young (mean age, 25.6 years), male (20/22 cases; 91%), and participating in high-intensity sports (19/22 cases; 86.4%) within 1 year of the index procedure. Half of the included study population underwent surgery for a radial tear. All professional athletes (13/13) returned to the preinjury level of sport. All authors of included studies suggested that the main causal risk factor was mechanical focal cartilage overload in the lateral compartment of the knee.
Conclusion:
Rapid chondrolysis after partial lateral meniscectomy is a rare condition that typically occurs within 12 months of the index procedure. Younger age, male sex, high-intensity sports participation, and some meniscal tear patterns (eg, radial tear) are potentially important risk factors. Return-to-sport rates at short-term follow up are high, but no long-term studies were identified. The pathogenesis of rapid chondrolysis seems to relate to mechanical focal cartilage overload.
Treatment of meniscal tears with arthroscopic meniscectomy is among the most frequently performed procedures in orthopaedic surgery. Partial lateral meniscectomy (PLM) performed in stable knees is associated with high satisfaction rates (>95%) 9 and a high number of symptom-free patients (79.9%) at a minimum follow-up of 10 years. 9 There are also numerous studies reporting favorable outcomes at short-term follow-up. 20,21,29,36 However, in contrast to these generally good results, there are reports of rapid chondrolysis (RC) after PLM. 2,8,19,22,35
Chondrolysis of the knee after PLM refers to rapid loss of articular cartilage in the lateral compartment, resulting in knee pain and persistent swelling. 2,8,19,22,35 Figure 1 demonstrates the typical radiological features and arthroscopic findings associated with RC in a 22-year-old soccer player who had undergone PLM of the right knee (at another institution) 8 months before presentation to our clinic. He had a history of persistent pain and swelling. There was no evidence of ligamentous injury, and he had normal limb alignment.

(A) Clinical suspicion of rapid chondrolysis was raised because radiographs (Schuss views) demonstrated 30% narrowing of the lateral compartment joint space as compared with the left knee (lateral compartment joint space, 7.5 mm in the left knee and 5.3 mm in the right). (B) Furthermore, magnetic resonance images at the same time demonstrated evidence of previous lateral meniscectomy and effusion. The patient went on to have arthroscopic evaluation, which revealed (C, D) abundant loose cartilaginous debris, (E) Outerbridge grade 4 changes on the lateral femoral condyle, and (F) grade 3 changes on the lateral tibial plateau.
The occurrence of this condition gives rise to the juxtaposition of typically excellent outcomes in the majority of patients who undergo this frequently performed procedure versus this rare complication of undefined etiology and unknown risk factors.
The primary aim of this scoping review was to examine the extent, range, and quality of the evidence available to explain the pathophysiology and potential risk factors for RC after PLM. The secondary aim was to report outcomes of treatment for RC.
Methods
A scoping review of the literature was conducted in accordance with the methodological framework of Arksey and O’Malley 3 and the PRISMA-ScR (Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews). A scoping review methodology was selected because this approach is considered to have great utility for addressing an exploratory research question. However, some limitations with this methodology can lead to a broader and less defined approach and some inconsistencies with the search that will require larger teams to review the search results. 3,10,24 The study protocol was prospectively registered with the Open Science Framework study registry before commencing data collection.
The 5-stage methodological framework of Arksey and O’Malley 3 comprises the following steps: (1) identification of a research question; (2) identification of the relevant studies; (3) the selection of studies to be included in the review; (4) data extraction from the included studies; and (5) collating, summarizing, and reporting of the results of the review.
Identification of the Research Question
The research question was as follows: What is known from the existing literature regarding the pathophysiology and risk factors for RC after PLM?
Identifying Relevant Studies
Relevant studies were identified by applying the search strategy to the PubMed database. This comprised the following keywords with automatic mapping to Medical Subject Headings terms: “chondrolysis” AND “knee,” “chondrolysis” AND “meniscus,” and “chondral damage” AND “lateral meniscus.” The search was conducted on March 31, 2020, by 2 independent investigators (C.P. and V.K.). Both investigators reviewed the titles and abstracts of all identified records, and potentially eligible articles were retrieved for full-text review. The reference lists of articles included at the full-text review stage were screened to identify any additional eligible studies for review.
Study Selection
All identified clinical studies and case series reporting RC after lateral meniscal tear and/or PLM were included. Articles were excluded only if a history of inflammatory arthritis or intra-articular local anesthetic administration was reported, because each is recognized to be independently associated with RC. 7,13,27,30 Disagreement between reviewers regarding study eligibility was resolved through discussion with the senior author (B.S.-C.).
Data Extraction
The following data were extracted from each study and charted in Excel 2011 (Microsoft Corp): demographic characteristics of the patients, type and level of sports participation, duration of follow-up, Outerbridge grade in the lateral compartment as documented at the time of PLM, limb alignment, time from PLM to diagnosis of RC, subsequent treatment undertaken, clinical outcomes, and the cause of lateral compartment RC reported.
Collating, Summarizing, and Reporting the Results
Owing to the small number of published studies and the heterogeneity among them, no statistical analyses were performed. Instead, the findings were summarized through a narrative analysis of the published literature. The risk of bias in case series was assessed using the MINORS (Methodological Index for Non-randomized Studies) tool. 34 The level of evidence of each article was classified according to the 2011 adjusted criteria of the Oxford Centre for Evidence-Based Medicine. 18 The quality of evidence for each potential risk factor studied was assessed using the criteria of the GRADE (Grading of Recommendations Assessment, Development and Evaluation) Working Group. 15,31
Results
Application of the search strategy and eligibility criteria resulted in the inclusion of 5 articles (totaling 22 cases of RC). Figure 2 demonstrates the flow of studies. The publication dates of the studies ranged from 1998 to 2014. Three studies were case series (level 4 evidence), 8,22,35 and the remaining 2 were case reports (level 5 evidence). 2,19

Flow diagram of identification, screening, and selection of studies.
Basic Characteristics of the Studies
Table 1 presents population characteristics, including demographic data, type and level of sports participation, and limb alignment. Of the 22 total cases, 20 (91%) were male. In all studies, the mean age of patients was <30 years, but the range was 16 to 43 years. Fifteen cases (68.2%) involved professional athletes, and the other 7 (31.8%) comprised patients who participated in sports for recreational purposes or at a competitive level.
Demographics and Clinical Characteristics of Included Patients With Rapid Chondrolysis After Partial Lateral Meniscectomy a

a F, female; M, male; NA, not available.
b Hip-knee-ankle angle in parentheses.
The methodological quality of the case series (as evaluated by the MINORS tool) varied between 6 and 8, indicating a high risk of bias (Table 2). The strength of the evidence available to determine potential risk factors for RC was very low based on assessment using GRADE recommendations (Table 3).
Quality Assessment of Included Case Series Using the MINORS a
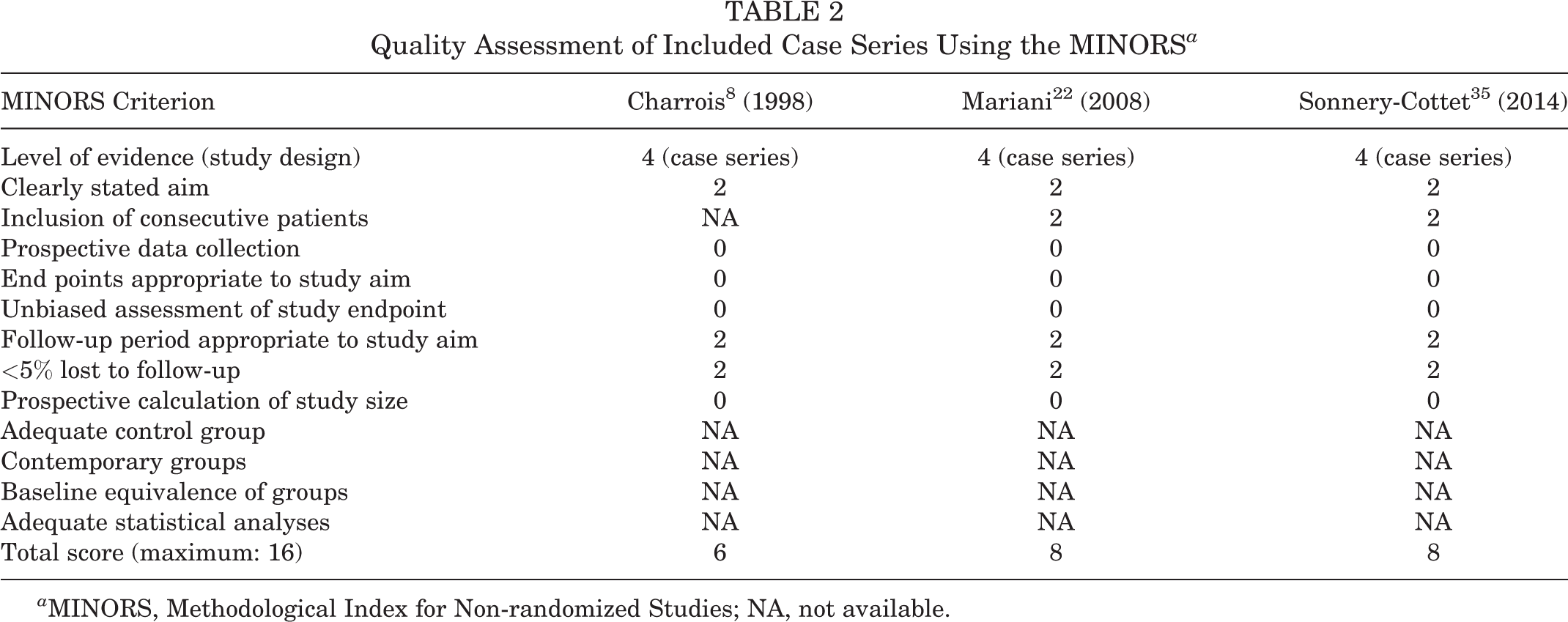
a MINORS, Methodological Index for Non-randomized Studies; NA, not available.
Quality of Evidence for All Possible Risk Factors for Rapid Chondrolysis a

a GRADE, Grading of Recommendations, Assessment, Development and Evaluation.
The main symptoms after RC were persistent pain and joint effusion, leading to decreased sports activity. Table 4 depicts the spectrum of meniscal lesions encountered, treatment undertaken, and evolution of cartilage damage experienced by the patients in the individual studies. It is potentially important that 45.5% (10/22) of patients underwent PLM for a radial tear. In the remaining patients, complex lateral meniscal tears were found in 4 cases and horizontal lesions in 2 patients, and the type of tear was not published in 6 cases. Table 5 presents details of the treatment provided and the outcomes, including return-to-sport data. All professional athletes in this scoping review (13/13) were able to return to competition at the preinjury levels of sport, including both of the bilateral cases. Of the remaining 7 patients, 2 returned to preinjury level of sport and 2 reduced their sports activity, while information about return to sport was missing for 3 patients. Sonnery-Cottet et al 35 noted that 6 of 8 professional soccer players were able to continue sports participation at the same level at a mean follow-up of 6.75 years (1 player retired because of his age, and 1 ended his career because of knee pain).
PLM Indication, Management, and Chondrolysis Onset a

a AH, anterior horn of the lateral meniscus; AL, arthroscopy lavage; Ho:YAG, holmium:yttrium-aluminum-garnet; MH, middle horn of the lateral meniscus; MRI, magnetic resonance imaging; NA, not available; PLM, partial lateral meniscectomy.
b Outerbridge classification.
c Kellgren-Lawrence classification.
Chondrolysis Management and Outcomes a

a AD, diagnostic arthroscopy; AL, arthroscopic lavage; HTO, high tibial osteotomy; NA, not available; PLM, partial lateral meniscectomy; ROM, range of motion; RTS, return to sport.
All of the authors reviewed suggested a possible causal mechanism for the development of RC. These data are presented in Table 6. In summary, there was universal agreement that mechanical overload was an important factor in the pathogenesis of RC. Mariani et al 22 stated that patients had increased rotational laxity and magnetic resonance imaging (MRI) evidence of posterolateral corner injury, however this finding was not reported by any of the other authors.
Suggested Pathophysiology of Rapid Chondrolysis After Partial Lateral Meniscectomy as Postulated by Authors of the Included Studies

Discussion
The main findings of this scoping review are that RC is a rare condition that may occur after PLM, typically within 1 year of the index procedure, and that it predominantly affects young men participating in high-intensity sports. A further important finding was that return to the preinjury level of sport is frequent. Specifically, all professional athletes in this scoping review were able to return to their preinjury levels of sport at a mean of 8 months after RC management, although never before the fourth postoperative month. Sonnery-Cottet et al 35 noted that 6 of 8 professional athletes in their series were still competing at the same level at a mean follow-up of 81.6 months, despite grade 3-4 Kellgren-Lawrence changes in the lateral compartment. However, return to sport was not universal in recreational athletes.
An additional important finding was that all of the authors postulated that the pathophysiological process for RC has a mechanical basis and that excessive focal cartilage loading is the trigger. 2,19,22,35,37 It is well recognized that meniscal resection negatively affects the stress distribution and load transmission within the knee. However, it is of particular relevance in the lateral compartment because the lateral femoral condyle and lateral tibial plateau are convex and rely considerably on the presence of the meniscus for joint congruity. As a result, the meniscus bears 70% of the load transmitted through the lateral compartment of the knee. In comparison, in the medial compartment, only 50% of the load is borne by the meniscus 32 because the convex femoral condyle articulates with the relatively congruous and concave tibial plateau. Consequently, the lateral compartment is more vulnerable than the medial compartment to degenerative changes after partial meniscectomy or meniscal tear and thus tends to deteriorate much faster. 5 Murakami et al 25 also reported in a 2018 MRI study with T2 mapping that resection of any lateral meniscal segment may cause early cartilage degeneration. These observations could also explain why outcomes of PLM are inferior 1,12,16,17,26 and why early return to sports after PLM in professional or competitive athletes is notably more challenging when compared with partial medial meniscectomy.
Specifically, Nawabi et al 26 cited a higher risk of adverse symptoms during the early recovery phase after PLM as compared with patients undergoing medial meniscectomy. Among 42 elite athletes who had undergone PLM, 69% experienced chronic effusion and/or persistent joint-line pain. 26 In the same study, the relative rate of return to preinjury levels was 6 times greater after medial meniscectomy than PLM. These findings were supported by Aune et al, 4 who indicated that 38% of National Football League athletes were unable to return to play at their previous levels after partial and isolated lateral meniscectomy; however, there was no mention of RC. In a retrospective case-control study, 6 the Tegner activity scores of 31 competitive athletes were evaluated before and after isolated PLM. The authors cited a decrease from a mean score of 7.2 (competitive sports) to 5.7 (recreational sports) at a mean follow-up of 8 years. 6 Additionally, Ford et al 14 suggested that concern is warranted in returning athletes to sport activities after PLM of an isolated radial tear attributed to isokinetic torque deficits. The authors postulated that athletes who returned to sport 3 months after PLM may employ compensation strategies with landing as compared with the uninjured limb, which could lead to poor outcomes.
Regardless of the compartment, a meniscal tear or partial meniscectomy alters the geometry and shape of the meniscus and reduces its functional capacity. The severity of the deficit is dependent on the tear morphology, with some tear patterns, such as radial tears extending to the periphery and root tears, being equivalent to a total meniscectomy in terms of the resultant increase in joint contact forces. 23,28 Based on this concept, it is perhaps unsurprising that half of the study population had a radial tear at the time of PLM. Although the study population was too small to make firm conclusions in this regard, it is likely that tear patterns with the most severe biomechanical consequences confer an increased risk of RC because of the potential for significant cartilage overload. However, it is important to note that RC has occurred even after a limited PLM, as demonstrated from our patient in Figure 1.
Once the cartilage is overloaded, chondrocyte death and cartilage matrix damage may occur. 11 The injured cartilage releases debris into the synovial fluid, which is phagocytosed by synovial macrophages, amplifying the synovitis. In response, synovial cells produce catabolic and proinflammatory mediators (cytokines, collagenases) that boost the production of proteolytic enzymes responsible for cartilage breakdown, creating a positive feedback loop 33 that may ultimately lead to RC.
Although a common denominator identified in this review was that the authors of all studies postulated that the pathophysiology of RC was based on mechanical overload, Mariani et al 22 suggested that posterolateral corner laxity may be important in the development of RC after PLM. The authors identified rotational laxity (positive dial test at 30° of knee flexion) and MRI evidence of posterolateral corner injury (lax fibular collateral ligament and increased signal at the popliteus musculotendinous junction) in 5 professional soccer players with RC after a PLM. They proposed that rotational laxity could increase the shear stresses in the articular cartilage during high-performance sport activities, and they performed arthroscopic lavage with open retensioning of the posterior meniscofemoral capsule in all patients to address laxity. 22 In contrast to Mariani et al, other authors reported no evidence of ligamentous/capsular injury or rotational laxity on physical examination or MRI evaluation in patients with RC. 35,37 In summary, it appears that there is consensus that mechanical overload is the primary causal factor, but it is important to carefully assess the posterolateral corner in any patient presenting with RC.
The main limitation of this scoping review was that published reports of RC are rare; therefore, there was limited available evidence overall. Furthermore, it may be the case that the condition is underrecognized (owing to a lack of previous publications on this topic), and as such, a reliable estimate of the true incidence after PLM cannot be determined. Additionally, all articles had small study populations, were retrospective, and had a high risk of bias. The duration of follow-up was also limited, so it was not possible to establish whether RC predisposes to a requirement for arthroplasty surgery at a young age. Although a range of treatment options was reported, there was insufficient evidence to determine the role of each, and no firm recommendations can be made. Furthermore, the overall strength of the evidence as assessed using the GRADE tool was very low. Despite these limitations, the review provides useful information for counseling patients before PLM, highlights patients potentially at risk, and guides realistic expectations of outcomes of treatment for RC.
Conclusion
RC after PLM is a rare condition that typically occurs within 12 months of the index procedure. Younger age, male sex, high-intensity sports participation, and some meniscal tear patterns (eg, radial tear) are potentially important risk factors. Return-to-sport rates at short-term follow-up are high, but no long-term studies were identified. All authors of the included studies postulated that the pathogenesis of RC relates to mechanical focal cartilage overload.
Footnotes
Final revision submitted July 8, 2020; accepted August 27, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: B.S.-C. is a paid consultant for and receives royalties and research support from Arthrex. M.T. is a paid consultant for Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.