
Abstract
Background:
Lateral meniscal tears are often seen with acute anterior cruciate ligament (ACL) injury and may be left in situ, repaired, or treated with meniscectomy. Clinical studies have shown good outcomes with vertical tears left in situ and poor outcomes following meniscectomy. However, clinically relevant studies are needed to establish a biomechanical foundation for treatment of these tears, particularly regarding the effects of meniscectomy.
Purpose:
To compare tibiofemoral joint mechanics following vertical lateral meniscal tears and meniscectomies. We hypothesized that a peripheral vertical tear of the lateral meniscus would alter joint mechanics, increasing contact pressure and area, and that more drastic effects would be seen following meniscectomy, at higher knee flexion angles, and with increased loads.
Study Design:
Controlled laboratory study.
Methods:
Ten fresh-frozen cadaveric knees (average age, 55 ± 12 years) were tested with 5 lateral meniscus states: intact, short vertical tear, extended vertical tear, posterior horn partial meniscectomy (rim intact), and posterior horn subtotal meniscectomy (rim excised). The specimens were loaded axially at knee flexion angles of 0°, 30°, and 60°, and musculotendinous forces were applied, simulating a 2-legged squat. Intra-articular contact pressures were measured using pressure-sensitive Fuji film. Kinematic data were acquired through digitization of fiducial markers.
Results:
Vertical tears did not cause a significant change in contact pressure or area. Partial meniscectomy increased maximum contact pressures in the lateral compartment at 30° and 60° from 5.3 MPa to 7.2 MPa and 7.6 MPa, respectively (P = .02, P = .007). Subtotal meniscectomy (8.4 MPa) significantly increased contact pressure compared with partial meniscectomy (7.6 MPa) at 60° (P = .04). Both meniscectomy states significantly increased contact pressures with increasing flexion from 0° to 60° (P < .001, P < .001).
Conclusion:
Vertical tears of the lateral meniscus during a simulated 2-legged squat did not significantly change contact pressures and areas compared with an intact meniscus. However, treating these tears with partial and complete meniscectomy significantly increased maximum contact pressures.
Clinical Relevance:
Biomechanical evidence supports treating vertical lateral meniscus tears with meniscal-sparing techniques as opposed to meniscectomy, which may lead to progressive degenerative joint disease from altered joint biomechanics.
The meniscus is a critical component of a healthy, functional knee and plays a role in load bearing, load distribution, shock absorption, and joint stabilization. 20,26,29,41 Tears or other injuries to the menisci are common and tend to disturb the circumferential fiber arrangement, disrupting hoop stresses and altering joint congruency. 5,19,33 Approximately two thirds of anterior cruciate ligament (ACL) injuries have been associated with a lateral meniscal tear, frequently peripheral vertical tears of the posterior horn. 7,12,34,40 Unstable tears are typically treated at the time of ACL reconstruction with either partial meniscectomy or primary repair. The treatment algorithm for relatively stable tears, however, is not as clear. Fitzgibbons and Shelbourne, 16 for example, contend that vertical longitudinal tears posterior to the popliteal hiatus do not need to be repaired in conjunction with ACL reconstruction, as they do not become unstable over time. 39
Current treatment strategies for meniscus injury include leaving them in situ, meniscal repair, and partial or total meniscectomy. Meniscectomy remains the most commonly performed surgical procedure by orthopaedic surgeons in the United States. 1 Partial lateral meniscectomy is often performed in conjunction with acute ACL reconstructions despite some studies showing 200% to 300% increases in contact stresses after meniscectomy. 14,15,20,37 Additionally, rapid chondrolysis is a rare complication that has only been reported following partial lateral meniscectomy, 3,21,28 suggesting increased vulnerability of the lateral compartment to degeneration following meniscal injury.
The existing literature indicates that lateral meniscus injury and meniscectomy portend poorer outcomes when compared with medial meniscal injuries, but few clinically relevant studies exist that specifically examine the biomechanics of peripheral vertical tears of the lateral meniscus. We elected in this study to focus on vertical tears of the posterior horn, which are commonly seen acutely with ACL injury. The purpose of this study was to characterize changes in in vitro tibiofemoral joint contact at different points in the arc of motion simulating a 2-legged squat following lateral meniscal tears and meniscectomy in an ACL intact knee. We hypothesized the following: (1) peripheral vertical tears of the posterior horn of the lateral meniscus would significantly alter joint contact mechanics and kinematics and (2) meniscectomy of the peripheral vertical tear would significantly alter joint contact and kinematics in comparison with the tear states.
Materials and Methods
Specimens and Preparation
Ten fresh-frozen cadaveric knees were stored at −20°C and thawed at room temperature overnight prior to dissection. The average age of the cadaveric knee specimens was 55 ± 12 years; 4 were male and 6 were female. They were examined externally and arthroscopically to ensure the absence of joint contracture, ligamentous or meniscal injuries, or other indicators of degenerative joint disease. At most, they had Outerbridge grade 1 osteoarthritic changes. Although the skin and subcutaneous tissues were removed, the capsular and ligamentous structures in and around the knee joint, including the cruciate and collateral ligaments, the popliteus muscle and tendon, and the oblique popliteal ligament, were kept intact. Three to 5 cm of the distal tendinous insertions of the semimembranosus medially and the biceps femoris laterally were preserved. Approximately 5 cm of the quadriceps tendon superior to the patella was preserved. Braided sutures were sutured to each of these tendons in a Krackow fashion for later attachment to a weight-pulley system. The femur and tibia were potted in 60 mm–inner diameter polyvinyl chloride cylinders using epoxy compound to be held by a custom fixture during biomechanical testing.
Creation of Meniscal States
Five lateral meniscus states were evaluated: (1) intact; (2) <1.5 cm peripheral vertical tear medial to popliteal hiatus (hereafter referred to as short vertical tear); (3) 1.5 to 3 cm peripheral vertical tear lateral to hiatus (extended vertical tear); (4) posterior horn partial meniscectomy, rim intact; and (5) posterior horn subtotal meniscectomy, rim excised (Figure 1). The tear states were created via combined open and arthroscopic minimally invasive approaches. Standard anterolateral (AL) and anteromedial (AM) portals were first established at the inferior poles of the patella (as practiced by the senior surgeon). Three accessory portals were then established to facilitate creation of tears: a lateral portal 2 cm lateral to the standard AL portal, a far lateral/proximal portal 4 cm lateral and 1 cm proximal to the standard AL portal, and a far lateral portal 5 cm lateral to the standard AL portal. Using a No. 11 blade, a peripheral vertical tear medial to the popliteal hiatus was created (short vertical tear state). This tear was then extended lateral to, and including, the popliteal hiatus (extended vertical tear state). A partial meniscectomy state was created with the removal of the torn meniscus, leaving the peripheral rim intact. Finally, a subtotal meniscectomy was performed by removing the peripheral rim.
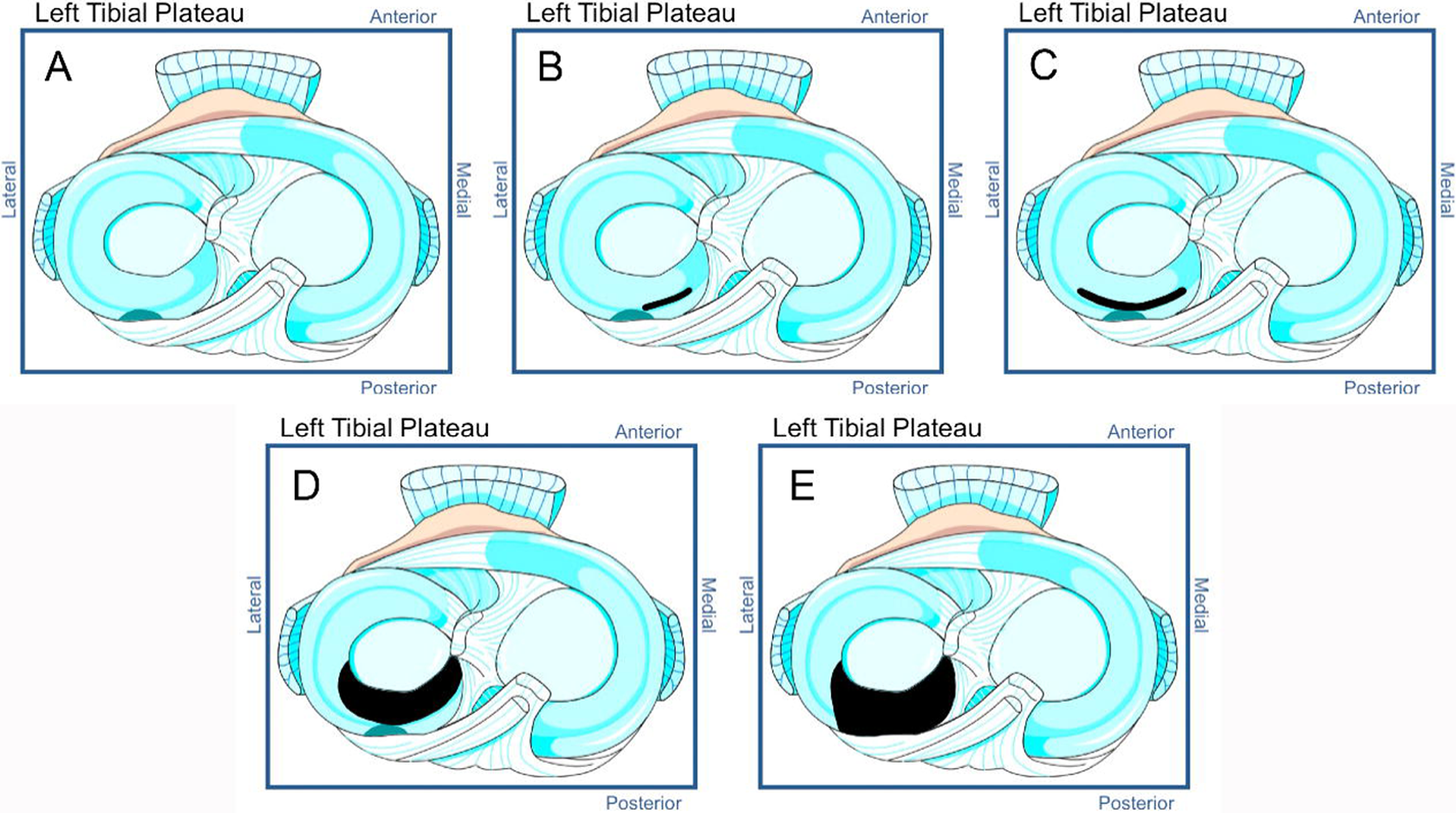
The 5 lateral meniscal states. (A) Intact; (B) short vertical tear (to the edge of the popliteal hiatus); (C) extended vertical tear; (D) posterior horn partial meniscectomy (peripheral rim is intact); (E) posterior horn subtotal meniscectomy (peripheral rim is gone).
Biomechanical Testing
Figure 2 summarizes our testing protocol. The specimens underwent biomechanical testing on a materials testing machine (Instron Model 8874; Instron Corp) after each of the 5 meniscal states was created. The testing configuration simulated a single lower extremity during a 2-legged squat by a person of approximately 70 kg body weight. Three knee flexion angles were included: 0°, 30°, and 60°. The femur was constrained in all 6 degrees of freedom. The distal end of the tibia was constrained in anterior-posterior and superior-inferior translations but allowed medial-lateral translation, abduction-adduction, flexion-extension, and internal-external rotation. Fuji film (Fujifilm Corp) in the shape of the tibial plateau was inserted through the anterior arthrotomies underneath both menisci using a technique previously described. 4,31 Simulated muscle forces were applied by pulling the quadriceps and hamstring along the shaft of the femur via a pulley-weight system mounted on a loading frame. We used a 2:1 ratio of quadriceps versus hamstring forces, as was done in previous studies. 8,27 The 2-legged knee squat was simulated such that a constant ground reaction force equal to half the weight of a 70-kg man, or 350 N, was maintained. To determine the quadriceps and hamstring forces needed to maintain equilibrium at each of the knee flexion angles, we applied a series of muscle loads to the cadaveric knee until 350 N was recorded by the load cell placed at the bottom of the specimen. With increasing squat, greater muscle forces are required to maintain force and moment equilibrium. We estimated, based on simple equilibrium equations and convenience of weight application, the forces that needed to be applied. The quadriceps and hamstring forces applied were determined to be, respectively: 30 and 15 lb (133 and 67 N) at 0° of flexion; 50 and 25 lb (222 and 111 N) at 30° of flexion; and 70 and 35 lb (311 and 156 N) at 60° of flexion. Thus, at 0° of knee flexion, a total of 550 N of force was applied, at 30° of flexion a total of 683 N was applied, and at 60° of flexion a total of 817 N was applied.

Flow diagram of testing protocol. The knee was mounted in a materials testing machine where an axial load and functional muscle loads were applied. Fuji film was inserted via submeniscal arthrotomies to obtain submeniscal contact pressure and area, and the fiducial markers were digitized to obtain tibiofemoral kinematics. Five knee states were studied in this manner.
Contact Pressure Measurement
The use of Fuji Prescale film in quantifying intra-articular contact pressures has been validated extensively in previous studies. 2,6,17,22,25 In this study, Super Low Prescale (0.5-2.5 MPa) and Low Prescale (2.5-10 MPa) film, corresponding to the range of values seen in previous studies, 2,10,11,17,24 was used to measure the tibiofemoral contact pressures. One centimeter AM and AL submeniscal arthrotomies were made to allow insertion of pressure-sensitive Fuji film, and posteromedial (PM) and posterolateral (PL) submeniscal arthrotomies were performed to confirm consistent placement of the Fuji film below the meniscus.
After testing, the developed film was scanned using an HP Scanjet 5550c scanner (Hewlett-Packard Development Co). The scanned images were converted into contact congruency measures via a previously developed calibration program relating the image intensity to contact pressure. 30 All image processing and analyses were performed using custom MATLAB programs (Mathworks Inc).
Kinematic Analysis
Metal screws (1/4 inch head diameter, 1 inch length, and 1/8 inch hexagonal indentation) were rigidly fixed to the femur and tibia as fiducial markers, a minimum of 3 per bone. While the specimen was in the materials testing machine, the fiducial markers on the femur and on the tibia were digitized with a Microscribe 3DX articulated digitizing robotic arm (Immersion Corp). The digitization was done before the application of any load (muscle or compressive) and approximately 30 to 60 seconds after the loads were applied with the load cell–measured axial force stabilized at 350 N. When the testing was completed, the specimen was disarticulated and the tibia and femur were digitized to associate the fiducial markers with anatomical coordinate axes. For the femur, the medial epicondyle, the lateral epicondyle, and the center of the femoral shaft proximally were digitized. For the tibia, the medial and lateral aspects of the tibial plateau and the center of the tibial shaft were digitized. With these points, anatomical axes for each bone were created, and tibiofemoral kinematics, in terms of relative positions and angles between the 2 bones, were determined according to the conventions established by Grood and Suntay. 18 Although the accuracy of the Microscribe digitizer stylus was 0.7 mm, by digitizing up to 5 fiducial markers, the calculated accuracy in determining the bone position was markedly improved to 0.3 mm and 0.3°.
Statistical Analysis
A 2-way repeated-measures analysis of variance (ANOVA) was performed to examine the effects of meniscal states and knee flexion angle on maximum contact pressure, contact area, and tibiofemoral kinematics. If P < .05, post hoc paired t tests were conducted to compare specific meniscal states. All statistical analyses were performed using SPSS (IBM Corp).
Results
Lateral Compartment Maximum Contact Pressure
Figure 3 illustrates how meniscal state affected the lateral compartment maximum contact pressure. At 0°, there were no significant differences in contact pressure or area between any of the meniscal states. However, at 30°, there were significant differences in lateral compartment maximum pressures (P = .001)—specifically between intact and meniscectomy states and between tear states and meniscectomy states. At 60° of knee flexion, maximum contact pressures changed significantly between meniscal states (P < .001), while total tibial contact area did not. Significant differences in maximum pressure were found between intact and meniscectomy states, tear states and meniscectomy states, and between partial and subtotal meniscectomy states. No significant difference in maximum contact pressures was found between intact and either short or extended vertical tear states.

Lateral compartment maximum pressures and areas: comparing meniscal states at different knee flexion angles.
Figure 4 and Table 1 illustrate the effect of knee flexion angle on lateral compartment maximum contact pressures. In the intact and short tear states, there were no differences in contact pressures with change of knee flexion angle. In the extended tear state, there was a significant increase in maximum contact pressure (P = .02) with increase in knee flexion angle, primarily at 60°. In the partial meniscectomy state, significant increases in maximum contact pressure were noted with increasing knee flexion angle (P < .001). In the subtotal meniscectomy state, significant increases in maximum contact pressure (P < .001) were observed among all degrees of knee flexion.
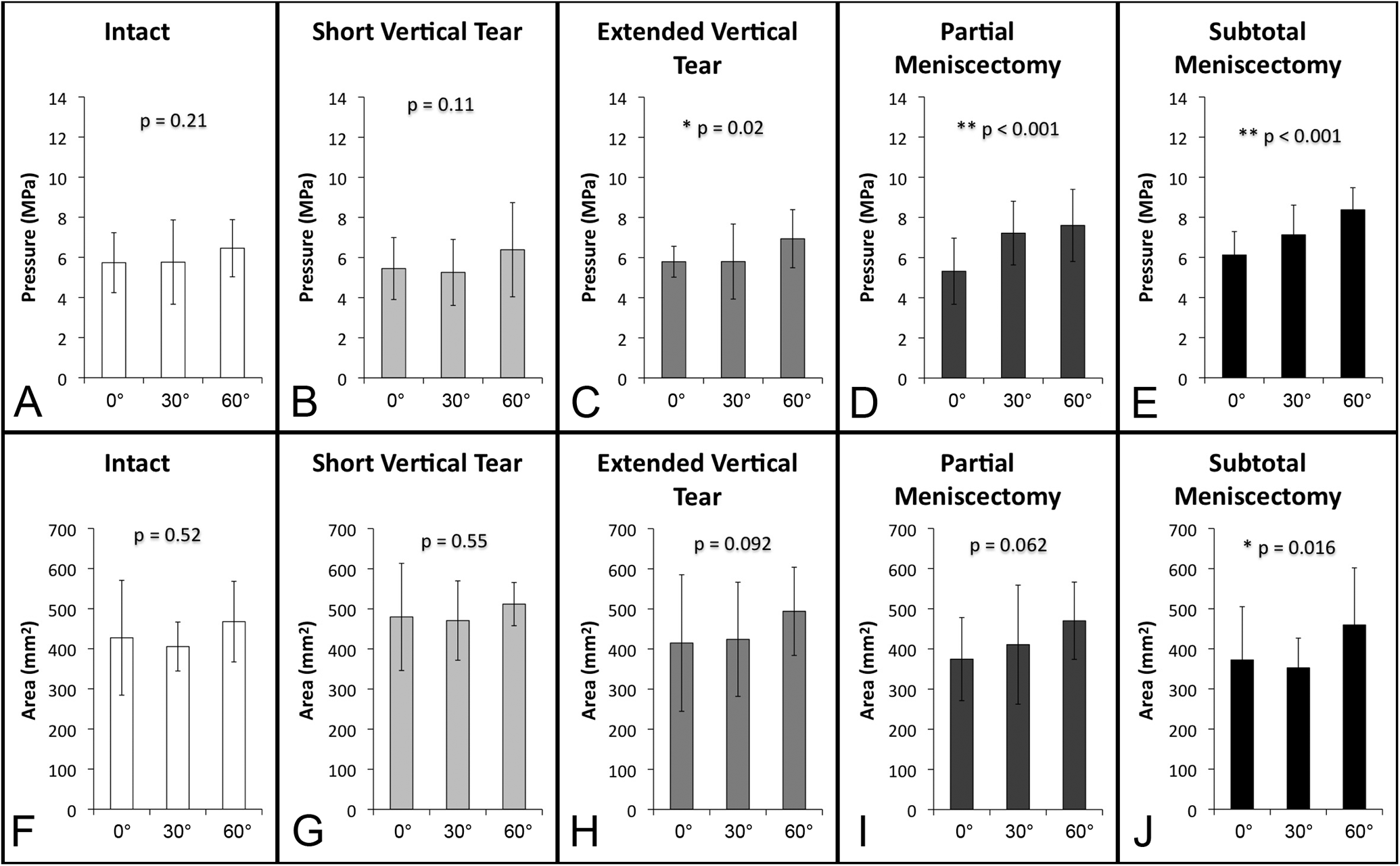
Lateral compartment maximum pressures and areas: comparing knee flexion angles for different meniscal states.
Lateral Compartment Maximum Contact Pressures and Contact Areas for All Meniscus States at All Flexion Angles a

a Values are expressed as mean ± standard deviation.
Lateral Compartment Versus Medial Compartment
In the medial compartment, there were no significant changes in the maximum contact pressures with the progression of lateral meniscal conditions. Contact pressure was not significantly different between the medial and lateral compartments in the intact state, but in the remainder of lateral meniscus states, there was significantly greater maximum contact pressure in the lateral compartment compared to the medial (Table 2).
Comparison of Maximum Contact Pressure and Tibial Contact Area at Different Lateral Meniscal States Between the Lateral and Medial Compartments a

a Data reported are with all flexion angles averaged. Values are expressed as mean ± standard deviation.
b Statistically significant at P < .05.
c Statistically significant at P < .001.
Joint Kinematics
No statistically significant differences (at α = .05 level) using repeated-measures ANOVA were found among the lateral meniscus states in any of the kinematic measurements (anterior-posterior translation, lateral-medial translation, external-internal rotation, and valgus-varus angulation) at 0°, 30°, or 60° of knee flexion (Table 3).
Tibiofemoral Kinematics During Simulated 2-Legged Knee Squat a

a Data were normalized with the intact state set to 0, and all the flexion angles were averaged. Values are expressed as mean ± standard deviation.
Discussion
Meniscal injury and meniscectomy have been associated with poorer outcomes after ACL injury and reconstruction. 9,23,44 Furthermore, lateral meniscectomy has been shown to result in more instability on pivot shift testing than medial meniscectomy in ACL-deficient knees, highlighting its importance in resisting anterior tibial translation with valgus and rotatory loads. 32 In the face of concomitant ACL and meniscal injury, every attempt should be made to salvage the meniscus. It remains unclear, however, whether an intrinsically stable tear such as a short peripheral tear of the posterior horn ought to be left in situ or debrided.
This study aimed to establish in vitro biomechanical evidence to support treatment decisions for peripheral vertical tears of the posterior horn of the lateral meniscus such as those frequently seen with ACL injury. As an initial step, we sought to understand how these tears affect tibiofemoral joint contact pressures and kinematics as compared with an intact meniscus in an ACL-stabilized knee. Specifically, we explored our hypotheses by biomechanical testing with a static functional 2-legged knee squat model at flexion angles of 0°, 30°, and 60°. Neither the short nor the extended peripheral vertical tears resulted in altered joint contact pressures or tibiofemoral kinematics at any degree of flexion compared with the intact knee. This suggests that peripheral vertical tears minimally disrupt the circumferential fiber arrangement and do not compromise the hoop stresses that are fundamental to the function of the meniscus. Meniscectomy of these peripheral vertical tears in fact results in greater contact pressures than when the tears are left in situ.
Fitzgibbons and Shelbourne 16 and Shelbourne and Heinrich 38 have reported their clinical results with peripheral vertical lateral meniscus tears treated with benign neglect or trephination. Based on their subjective and objective knee scores, they concluded that these tears were asymptomatic at short-term (average, 3.6 years) and medium-term (average, 6.6 years) follow-up 16,38 ; at medium-term follow-up, there was no lateral joint space narrowing radiographically in greater than 93% of patients. 38 At long-term (10 years) follow-up, mild joint space narrowing was appreciated though there was no significant difference in subjective or objective scores compared with the control group. Uchio et al 42 and Yagishita et al 45 further showed a 71% to 74% healing rate of short peripheral tears of the meniscus as well as minimal arthritic changes at second-look arthroscopy performed at 17 to 21 months. These clinical findings support the notion that short peripheral tears of the lateral meniscus may have minimal effects on the biomechanics of the tibiofemoral compartment.
We also hypothesized that subtotal meniscectomy would result in more drastic joint contact changes when compared with a partial meniscectomy. In the present study, the only significant difference noted between the rim-intact and rim-excised partial meniscectomy states was at 60° of flexion with maximum lateral contact pressure. This is consistent with the increased importance of the meniscal rim at higher degrees of flexion as the femoral condyles increasingly engage the posterior horn of the meniscus. While 100% to 200% increases in contact pressure have been reported following total meniscectomy, 6,36 Ode et al 35 and Dienst et al 13 reported more modest increases in contact pressures after total meniscectomy (<50%). Of note, the load used by Baratz (Fu) et al6 and Paletta et al36 was 1800 N, while Ode et al 35 and Dienst et al 13 used loads of 800 N and 1000 N, respectively. In the current study, we used loads ranging from 550 N at 0° of knee flexion to 817 N at 60° of flexion.
The stability of compartment contact pressures seen with short and extended peripheral tears may help to explain why minimal arthritic changes have been found after vertical tears. 39 As previously shown, increasing contact pressures result in a higher likelihood of development of chondrosis and arthritis. Significant increases in maximum lateral compartment contact pressure when compared with the medial compartment were seen after partial and subtotal meniscectomy, which may explain, in part, complications of menisectomy such as rapid chondrolysis and unicompartmental degenerative joint disease.
The present study also explored the effect of various lateral meniscus states on knee kinematics, which few studies have done. Those were limited to tibial subluxation in the anterior-posterior direction 26,41 and primarily showed alteration in kinematics with medial meniscus deficiencies. In the present study, no significant differences in anterior-posterior translation, lateral-medial translation, external-internal rotation, or varus-valgus angulation were found with changes in lateral meniscus state. This result would be expected based on the lateral meniscus having a smaller role in joint stabilization than the medial meniscus due to its less developed capsular attachments and the presence of the popliteal hiatus. 43
The primary limitation of the present study, as with any cadaveric in vitro study, is the clinical applicability. The tears represent 2 types of tears frequently encountered in clinical practice, especially in association with acute ACL tears. We were only able to estimate in vivo mechanical conditions, and, due to time/funding limitations, only a single activity was chosen. We modeled a 2-legged knee squat—a relatively simple and static activity with few forces and of low magnitude. We were not able to re-create forces that would be created by cutting- or pivoting-type movements. Effects or differences identified in our study are likely to be more substantial during more dynamic, higher flexion, and greater torque–associated activities. Therefore, the results obtained from this controlled laboratory study are specific to our in vitro testing conditions, and generalization must be cautioned.
Further, the present study did not address the likelihood of these tears propagating and leading to meniscal displacement. The meniscus functions in a dynamic environment and would respond to tears in a dynamic way. The current study utilized a static loading model designed to measure primarily joint contact changes. It was not designed to test the dynamic or time-dependent responses of meniscal tears. Cyclic or impact loading may be better suited for testing those aspects of meniscal tears.
In summary, the results of this study indicate that neither short nor extended peripheral vertical tears of the lateral meniscus significantly affect contact pressures of either compartment or tibiofemoral kinematics with loading of the knee during a simulated 2-legged knee squat. Meniscectomy, however, increases joint contact pressures with amplified effects at higher degrees of knee flexion and with excision of the meniscal rim. Meniscal preservation should be the goal when considering treatment options. Potentially unstable tears with tissue loss should be repaired to avoid the possibility of propagation that would necessitate meniscectomy.
Footnotes
One or more of the authors has declared the following potential conflicts of interest or source of funding: The Pittsburgh Foundation funded this study through a Ferguson Grant Award.