
Abstract
Background:
Ever since orthopaedic surgery was cited as the specialty with the lowest percentage of women, research has geared toward better understanding where lapses occur and ensured that equitable opportunities exist within the field.
Purpose/Hypothesis:
To analyze the 5-year trend in the academic leadership roles of female versus male orthopaedic surgeons at the AOSSM Annual Meeting. We hypothesized that a nationally representative proportion of female surgeons would hold academic leadership positions and that this figure would increase during the study period.
Study Design:
Cross-sectional study.
Methods:
Publicly available AOSSM Annual Meeting brochures from 2015 to 2019 were analyzed. Moderators and course instructors with doctor of medicine (MD) or doctor of osteopathic medicine (DO) degrees were included. Gender-neutral names were researched as needed for gender clarification. The gender composition of total moderators and total course instructors was calculated and trended over the 5-year period. Statistics from the Association of American Medical Colleges (AAMC) in 2017, the median of the study period, were used for comparison with total active sports medicine orthopaedic surgeons.
Results:
Women represented 5.9% of moderators and course instructors at the AOSSM Annual Meeting from 2015 to 2019. The percentage of female moderators increased from 6.0% in 2015 to 8.6% in 2019, and the percentage of female course instructors increased from 3.4% in 2015 to 5.6% in 2019. After adjusting for dual contributions by a single woman to both roles, we found that 6.7% of total moderators and course instructors over the 5-year study period were women (6.3% in 2015, 7.7% in 2019). This was close to the 6.6% rate of female sports orthopaedic surgeons reported by the AAMC in 2017.
Conclusion:
Using moderator and instructor involvement at the AAOSM Annual Meetings as a proxy for involvement in academia, we found evidence to support gender parity in the orthopaedic subspecialty of sports medicine. This example of a culture of equity and inclusion may be an encouraging example to cite in recruitment efforts for prospective medical student applicants and endorsing current female surgeons to seek leadership roles in academia.
Introduction
In 2016, approximately 50% of the US medical school matriculates were women, and there were more female than male first-time applicants. 3 Moreover, women accounted for 52% of matriculants in 2019. 3 Yet, the representation of women in orthopaedic surgery has not kept pace with the steady and progressive representation of women in the nation’s medical schools. 5,10 Approximately 11% of orthopaedic surgery residents were women in the 2005 to 2006 academic year, which increased to 14% by 2017. In the 2016 to 2017 academic year, orthopaedic surgery remained the specialty with the lowest proportion of female residents. 7 Although percentages appear to be slowly improving, orthopaedic surgery continues to lack gender diversity, especially in comparison with other surgical fields such as general surgery, neurological surgery, and most notably cardiothoracic surgery, which has seen a 110% increase over the same period. 7,9
This lack of diversity has motivated investigations and subsequent innovative solutions to resolve the barriers to gender equality in orthopaedic surgery. These investigations revealed that there are several misconceptions that discourage women from entering the field, including that a work-life balance is impossible, too much physical strength is required, and the field deals mainly with sports-related injuries. Additionally, a lack of strong mentorship on the path to residency has been cited in the literature. 15 Same-gender mentorship opportunities for women are limited because of the low percentage of female residents and attending orthopaedic surgeons. 13 In the 2015 to 2016 academic year, 8.7% of US medical school orthopaedic surgery professors were women and only 1 orthopaedic surgery department chair was a woman, the lowest number of female full-time faculty of all specialties. 7
With some of the barriers better understood, targeted efforts have focused on increasing the recruitment of women into orthopaedic surgery via the dispelling of misconceptions of the specialty and the fostering of positive perceptions of science, technology, engineering, and mathematics careers as early as college. Medical schools with required coursework in musculoskeletal medicine and early exposure to orthopaedic principles have consistently been shown to increase the number of female students pursuing orthopaedic surgery. 4,9,12,13 Additional efforts have aimed to promote mentorship in medical school. Collectively, organizations and advocates of these initiatives summarize this longitudinal mission as “building the pipeline.” 13 One critical feature of building the pipeline is ensuring that opportunities in orthopaedic surgery are available to all those who desire them, regardless of gender. Given that many of the cited deterrents for women entering the field of orthopaedic surgery can be dispelled in the recruitment phase, it is our duty to ensure that these misconceptions are, in fact, misconceptions and that equitable opportunities are available to both men and women in the field of orthopaedic surgery.
A recent study 16 indicated that women in orthopaedic surgery are represented in academia proportionally to their representation in the field, specifically in terms of editorship and authorship in major orthopaedic journals. In sports medicine, female authorship increased nearly 7-fold from 2.6% in 1972 to 14.7% in 2018. 11 Given that the orthopaedic subspecialty of sports medicine is currently among the top 3 most common subspecialties chosen by women, especially among younger surgeons, 6 we believe there is great utility in extending the aforementioned investigation into sports medicine. Therefore, to further analyze the representation of women in academic sports medicine, our goal was to (1) quantify the contributions of female orthopaedic surgeons at the AOSSM Annual Meeting and (2) determine if representation of female orthopaedic surgeons at the conference reflects changes in the field in light of new efforts to recruit women to orthopaedic surgery. We hypothesized that a nationally representative proportion of female surgeons would hold academic leadership positions and that this figure would increase during the study period.
Methods
Archived AOSSM Annual Meeting program brochures over a 5-year period from 2015 to 2019 were evaluated. The proportion of male and female moderators and course instructors was calculated to assess the representation of women at each meeting. Moderators were obtained from the Conference Agenda section, and course instructors were obtained from the Instructional Course section of the brochure. Only moderators and course instructors with doctor of medicine (MD) or doctor of osteopathic medicine (DO) degrees were included. Some individual surgeons were counted multiple times depending on how many moderator and/or course instructor roles each served in. When there was an orthopaedic surgeon with a gender-neutral name, the surgeon was researched for clarification. Percentages of male and female surgeons were then derived from the totals. We repeated our analysis, but this time, surgeons who had multiple moderator roles and/or participated in instructional courses were counted only once. This enabled us to provide a more accurate estimate of how many individual women participated at each conference.
Reported outcomes included annual percentage of female moderators, female instructional course instructors, and total female contributors to the meeting (with multiple contributions as moderators and/or course instructors counting only once) for each year during the study period. Percentages were trended over time from 2015 to 2019 and compared with the number of active sports medicine orthopaedic surgery physicians and fellows according to the Association of American Medical Colleges (AAMC). 1,2 However, because the AAMC-reported percentages were published for only 2017, the means of the reported outcomes were used for comparison.
Results
In the 5 AOSSM Annual Meetings from 2015 to 2019, women represented 5.9% (52 of 887) of the total moderators and course instructors. Specifically, 7.2% (21 of 292) of total moderators and 5.2% (31 of 595) of total course instructors were women. After accounting for multiple moderator and course instructor positions held by a single individual, female representation increased, with 6.7% (44 of 653) female contributors (Table 1).
Moderators and/or Course Instructors at the AOSSM Annual Meeting by Gender, 2015 to 2019
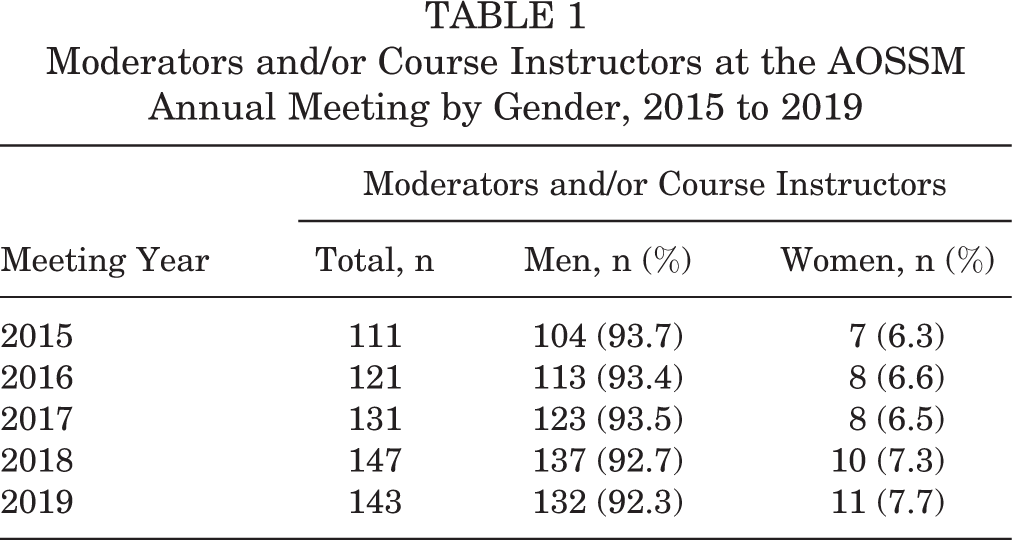
The total female moderator percentage increased from 6.0% in 2015 to 8.6% in 2019, peaking at 8.8% in 2018. The total female course instructor contribution increased from 3.4% in 2015 to 5.6% in 2019, also peaking at 6.9% in 2018. The combined percentage, after controlling for multiple contributions, increased from 6.3% in 2015 to 7.7% in 2019 (Table 1) (Figure 1).
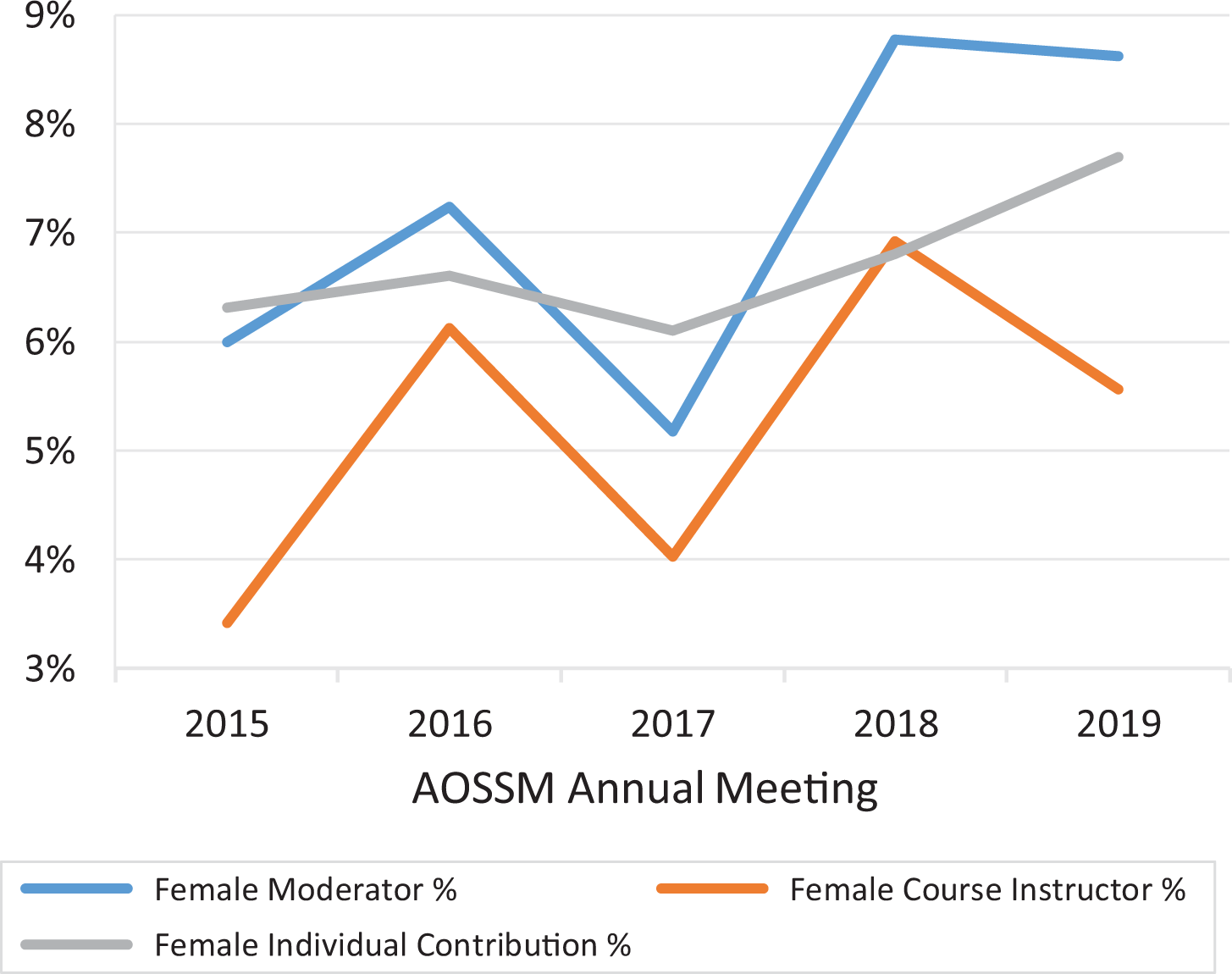
Female moderator, course instructor, and individual contribution percentages at the AOSSM Annual Meeting from 2015 to 2019.
According to the AAMC, in 2017, 6.6% and 12.1% of active sports medicine orthopaedic surgery physicians and fellows, respectively, were women. 1,2 The representation of women at the AOSSM Annual Meetings was 6.7% during the study period, after accounting for multiple contributions by an individual. This value is representative of the AAMC percentage of sports medicine orthopaedic surgeons in 2017 but less than the percentage of fellows. The representation of women at AOSSM meetings increased to 7.7% in 2019, which was still lower than the AAMC-reported percentage of female sports medicine orthopaedic surgery fellows.
Discussion
The findings of the current study demonstrated that the AOSSM Annual Meetings have a nationally representative proportion of female orthopaedic surgeons in academic and research roles, which increased during the 5 years of the study period. In addition, we found that, overall, 6.7% of the moderators and course instructors at the AOSSM meetings were women (6.3% in 2015, 7.7% in 2019). This was close to the 6.6% rate of female sports orthopaedic surgeons reported by the AAMC in 2017.
Interestingly, the percentage of female sports orthopaedic surgeons according to the AAMC (6.6%) was greater than the percentage of total female orthopaedic surgeons from all subspecialties (5.3%), supporting its popularity among female surgeons. 1 Over the 5-year study period, 5.9% of leadership roles were represented by women. However, 6.7% of individual AOSSM contributors were women. In other words, 44 different women accounted for the 52 instances in which female surgeons appeared in a leadership position over the study period. We believe 6.7% to be the most accurate snapshot of the 5-year study period, because it controls for multiple contributions by a single surgeon. Therefore, it best depicts how many individual women comprised meeting contributions. This percentage is nearly equivalent to the 2017 midstudy period 6.6% composition of active female sports orthopaedic surgeons reported by the AAMC. Additionally, both of these numbers are half that of the female resident composition reported by the AAMC. Based on this comparison, it appears that women have been proportionally represented at the AOSSM meeting in the past 5 years. Moreover, we expect this number to rise based on the 12.1% female orthopaedic surgeons on track to complete an orthopaedic sports medicine fellowship.
This study is important for several reasons. One, a recent survey of both male and female graduating orthopaedic surgery residents indicates that they have similar leadership and research aspirations. 8 Therefore, one would expect representation of both genders in such roles to be proportional to overall representation in the field. Interestingly, a recent study 14 indicated that male orthopaedic surgeons represent a significantly greater proportion of team physicians in most National Collegiate Athletic Association Division I conferences and professional sports. Two, in an effort to recruit more prospective female applicants to the field of orthopaedic surgery, it is important for mentors to have tangible examples of gender parity in the field. Three, as we continue to support initiatives to increase female recruitment, it is important we measure their success through longitudinal analyses. Although the current study utilized a mean percentage over a 5-year period to compare to a single-year AAMC statistic, we anticipate that our individual data points can be used in future trend analyses once more AAMC data points become available for comparison. In fact, we encourage such an extension of our investigation, as the nonlinear growth pattern in our data set prevented calculation of a yearly growth rate.
The study has several limitations. Although limiting moderators and course instructors to those with MD and DO degrees ensures the counting of only physicians, we cannot ensure that all of them were orthopaedic surgeons or orthopaedic surgery residents or fellows. The massive sample size of total meeting contributors over a 5-year period precluded us from such an analysis. These meetings are oftentimes attended by other physicians of other specialties who have specific interests in the field of orthopaedics, such as musculoskeletal radiologists and pathologists. However, we searched every 10th contributor at the meeting, all of whom were orthopaedic surgeons. Additionally, this study excludes surgeons from international countries with degrees other than MD or DO, such as bachelor of medicine, bachelor of surgery, Fellow of the Royal Australasian College of Surgeons, or Fellow of the Royal College of Surgeons. Last, our 5-year period was shorter than initially planned. Although the first AOSSM Annual Meeting was in 1973, publicly available online records are available from only 2015 to present. Subsequently, because the path from medical school graduation to the orthopaedic sports medicine specialty is 6 years in length, there is a time lag for recruitment efforts. In other words, our results are an indication of diversity initiatives that were put into motion ≥6 years ago. Since most diversity initiatives are still fairly new or in their infancies, we do not believe this to be a great limitation. Moreover, we encourage a follow-up study to quantify the success of diversity initiatives at work within the past 6 years, which will be reflected in the composition of future AAOSM meetings.
Conclusion
Our data suggest that the representation of female orthopaedic surgeons at the AOSSM Annual Meeting has kept pace with the percentage of current female orthopaedic sports medicine surgeons. This is important, and it supports that leadership positions at AOSSM are equitably available to all orthopaedic sports surgeons. There is, however, an overall limited female presence at the 5 most recent AOSSM meetings, which underscores the importance of continuing to recruit prospective women into orthopaedic surgery. Again, we highlight the need for an extension of the current study to not only evaluate more recent recruitment efforts but also to compare them with the next set of available AAMC statistics on the gender breakdown of orthopaedic sports medicine surgeons. As the orthopaedic workforce continues to diversify among its subspecialties, we will foster diversity in thought, approaches, perspective, and background, which enables future surgeons to care for a diverse patient population.
Footnotes
Final revision submitted July 17, 2020; accepted September, 14, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: B.G. has received education payments and nonconsulting fees from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.