
Abstract
Background:
The role of team physician (TP) in professional sports is a highly coveted position within sports medicine. There is currently limited research on the demographic characteristics of TPs within the National Football League (NFL).
Purpose:
To identify demographic characteristics and educational backgrounds of NFL head TPs (HTPs) and assistant TPs (ATPs).
Study Design:
Cross-sectional study.
Methods:
A list of TPs was identified through the National Football League Physicians Society (NFLPS). Variables investigated include age, gender, race, medical specialty, location and year of residency and fellowship training, leadership among medical societies and editorial boards, academic rank, and personal Scopus Hirsch index (h-index). Linear regression was performed to determine correlation, and t tests were used to assess differences in the h-index.
Results:
Of the 170 TPs, 21.2% were HTPs and 78.8% were ATPs. TPs were 97.6% male, 91.2% were non-Hispanic White, and 60% had attained an academic rank. The mean ages of the HTPs and ATPs were a 56.2 ± 9.6 and 52.6 ± 9.6 years, respectively (P = .047). Among orthopaedic surgeons, the most common subspecialties were sports medicine (70.5%), foot and ankle (7.6%), and spine (5.7%). Of the TPs, 48.2% and 32.9% worked for a team in the same state in which they graduated residency and fellowship, respectively. HTPs and ATPs had been in the NFLPS for a mean of 16.9 ± 10.8 and 8.8 ± 8.3 years, respectively (P < .001). Further, TPs holding an academic rank had a mean h-index of 14.0 ± 19.3, while those without an academic rank had a mean h-index of 6.2 ± 8.8 (P < .01). HTPs and ATPs had mean h-indices of 15.7 ± 15.9 and 9.6 ± 16.3 (P = .0503), respectively.
Conclusion:
TPs in the NFL are typically White men in their mid-50s who have trained at specific high-ranking institutions and obtained a fellowship in sports medicine. HTPs were likely to be older with longer tenures within the NFLPS and with more impactful research than their ATP counterparts.
The field of medicine offers physicians a multitude of leadership opportunities in the realms of education, business, research, media, and more. Among these many career possibilities, the position of team physician (TP) uniquely merges medical expertise with the world of sports and is considered a highly coveted achievement in sports medicine. TPs are especially critical in the sport of American football, a game in which players are frequently injured and TPs must intervene at any given moment to care for an injured athlete. The National Football League (NFL), the premier professional football league in the United States, features 32 distinct teams, each with its own set of TPs. Within these medical teams, 1 or 2 head TPs (HTPs) lead the management and provision of care to athletes with the support of multiple assistant TPs (ATPs).
The National Football League Physicians Society (NFLPS) is an organization governing all TPs in the league. Founded in 1966 with the goal of ensuring that all players have access to the best medical treatment, the society promoted communication across teams with the purpose of keeping track of traded players’ medical records. Since then, the group has been instrumental in developing standardized physical examinations during the drafting process, improving rules and protocols to safeguard the health of athletes, and promoting communication between medical professionals and NFL team owners. To achieve these objectives, the NFLPS designates a variable number of TPs per team as “voting members” who influence policy and guidelines. Recent policy changes that increased player safety include providing electronic tablets to facilitate efficient diagnosis of concussions and positioning a certified athlete trainer high above the field to help locate injured players in need of medical assistance. 31
Duties of a TP go far beyond managing injuries on the field as they occur. TPs coordinate preparticipation screening and evaluation, manage rehabilitation and return-to-play after injury, and consult medical experts from other fields when necessary. They also establish a medical chain of command, develop plans for medical emergencies, and train staff to operate efficiently if a crisis occurs. Furthermore, they must interface with administrators, coaches, and parents to communicate the health status of players while also maintaining patient confidentiality. 14,15
In the NFL, TPs are often fellowship-trained experts in treating life-altering injuries and are selected by individual NFL front offices. 12 In professional leagues outside the NFL, medical institutions may enter contracts with professional sports team in order to advertise their doctors as TPs. However, since 2004, the NFL has prohibited teams from entering marketing contracts that require the team to use TPs from a specific medical group. 9 While this rule was well intentioned, it has not prevented some teams from accepting sponsorship money from health care providers who employ TPs. 19
The lack of minority representation in orthopaedic surgery has been extensively discussed over the past decade. 10,18 Previous groups have conducted cross-sectional studies describing traits among various leadership roles within orthopaedic fellowships and have all demonstrated the lack of ethnic diversity among these positions. 7,11,25,26 Recently, Wiggins et al 32 evaluated diversity in terms of race and sex in 5 major US professional sports leagues, including the NFL, and concluded there is low minority and female representation among HTPs across professional sports. Otherwise, there has been limited evaluation of the characteristics of those who achieve the role of TP in professional football.
This study aimed to not only establish trends in how physicians attain the role of TPs but also uncover potential institutional barriers that may inhibit underrepresented minorities (URMs) to pursue leadership positions in the field of sports medicine, especially in the NFL. We hypothesized that NFL TPs would have decades of experience within sports medicine, would have trained at elite institutions, and would prove to be highly productive researchers. We also hypothesized that demographic characteristics of TPs would demonstrate a lack of gender and racial diversity that mirrors disparities in representation of minorities across the field of sports medicine as a whole.
Methods
In April 2021, we obtained from the NFLPS website 30 a list of TPs, including their title, voting status, the year they joined the NFLPS, and team affiliation. The demographic and educational background data were obtained for each TP through evaluation of publicly available and up-to-date curriculum vitae (CV). Any information that was unable to be gathered through CV review was found through institutional biographies as well as websites such as Doximity, LinkedIn, and Healthgrades, as described in previous studies. 7,11,26
The academic and professional degree(s), specialty, subspecialty, work region, academic rank, gender, age, race, medical school, residency program, fellowship program, personal Scopus Hirsch index (h-index), and year of training completion were successfully obtained for each TP. The h-index is a measure of the productivity and citation impact of research publications, where h is the number of articles in which each has been cited at least h times. We used previously described methods for race designation, with categories (White, African American, Asian American, Latin American, American Indian/Native Hawaiian/Native Alaskan/Pacific Islander) chosen based on current racial classifications used by the US Census Bureau. 2,17,32 Next, all physicians’ names were cross-referenced with lists of the past presidents of 7 national medical societies (American Orthopaedic Society for Sports Medicine [AAOSM]; Arthroscopic Association of North America [AANA]; Fellow of the American Academy of Orthopaedic Surgeons [FAAOS]; International Society of Arthroscopy, Knee Surgery and Orthopaedic Sports Medicine [ISAKOS]; American Shoulder and Elbow Surgeons [ASES]; American Academy of Family Physicians [AAFP]; and American College of Physicians [ACP]), as well as with the editorial boards of The American Journal of Sports Medicine and Arthroscopy.
Linear regression was performed to determine the correlation between the time since education completion and h-index, as well as the duration of NFLPS membership and h-index. Next, independent t tests were performed to assess for differences in the h-index of TPs with academic rank versus those without, differences in the mean h-index of HTPs and ATPs, differences in the duration as a member of the NFLPS in HTPs versus ATPs, and differences in age between HTPs and ATPs. All statistical analyses were performed using SPSS Version 23 (IBM). The threshold for statistical significance was set at P < .05.
Results
A total of 170 TPs were identified via the NFLPS website, with 21.2% listed as HTPs and 78.8% as ATPs. Of the HTPs, 75% were orthopaedic surgeons while the remaining 25% were internists or family medicine physicians. Of the 170 TPs, 38.2% were designated as NFLPS voting members, including all HTPs. HTPs and ATPs had mean ages of 56.2 ± 9.6 and 52.6 ± 9.6 years, respectively (P = .047). TPs were 97.6% male with a mean age of 53.4 ± 9.7 years. By race, TPs were 91.2% White, 3.5% African American, 3.5% Asian American, 1.8% Latin American, and 0% American Indian/Native Hawaiian/Native Alaskan/Pacific Islander (Table 1). In addition, 97.1% of TPs were graduates of an allopathic (MD) medical school. The most common medical specialties were orthopaedic surgery, internal medicine, family medicine, emergency medicine, and physical medicine and rehabilitation (Figure 1).
Characteristics of NFL Team Physicians (N = 170) a

a Data are reported as n (%) unless otherwise indicated. ATP, assistant team physician; HTP, head team physician; NFL, National Football League; NFLPS, National Football League Physicians Society; TP, team physician.
b The following NFL teams had 2 head physicians listed on the NFLPS website: Dallas Cowboys, Washington Football Team, Arizona Cardinals, and Pittsburgh Steelers.
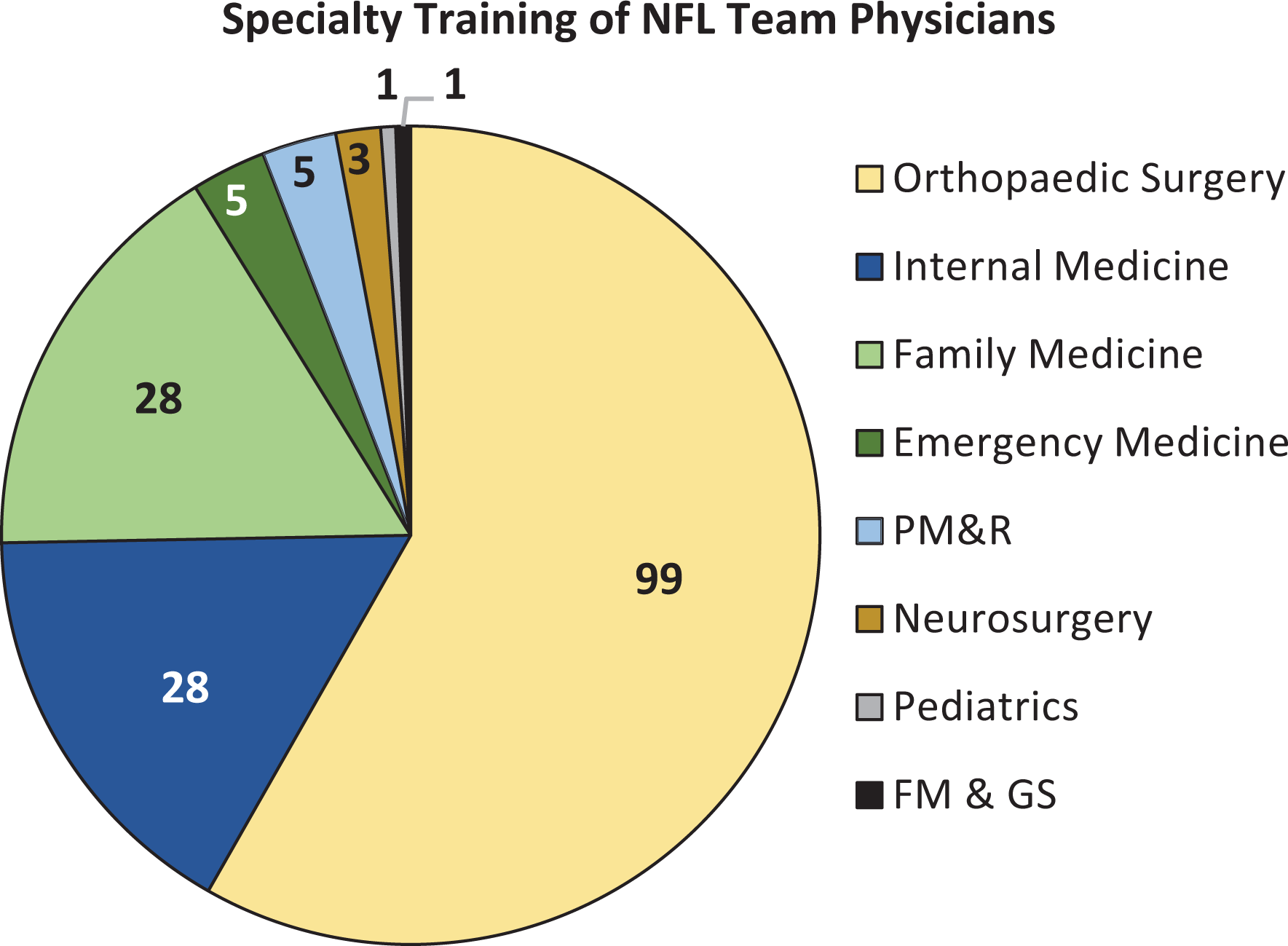
The most common medical specialties among NFL team physicians. FM & GS, family medicine and general surgery; NFL, National Football League; PM&R, physical medicine and rehabilitation.
The most common orthopaedic residency institutions were the Hospital for Special Surgery (HSS) in New York City, New York (15.2%), and the University of Pennsylvania in Philadelphia, Pennsylvania (5.1%) (Figure 2). Of the 99 orthopaedic surgeons who are members of the NFLPS, 96 completed at least 1 fellowship after residency. The most common fellowship subspecialties were sports medicine (70.5%), foot and ankle (7.6%), spine (5.7%), hand (5.7%), trauma (3.8%), and shoulder (3.8%) (Figure 3). The most common institution for fellowship training among orthopaedics was also HSS, with 17 surgeons (17.7%) graduating from the program. Other heavily attended fellowship programs include the American Sports Medicine Institute in Birmingham, Alabama (9.4%) and Harvard University (9.4%) (Figure 4). Interestingly, 48.2% of TPs worked for a team in the same state in which they graduated residency, and 32.9% worked for a team in the same state in which they graduated fellowship. Individuals worked for a mean of 9.1 years (range, 0-43 years) after finishing their specialty training before joining the NFLPS. HTPs and ATPs had been in the NFLPS for a mean of 16.9 ± 10.8 and 8.8 ± 8.3 years, respectively (P < .001) (Table 2).
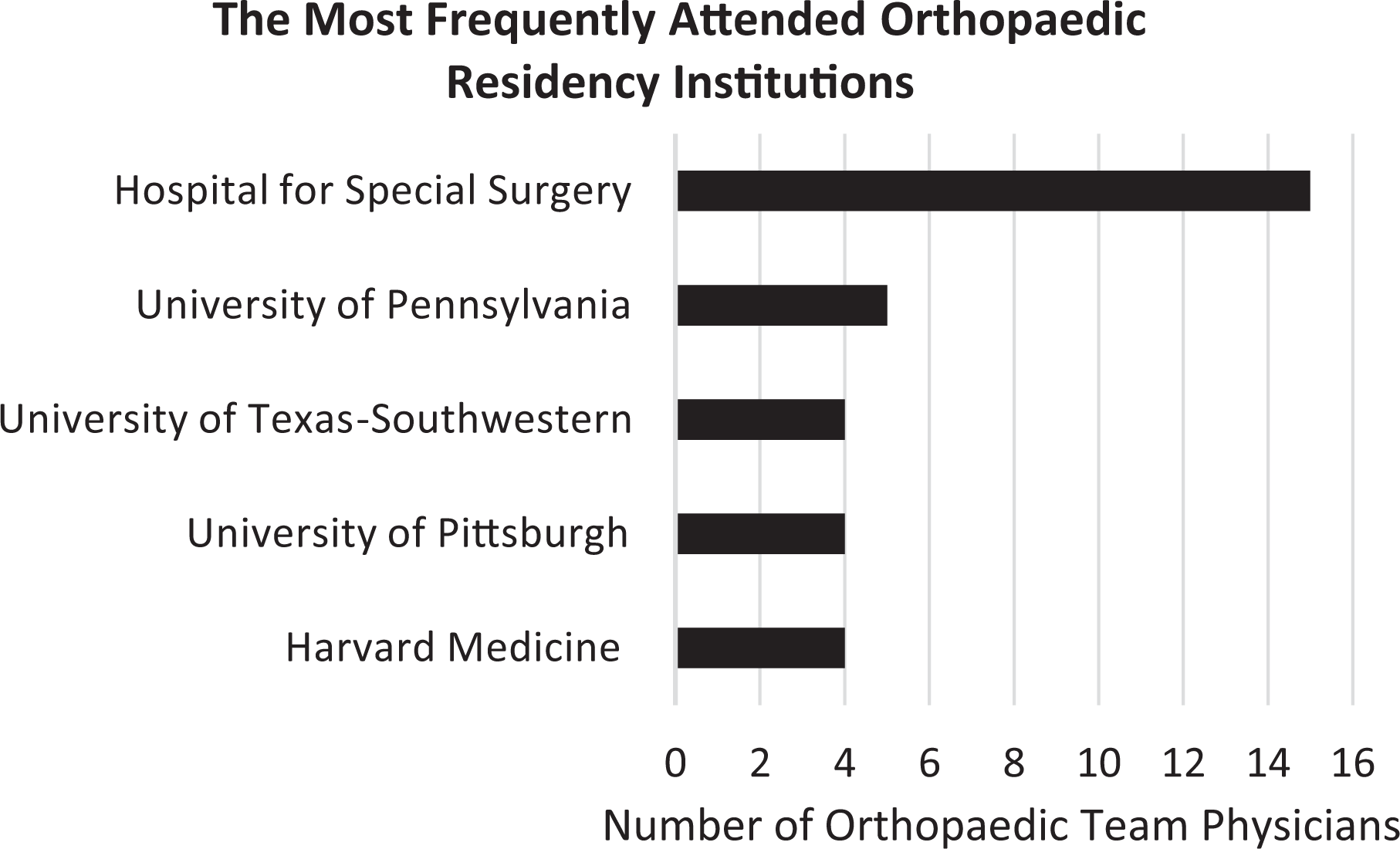
The most attended residency training programs among current orthopaedic National Football League Physician Society members. Included were residency programs at which at least 4 orthopaedic team physicians trained.

The most common orthopaedic subspecialties among National Football League (NFL) orthopaedic team physicians.

The most attended fellowship training programs among current orthopaedic National Football League Physician Society members. Included were fellowship programs at which at least 8 orthopaedic team physicians trained.
Education, Employment, and Leadership Progression of NFL Team Physicians a

a Data are reported as n (%) unless otherwise indicated. AJSM, The American Journal of Sports Medicine; ATP, assistant team physician; HTP, head team physician; NFLPS, National Football League Physicians Society; TP, team physician.
b TPs for Washington Football Team were included if residency/fellowship was completed in Maryland or Virginia, and TPs for Kansas City Chiefs were included if residency/fellowship was completed in Kansas or Missouri.
c Societies included were American Orthopaedic Society for Sports Medicine; Arthroscopic Association of North America; Fellow of the American Academy of Orthopaedic Surgeons; International Society of Arthroscopy, Knee Surgery and Orthopaedic Sports Medicine; American Shoulder and Elbow Surgeons; American Academy of Family Physicians; and American College of Physicians.
d Statistically significant difference in groups compared (P < .05).
In terms of medical society and editorial board leadership, 5.1% of TPs have served as a president of 1 of 7 major medical societies (AOSSM, AANA, FAAOS, ISAKOS, ASES, AAFP, and ACP), and 5.3% currently hold a seat on the editorial board of The American Journal of Sports Medicine. Of all TPs, 60% had attained an academic rank, with 31.2% as assistant professors, 15.3% as associate professors, 9.4% as professors, and 4.1% as department chairs (Table 2). The research background of all TPs revealed an h-index range of 0 to 113. The mean h-index of all TPs was 11.0 ± 16.4, and 9 TPs had scores ≥41 (Figure 5, Tables 2 and 3). Further, TPs with and without an academic rank had an h-index of 14.0 ± 19.3 and 6.2 ± 8.8 (P < .01) and HTPs and ATPs had mean h-indices of 15.7 ± 15.9 and 9.6 ± 16.3 (P = .0503), respectively (Table 2).

Scopus Hirsch index (h-index) values of team physicians within the National Football League (NFL). h-Index values were as of December 9, 2021.
Most Productive Team Physician Researchers

a The h-index values are as of December 9, 2021.
Discussion
The most noteworthy findings of this study can be grouped into 4 main subjects. First, our demographic analysis revealed that NFL TPs are 97.6% male, 91.2% White, and 53.4 ± 9.7 years of age. Second, our examination of the educational background of TPs showed a majority with orthopaedic surgery specialization (58.2%) and, within that group, a majority with sports medicine subspecialization (74.7%). Third, our review of TP research productivity found great variety with a mean h-index of 11.0 ± 16.4. Lastly, there is minimal gender and racial diversity among NFPLS members, with 97.6% classified as male and 91.2% racially classified as non-Latino White. To the best of our knowledge, this is the first study to analyze TPs within the NFLPS based on demographics, educational background, and research output.
Although the NFL comprises 32 teams within 22 different states across the United States, our data reveal many common features among TPs within the NFLPS. Most TPs specialize in orthopaedic surgery, and the majority of orthopaedic and nonorthopaedic TPs pursued additional sports-specific subspecialty training. Our findings that a large proportion of physicians specialize in sports medicine is aligned with the 2011 collective bargaining agreement between the NFL and NFL Players Association mandating the board certification of all NFLPS physicians in sports medicine. 8 However, this has not prevented some teams from retaining physicians with extensive training in pulmonology, cardiology, nephrology, or neurosurgery. Orthopaedic surgeons with advanced fellowship training in the domains of trauma, shoulder surgery, and joint replacement are also seen within the NFLPS.
The educational background of TPs demonstrated a strong presence of elite training institutions. HSS, often ranked as one of the best orthopaedic training institutions in America, topped the list for most common residency and fellowship training locations of NFLPS orthopaedic surgeons. 24 With 53.1% of fellowship-trained orthopaedic TPs receiving instruction at 5 top institutions (Figure 4), we can infer a possible association between training institution and NFLPS membership. Since many highly regarded orthopaedic fellowship programs are not well represented, networking bias may be at play in helping certain graduates attain NFLPS status over others. For example, attending one of these fellowships may help with connections given that many alumni and physicians directly involved in training at these programs are active in professional sports. 23,28 Although a slight majority of orthopaedic TPs were trained at 5 institutions, 34 other fellowship programs were represented, suggesting that there are multiple training routes to becoming a TP.
Research accomplishments among TPs in the NFL are quite variable, suggesting that research attainment may be less important to becoming a TP. The h-index was originally developed to objectively assess an individual’s research accomplishments using a formula that considers both number of publications and citations received. 27 Of 170 TPs, 42 have attained a score >11, while 55.8% of NFLPS members had an h-index between 0 and 5 (Table 3). A study completed by Bastian et al 4 reported that the h-indices of orthopaedic surgeons with the rank of assistant professor, associate professor, professor, and chair were 3.6, 8.4, 15.1, and 17.8, respectively. Our data show that TPs, with a mean h-index of 11, have research output ranking between that of associate and full professors of orthopaedic surgery, However, the top-heavy h-indices among select physicians have skewed the mean values to be much greater than the median value of 4, which falls more closely to assistant professor. 4 Nevertheless, HTPs had a higher mean h-index than ATPs, which may support the NFLPS’s interest in promoting HTPs who are leaders in research. Although making up just 21.2% of all TPs, HTPs accounted for 40% of the top 10 h-indices recorded.
Over the past decade, racial diversity within NFL front offices and coaching staffs has been under substantial scrutiny across media platforms, and the NFL has made an effort to increase diversity among leadership positions. League-wide hiring rules have required NFL teams to interview URMs for upper-level management positions; however, in 2021, URMs still made up only 15.6% of general managers or head coaches across the league. With 58% of players self-identifying as African American, the racial gap between players and those in senior management is significant. 13,16 Nevertheless, the racial discrepancies between players and team doctors is even more disparate. Wiggins et al 32 found that the NFL had the lowest proportion of minority HTPs (Asian American, African American, and Latin American) when compared with other professional sports leagues. In fact, only 11.8% of HTPs were identified as a minority.
Our study found similar racial disparities across all NFL TPs, with 91.2% being non-Hispanic White, compared with 5.3% URMs (defined by the American Academy of Orthopaedic Surgeons as African American, Latin American, American Indian, Pacific Islander, or multiracial) (Table 1). When subdivided by specialty, orthopaedic surgery heavily contributes to this disparity, with African Americans accounting for 2% (2 of 99) of all orthopaedic team doctors, while African American physicians comprise 11.3% (8 of 71) of all remaining nonorthopaedically trained NFLPS members. The lack of diversity among NFLPS orthopaedic surgeons undoubtedly stems from the minimal minority representation within the specialty as a whole. According to the American Academy of Orthopaedic Surgeons (AAOS) Governance Diversity Report, only 4.7% of its members self-identify as a URM. 1 This lack of racial diversity becomes particularly important when caring for NFL players because studies show that trust and satisfaction scores significantly increase when patients and physicians identify as the same race/ethnicity. 3 , 29
Gender disparities also exist, with our data showing an even smaller proportion of female TPs within the NFL (2.4%) when compared with other professional leagues and college conferences (6.7%-18.1%, depending on the level of competition and gender of the athletic program). 22 Further, even though women make up 6.8% of all AAOS members, our study found that they only make up 2% (2 of 99) of orthopaedic NFLPS TPs (Table 1). While this does not account for other medical specialties in sports medicine, it is clear that the female orthopaedic representation within the NFL is far below the percentage of women within orthopaedics. 6 Female underrepresentation within orthopaedics has also been seen in leadership positions across many orthopaedic specialty societies, including The Knee Society and The Hip Society, which have the lowest percentages of women at 0.5% and 0.6%, respectively. 5 Thus, this lack of diversity among NFLPS members and TPs is not unexpected.
There are many ways by which the NFL can tackle the lack of diversity within its TP population. The NFL’s 2021 Diversity and Inclusion Report outlines multiple recommendations to increase diversity among head coaches, but many of these strategies could be implemented during the hiring process of new TPs as well. For instance, including select players (4 players with at least 2 self-identifying as URMs) during a TP interview and hiring process could ensure a high level of trust and respect between players and their doctors. 13 Even if this is implemented, a major hurdle for increasing minority inclusion within the NFLPS is their lack of representation within orthopaedic surgery and its residencies. While a recent study has shown that female representation within residency increased by 3% (12.4%-15.4%) from 2007 to 2019, the number of minorities, particularly those who identify as African American, has decreased by 0.4% (4.0%-3.6%) over the same time period. 21 This trend indicates that orthopaedic residencies may need to change recruiting practices to increase racial diversity among resident applicants as well as those accepted into orthopaedic residencies. Proposed strategies to increase African American representation among residencies include actively recruiting persons of color, increasing the diversity of orthopaedic faculty, and department leadership becoming more involved in diversity-related organizations. 20 Such upstream changes would allow for a more diverse applicant pool in the fellowship match, attending physician job market, and, eventually, applicants to NFL TP positions.
Limitations
The present study is not without limitations, and our data may have been incomplete for 2 reasons. First, the NFLPS does not contain every physician who is affiliated with an NFL team, including unbiased concussion specialists and team consultants. Second, for information unable to be obtained from an updated CV, it is possible that information pertinent to some TPs is not entirely accurate or up to date. Since our study did not ask each physician their own racial identity through direct surveys, improper categorization may have occurred, especially for those with multiracial backgrounds. Nevertheless, we used a peer-reviewed published methodology for systematically inferring racial identity, so we believe it is an adequate representation. Furthermore, this study only looked at 1 sport (professional football in the United States); thus, the outcomes may not apply to recreational, college, or other professional sports. It is also difficult for this study to capture the variety of unique, immeasurable factors that may lead a doctor to become a TP, or specifically an HTP. For example, many TPs may once have been former athletes or have socially significant connections to those within a team. Lastly, while the h-index is a validated metric for understanding an author’s scholarly impact, it is unable to reflect all types of research output, including book chapters; international, national, and regional podium presentations; committee participation; and conference leadership roles.
Conclusion
TPs in the NFL are typically White men in their mid-50s who have trained at certain high-ranking institutions and obtained a fellowship in sports medicine. HTPs are likely to be older with longer tenures within the NFLPS and with more impactful research than their ATP counterparts. Also, gender and racial disparities exist within the NFLPS, and increasing diversity may cultivate stronger patient-physician relationships between players and their physicians. Understanding these features will help guide young surgeons interested in professional sports team coverage and uncover potential opportunities for URM physicians to play a larger role in team coverage for professional sports leagues like the NFL.
Footnotes
Final revision submitted January 18, 2023; accepted February 26, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: P.R.S. has received hospitality payments from Stryker. M.A.T. has received nonconsulting payments from Arthrex and Smith & Nephew and hospitality payments from Medwest. V.K.T. has received education payments from Medwest, consulting fees and nonconsulting fees from Smith & Nephew, and hospitality payments from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.