
Abstract
Background:
Shoulder pain is common, with a lifetime prevalence of up to 67%. Evidence is conflicting in relation to imaging findings and pain in the shoulder. Sonoelastography can be used to estimate tissue stiffness and may be a clinically relevant technique for diagnosing and monitoring tendon healing.
Purpose:
To evaluate changes in supraspinatus tendon stiffness using strain elastography (SEL) and associations with changes in patient-reported outcomes, supraspinatus tendon thickness, and grade of tendinopathy after 12 weeks of unilateral shoulder exercises in patients with supraspinatus tendinopathy.
Study Design:
Controlled laboratory study.
Methods:
A total of 23 patients with unilateral clinical supraspinatus tendinopathy performed 12 weeks of “standard care” exercises. At baseline and follow-up, supraspinatus tendon stiffness was measured bilaterally using SEL and compared with tendinopathy grading on magnetic resonance imaging scans and tendon thickness measured using conventional ultrasound. Patient-reported outcome measures included physical function and symptoms from the Disabilities of the Arm, Shoulder and Hand questionnaire and pain rating (visual analog scale).
Results:
No significant changes in SEL within or between groups (asymptomatic vs symptomatic tendon) were seen. All patient-reported outcomes showed significant improvement from baseline to follow-up, but with no change in tendinopathy grading and tendon thickness. No significant differences in the proportion of patients changing above the minimal detectable change in SEL and PROM were seen, except for discomfort while sleeping.
Conclusion:
Despite no significant within-group or between-group changes in SEL, significant improvements were found in patient-reported outcomes. An acceptable agreement between patients changing above the minimal detectable change in SEL and patient-reported outcome measure was seen. Further studies should explore the use of SEL to detect changes after tendon repair and long-term training potentially in subgroups of different tendinopathy phases.
Clinical Relevance:
In the short term, structural changes in supraspinatus tendons could not be visualized using SEL, indicating that a longer time span should be expected in order to observe structural changes, which should be considered before return to sports. Subgrouping based on stage of tendinopathy may also be important in order to evaluate changes over time with SEL among patients with supraspinatus tendinopathy.
Registration:
NCT03425357 (ClinicalTrials.gov identifier).
Keywords
Shoulder pain is common in the general population, with a lifetime prevalence estimated to be up to 67%. 24 A common cause of shoulder pain is subacromial pain syndrome including supraspinatus tendinopathy, 37 which may lead to functional disability as well as reduction in health-related quality of life. 1 Tendinopathy is conceptualized as a continuum of stages, ranging from short-term adaptions to increased load through degeneration due to long-term overload. 6 Pain may be present at all stages of this continuum, making categorization of a specific stage difficult to assess clinically. The chronic stage of tendinopathy involves collagen breakdown and vascular alterations, 33 which can be seen using conventional ultrasound (US). However, there is conflicting evidence about the correlation between imaging findings and pain in the shoulder because pathologies may also exist in asymptomatic individuals. 36 It is not assumed that changes in the chronic stage of tendinopathy are reversible, but exercise may optimize the function of the remaining healthy tendon structure including improved elasticity and thereby function of the tendon. Elasticity is not measurable using existing imaging modalities, such as conventional US. However, sonoelastography can be used to estimate tissue stiffness by evaluating tissue stress response and may be a clinically relevant technique for diagnosing and monitoring tendon healing. 30
In the musculoskeletal area, shear wave elastography (SWE) and strain elastography (SEL) are of interest. In SWE, the US transducer produces a horizontally focused radiation force, which results in high-intensity shear waves traveling through the tissue. 28 In contrast, SEL is based on manual transducer compressions, where soft tissue is deformed differently from stiff tissue. It has been recommended to present ratios between the region of interest and a reference area because the applied stress in SEL cannot directly be measured. 9,12 SEL has shown satisfactory reliability 4 and validity in patients with supraspinatus tendinopathy and healthy volunteers. 3,23 Follow-up evaluation of tissue elasticity using sonoelastography has, to our knowledge, only been estimated in 2 studies, both of which involved only the Achilles tendon. 5,39 In both studies, 1 using SEL 5 and the other using SWE, the Achilles tendon had undergone surgery and was significantly stiffer 1 year later. 39
In clinical practice, exercises are the first line of treatment for the majority of shoulder diagnoses, and 12 weeks of training is recommended as the minimum duration of exercise treatment before evaluating patient-reported outcome in the shoulder. 7 However, changes in SEL after such exercise treatment in patients with supraspinatus tendinopathy have not been studied. The first objective of this research was therefore to investigate changes in supraspinatus tendon stiffness using SEL after 12 weeks of unilateral shoulder exercises in patients with clinically diagnosed unilateral supraspinatus tendinopathy and compare these changes with stiffness changes in the same patients’ asymptomatic shoulder. We hypothesized that SEL would demonstrate measurable changes in suprapinatus tendons in patients with tendinopathy. The second objective was to report changes in the symptomatic tendon with respect to patient-reported outcomes, tendon thickness using conventional US, and grading of tendinopathy on magnetic resonance imaging (MRI) scans and evaluate the agreement of these changes with those using SEL of the symptomatic tendon.
Methods
The current study was an exploratory prospective cohort study using the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 38 The study protocol was approved by the regional ethics committee, reported to the Danish Data Protection Agency (2014-41-3266), and registered at ClinicalTrials.gov (NCT03425357). Written informed consent was provided by all patients before participation.
Patient Recruitment
Patients were consecutively recruited between February 2018 and January 2019 from a single institution. Inclusion criteria were age 40 to 60 years and body mass index (BMI) <30 (to optimize image quality), unilateral shoulder pain ≥3 months, and positive signs from at least 3 of 5 clinical tests including the full-can test, 20 Jobe test, 18 resisted external rotation test, 21 Hawkins-Kennedy test, 13 and Neer impingement test. 27 Exclusion criteria for both shoulders were any of the following: (1) MRI-verified biceps ruptures, labral lesions, glenohumeral arthrosis, and full-thickness rotator cuff tears; (2) clinical suspicion of periarthritis or symptoms derived from the neck (based on clinical examination from an orthopaedic surgeon); (3) US-verified supraspinatus tear more than one-third of the vertical height of the tendon (because the stress is increased on the intact tendon part) and calcifications >2 mm in length (due to low US penetration depth in hard structures); and (4) previous comorbidity (shoulder fractures, surgery and luxation, known neuromuscular disease, rheumatoid arthritis, cancer, fibromyalgia, spondyloarthropathy, psychiatric disorders), pregnancy, inability to read and understand Danish, and inability to follow the exercise intervention.
After recruitment, the patients underwent baseline measurements. The testing procedures lasted approximately 1 hour. After inclusion and baseline tests, all patients were instructed in the exercise program by an experienced physiotherapist (K.G.I.). Finally, patients underwent MRI, which was performed within approximately 1 week after the baseline tests. Follow-up MRI examinations were performed as close to the 12-week follow-up tests as possible. SEL, US, and MRI were performed bilaterally; however, MRI and US of the asymptomatic shoulder were used only for identifying exclusion criteria and, regarding MRI, for blinding the radiologist between symptomatic and asymptomatic tendons during tendinopathy grading.
Intervention
The exercise program consisted of 2 exercises for the scapula-stabilizing muscles, 2 exercises for the rotator cuff muscles, and 2 mobility exercises for the rotator cuff and scapulothoracic complex. This intervention has previously been shown to produce significant improvement in pain and function in patients with supraspinatus tendinopathy. 17 The intervention was primarily home-based for 12 weeks, with 2 supervised control sessions (corrections and weight adjustment) after 4 and 8 weeks. The exercises were performed in 3 sets with 15 to 25 repetitions per set 3 times per week for 12 weeks. Loads were individually tailored, making it possible for all patients to complete the sets correctly and with an acceptable pain level. 35
Patients were asked to train only the symptomatic arm and, further, not to seek any other treatment during the intervention. Pain-relieving medication was allowed in the intervention period, but patients were instructed not to use it the same day as baseline and follow-up tests to ensure equal/actual pain experience. Patients recorded the number of sets and repetitions per set for each training session in a diary. A total of 648 exercise sets (12 weeks × 3 sessions/week × 3 sets × 6 exercises) were defined as 100% compliance. Patients were asked not to train on the same day the follow-up tests took place.
Strain Elastography
Apparatus
A LOGIQ S7 (GE Healthcare) equipped with a high-frequency linear probe (15-MHz linear probe) was used for SEL examinations. The settings and procedures recommended by the manufacturer (GE Healthcare, personal communication with application specialist in Ultrasound, Heidi Sørensen, 2018) were used for SEL on the shoulder.
Patient Placement
The supraspinatus tendons were scanned bilaterally while the patient was sitting in a custom-made chair ensuring the upper limb was held in a standardized position (at both baseline and follow-up), with the hand placed on the backrest, as previously described. 4
Image Capturing
Conventional US was used to locate the most affected part in the tendon regarding neovascularization and fibrillar disruption, and SEL measurement was performed at this site. Where no such tendon changes were identified using conventional US, SEL was captured in a standardized position, with the probe placed laterally from the anterior-lateral corner of the acromion as previously described. 4 Image window depth and width and the tissue compression force technique were performed according to previous recommendations. 8,12 Only high-quality images, determined by an in-built software quality bar, were used for analysis, as recommended by the manufacturer (GE Healthcare, personal communication with application specialist in Ultrasound, Heidi Sørensen, 2018). To minimize intraobserver variation, measurements were based on 3 (20-second) cine loops, as previously recommended. 8
Image Measurements
Tendon stiffness measured using SEL was assessed using 2 different quantitative approaches. These included the raw strain index (RAW; continuous scale from 0 = softest tendon to 6 = stiffest tendon) and a ratio between the selected tendon area and a soft part of the deltoid muscle (DELT), calculated as the strain value of the supraspinatus tendon divided by the DELT value, as previously described. 4 The SEL was performed and assessed by a radiographer (K.B.) with 4 years of experience in musculoskeletal SEL. Images were assessed at least 14 days after capturing to minimize investigator memory of pain response from the affected side during SEL measurements and to keep blinding of the investigator regarding symptomatic and asymptomatic sides.
Magnetic Resonance Imaging
MRI examinations were performed bilaterally on the shoulders using the MAGNETOM Skyra 3-T MRI scanner (Siemens Medical Solutions) and consisted of a transverse, coronal, and sagittal fat-suppressed proton density–weighted sequence and a coronal T2-weighted sequence. The MRI scans were graded using a previously established protocol for estimation of tendinosis or tendinopathy in the supraspinatus tendon, ranging from grade 0 (normal) to grade 3 (marked tendinosis/tendinopathy). 31 A radiologist with >20 years of experience in musculoskeletal imaging (J.H.), who performed the MRI gradings, initially had access to the patient’s history, as this combined knowledge was important for potential exclusion of the patient from the trial based on imaging analyses and also for the patient’s further treatment. After determining eligibility of the patients, the images were regraded for analyses by the same radiologist, blinded to patient history, approximately 6 months later (mixed with MRI scans from the patients’ asymptomatic shoulder).
The time between MRI capturing and the remaining baseline tests and the time between MRI capturing and the remaining 12 weeks of follow-up tests were on average 4 days. During all MRI gradings or ratings, the radiologist was blinded toward SEL and conventional US findings.
Ultrasound
Tendon thickness was measured by a clinician with >7 years of experience in musculoskeletal US (K.G.I.) using the GE LOGIQ S7 fitted with a 15-MHz linear dedicated probe with standardized settings, as recommended by the manufacturer (GE Healthcare, personal communication with application specialist in Ultrasound, Heidi Sørensen, 2018). Standardized image capturing and measurements were performed according to a previously described protocol just laterally from the anterior-lateral corner of the acromion in the longitudinal plane. 14,16
Patient-Reported Outcomes
Patient-reported outcomes consisted of questionnaires in the form of the Disabilities of the Arm, Shoulder and Hand (DASH) for investigating disability of both upper extremities (range, 0-100; 100 = most disabled), 22 the visual analog scale (VAS) for pain (range, 0-100; 100 = the most painful) on the symptomatic side, 2 and the global perceived effect (GPE) for investigating overall pain improvement or worsening on the symptomatic side (range, –3 to 3; –3 = much worse, 3 = much better). 19 Patient data included self-reported information on age, sex, BMI, duration and origin of symptoms, symptomatic shoulder side (dominant or nondominant), corticosteroid injection(s) within the past 6 weeks, and the patient’s workload and work ability.
Statistical Analysis
A histogram with a normal distribution curve was used to verify normality for the continuous data, with all continuous variables except for tendon thickness and duration of symptoms being normally distributed. Patient characteristics are presented as mean ± SD for normally distributed data (continuous scales) and median (interquartile range) for nonnormally distributed data (continuous or ordinal scales), while nominal data are presented as frequency and percentage.
A paired t test with 95% CI was used to compare within-group change scores of SEL (change from baseline to follow-up for symptomatic and asymptomatic tendons, independently), as well as between-group differences in changes from baseline to follow-up (symptomatic vs asymptomatic tendon). To visualize the number of patients with a SEL change larger than the minimal detectable change (MDC; symptomatic or asymptomatic shoulders) related to baseline characteristics, scatterplots of patients’ SEL change (y-axis) and SEL baseline value (x-axis) were made, with horizontal lines indicating the MDC of SEL, defined as 0.28 for RAW and 2.91 for DELT 4 (Figure 1). The number of patients who had a minimal clinically important change (MCIC) on the DASH, VAS, and GPE was reported, as well as the mean change. Cutoffs of ≥12 change points on the DASH, 25 ≥2 change points on the VAS, 29 and ≥2 on the GPE (“somewhat better” or “much better”) were used to define MCIC.
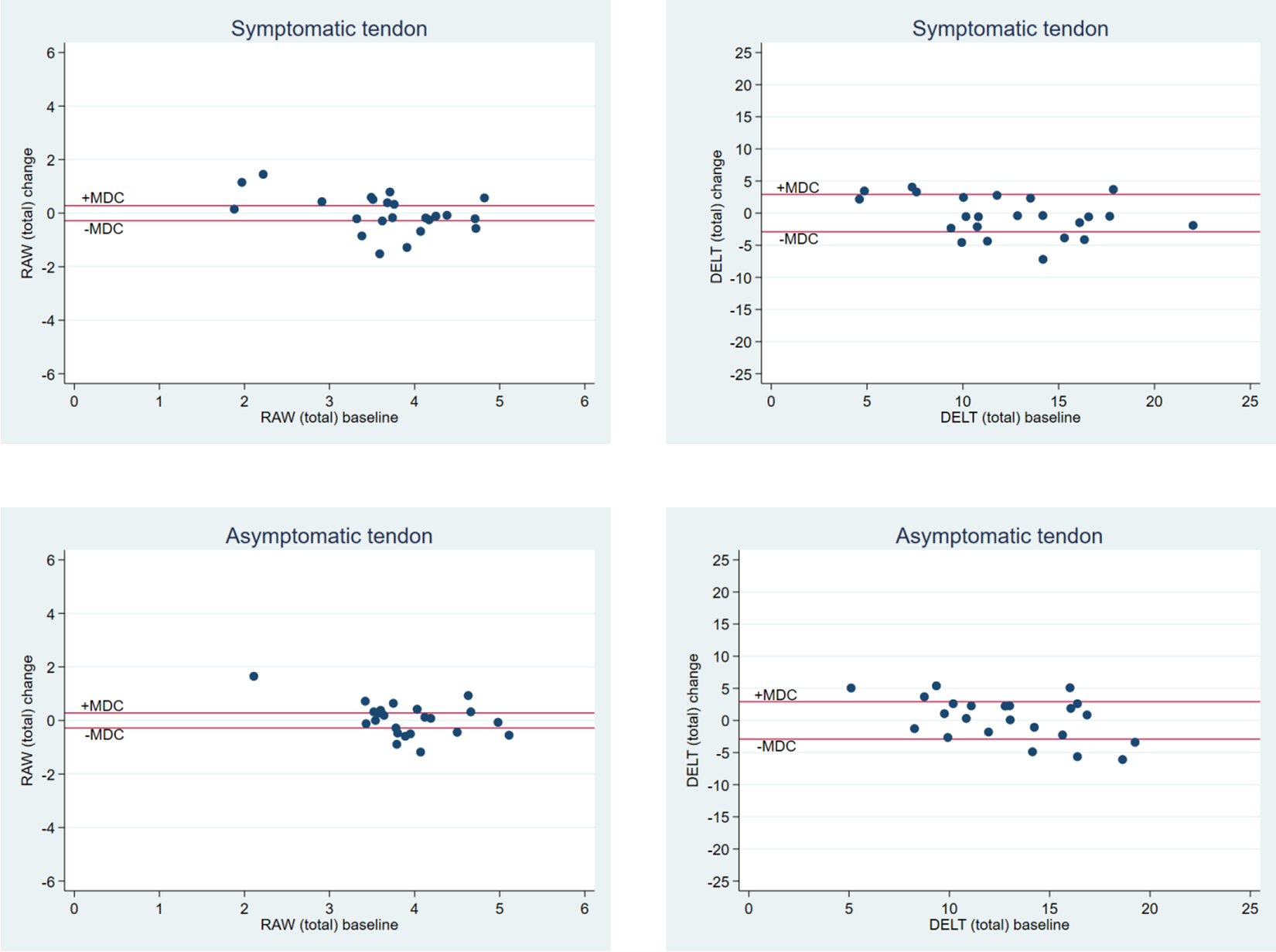
Scatterplots of baseline values (x-axis) and changes (y-axis) in the (total) symptomatic and the asymptomatic supraspinatus tendons using raw elastography data (RAW) and the ratio with the deltoid muscle as reference (DELT). A larger baseline value and a positive change value indicate increasing tendon stiffness. The reference lines illustrate the upper and lower boundaries of the minimal detectable change (MDC).
Changes from baseline to follow-up on the DASH and the VAS for the symptomatic shoulder were reported and tested using a paired t test with 95% CI, while changes in MRI-verified tendinopathy and tendon thickness (from US) for the symptomatic shoulder were tested using a Wilcoxon signed rank test. A McNemar test was used to determine if the number of patients with a SEL above the MDC was different from the number with patient-reported outcomes or a tendon thickness above the MDC. Cutoffs of ≥10.81 change points on the DASH, 11 ≥1.33 change points on the VAS, 34 and ≥0.33 mm for changes in tendon thickness 15 were used.
Two-sided statistical significance was defined as P ≤ .05. Statistical analyses were carried out in SPSS, Version 25.0 (IBM Corp).
Results
Of the 29 patients included in the study, 6 patients did not complete the study because of other acute illnesses (n = 2), death in the family (n = 2), or lack of desire to continue with the research (n = 2). The majority of patients were women, and the mean age was 51 years. The patients had an average BMI of 26 and had experienced shoulder symptoms for 9 months on average (Table 1).
Characteristics of Patients With Supraspinatus Tendinopathy (N = 23) a
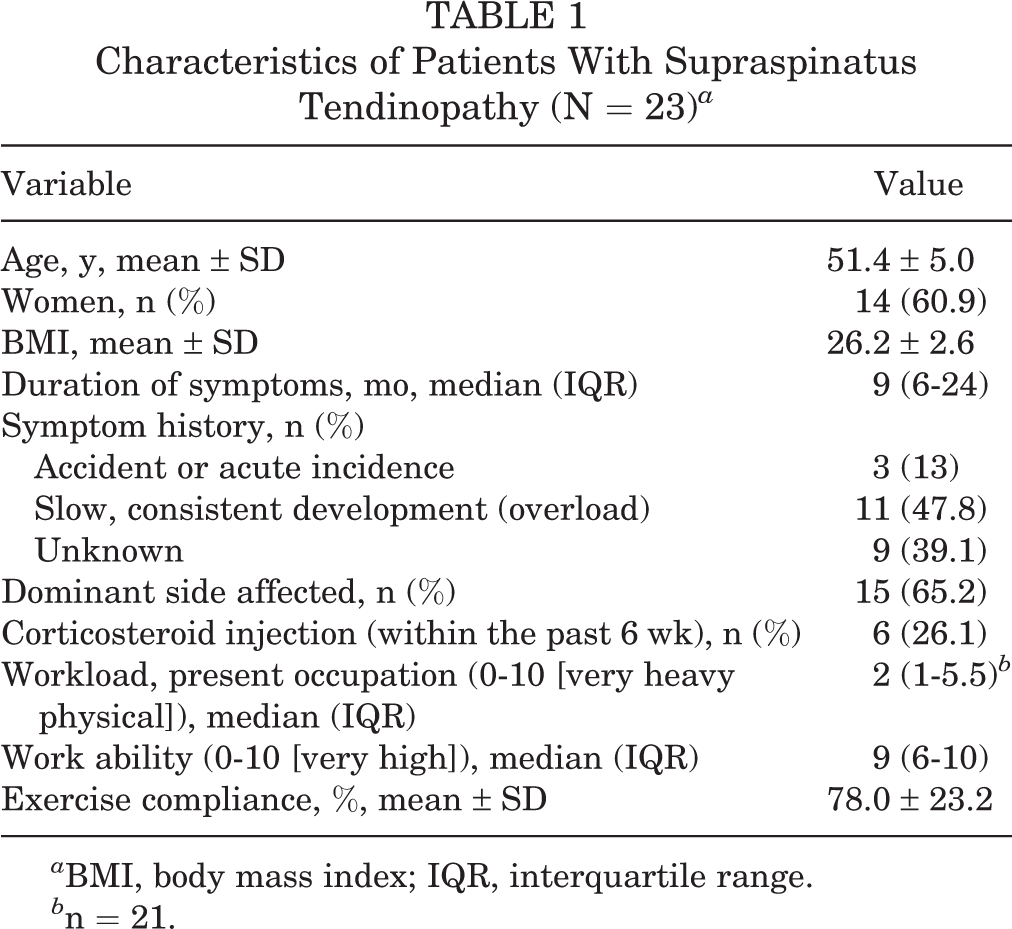
a BMI, body mass index; IQR, interquartile range.
b n = 21.
No significant within-group changes (from baseline to follow-up SEL) or between-group differences in change scores of SEL (asymptomatic vs symptomatic tendon) were observed (Table 2).
Baseline and Follow-up SEL Values for RAW and DELT and Within- and Between-Group Changes Between Symptomatic and Asymptomatic Shoulders (N = 23) a
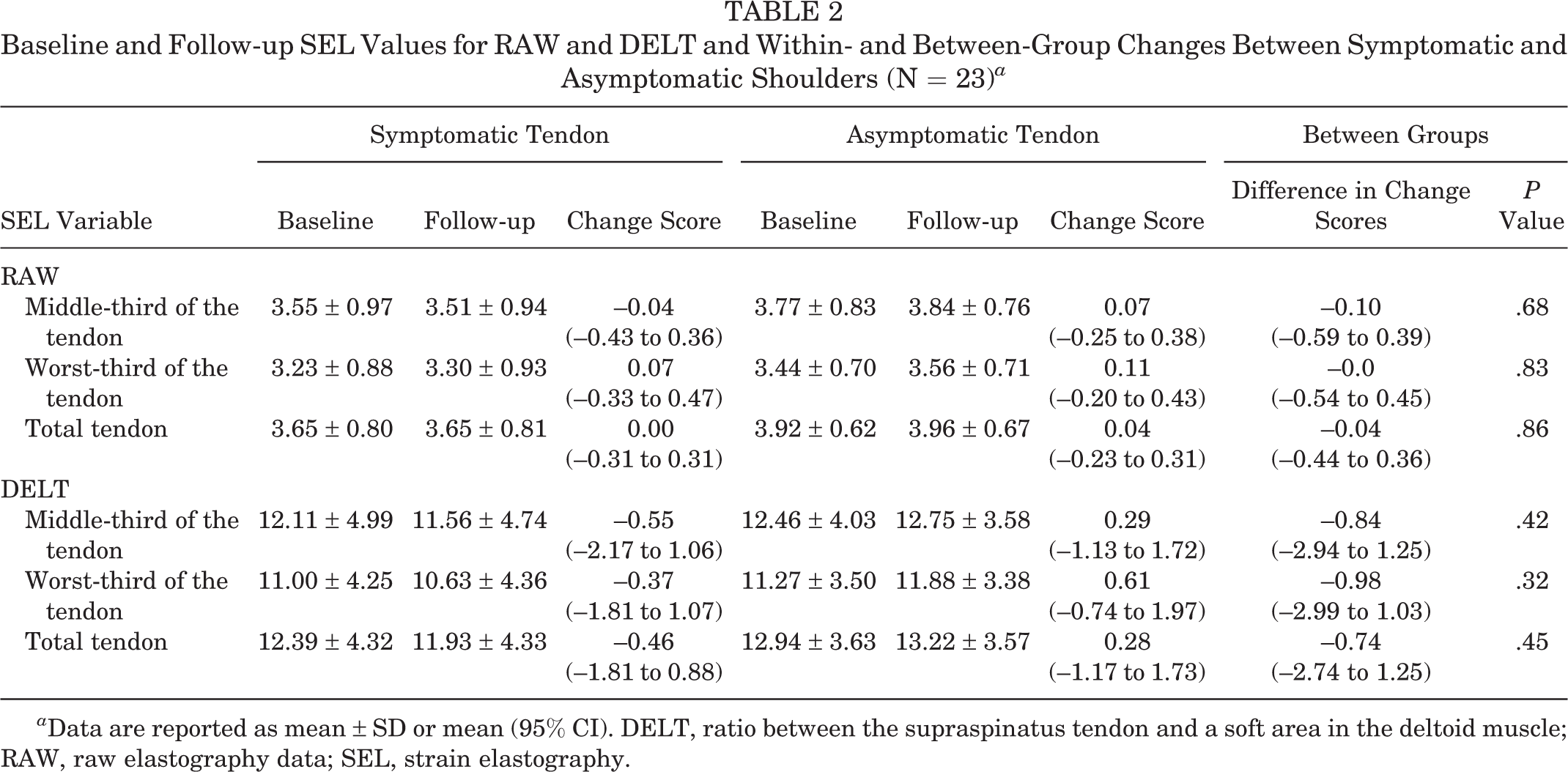
a Data are reported as mean ± SD or mean (95% CI). DELT, ratio between the supraspinatus tendon and a soft area in the deltoid muscle; RAW, raw elastography data; SEL, strain elastography.
All patient-reported outcomes changed significantly from baseline to follow-up, with DASH and VAS activity above the MCIC. In 17 (74%) patients, a clinically important change was found in DASH, and this was also found in 7 (30%) patients in VAS pain during rest, 11 (48%) in VAS pain during activity, 12 (52%) in VAS pain during sleep, 10 (43%) in VAS maximum pain, and 19 (83%) in GPE (Table 3). Tendon thickness and MRI grading of tendinopathy did not change significantly from baseline to follow-up (Table 3).
Baseline, Follow-up, and Improvement in DASH (Overall Score), VAS, GPE (Overall [Follow-up] Score), Tendon Thickness, and MRI for the Symptomatic Tendon (N = 23) a

a Baseline and follow-up data are presented as mean ± SD or median (IQR) unless otherwise stated. Boldface P values indicate a statistically significant difference between baseline and follow-up (P < .05). DASH, Disabilities of the Arm, Shoulder and Hand questionnaire (0-100); GPE, global perceived effect; IQR, interquartile range; MRI, magnetic resonance imaging; VAS, visual analog scale (0-100).
b Median.
c n = 21 (2 patients were scanned with the incorrect protocol).
Variations in total tendon changes of SEL (in relation to baseline values) were present for both the symptomatic and the asymptomatic tendons (Figure 1). When RAW was used, a total of 14 patients (9 stiffer tendons vs 5 softer tendons) gained a change beyond the MDC for the symptomatic tendon compared with 15 patients (8 stiffer tendons vs 7 softer tendons) for the asymptomatic tendon. When DELT was used, a total of 9 patients (4 stiffer tendons vs 5 softer tendons) gained a change beyond the MDC for the symptomatic tendon compared with 8 patients (4 stiffer tendons vs 4 softer tendons) for the asymptomatic tendon. The same variations of tendon changes in SEL were seen for the middle and the worst part of the tendon (Appendix Figures A1 and A2).
The number of participants who had an absolute change beyond the MDC for DASH with their total SEL (RAW) scores remaining unchanged was not significantly different from the number of participants who had their total SEL (RAW) score absolute change beyond the MDC, yet their DASH score remained constant (P = .77) (Figure 2A). The same was seen for total SEL RAW and VAS pain during rest (P = .39), VAS pain during activity (P > .99), VAS pain during sleep (P = .55), VAS maximum pain (P > .99), and tendon thickness (P = .51) (Figure 2, B-F), and total SEL DELT and DASH (P = .06), VAS pain during rest (P = .75), VAS pain during activity (P = .18), VAS maximum pain (P = .23), and tendon thickness (P = .51) (Figure 2, G-I, K, L). For total SEL DELT and VAS pain during sleep, a significant difference (P = .04) was seen, with 12 patients with an absolute change larger than that for MDC VAS pain during sleep yet SEL that remained unchanged and 3 patients with an absolute change larger than that for MDC SEL and VAS pain during sleep that stayed constant (Figure 2J). The same pattern was seen for the SEL worst and SEL middle part of the tendon for both RAW and DELT.

Scatterplots of absolute change in (A-F) total SEL RAW and (G-L) total SEL DELT in relation to the absolute change in DASH, VAS rest, VAS activity, VAS sleep, VAS max, and tendon thickness. Corresponding minimal detectable change values are marked with horizontal and vertical lines. DASH, Disabilities of the Arm, Shoulder and Hand; DELT, deltoid muscle; RAW, raw elastography data; SEL, strain elastography; VAS, visual analog scale.
Discussion
After 12 weeks of shoulder training for the symptomatic shoulder, patients improved significantly on the patient-reported outcomes; however, SEL showed no significant changes. All SEL changes, except for DELT and VAS pain during sleep, had similar proportions of patients changing above the MDC of SEL while remaining within the MDC for the patient-reported outcomes, and vice versa. This indicates that there is, in general, an acceptable agreement between change in SEL and change in the patient-reported outcome measure (PROM).
The current results raise questions regarding tendinopathy and its response to training, SEL’s ability to detect changes, and the contribution of pathological findings on imaging in painful conditions, which is discussed in the following.
In the current study, no within-group or between-group differences in SEL change scores were found, and the observed mean changes for the symptomatic total tendon (0 for RAW; 0.46 for DELT) were smaller than and therefore within previously reported MDCs (0.28 for RAW; 2.91 for DELT). 4 A previous study using SEL found the ruptured Achilles tendon to be significantly stiffer 1 year after surgery compared with both the contralateral healthy side and the healthy controls. However, that study only used ratios with fat reference tissue, which hampers comparison. 5 These results were supported by a study using SWE, where the ruptured Achilles tendon also became significantly stiffer 24 weeks after surgery. 39 That study also demonstrated a positive correlation between an increased tendon stiffness and improved patient-reported outcome 48 weeks after surgery for the ruptured Achilles tendon. 39 The difference between the current and the previous results may be explained by the different diagnoses because ruptured Achilles tendons may have had a preexisting, more severe tendinopathy than the current population of nonruptured supraspinatus tendons. Another explanation may be the intervention itself, as the surgical response could increase inflammation and edema in the tendon, causing the tendon to become softer at baseline (just after surgery). After initial postoperative rehabilitation (rest, fixation, and limited weightbearing), a gradual return to normal daily activity will follow, with the aim of normalizing the strength and stiffness of the tendon. During the year postsurgery, this process is inherently accompanied by a large change in morphology and improvements in patient-reported outcomes.
The short duration of the current intervention and follow-up may also explain the current lack of change in SEL. Although 12 weeks is considered sufficient to detect a clinically important patient-reported change, 7 complete tendon healing or restoration may take up to 1 year, 10 which is why a longer intervention and/or follow-up period than 12 weeks may be needed in order to detect tendon changes using SEL. Further, changes in tendon structure after a training intervention of short-term duration are often minimal, and SEL therefore may not be able to measure these tendon changes. Although SEL has been shown to have satisfactory reliability 4,32 as well as validity 3,23,32 in both patients with and patients without supraspinatus tendinopathy, SEL may not yet have the capability to detect changes over a short time.
The SEL method itself and its associated procedures may contribute to the limited change in SEL variables because of inaccuracy. In the SEL study of the Achilles tendon, 5 the reference tissue was (nonchangeable) fat tissue in contrast with the current study, where the reference tissue was a soft area of the deltoid muscle. In the current study, where the exercise intervention might have caused changes in the deltoid muscle, leading to increased stiffness in both regions, potential changed ratios (DELT) may have been eliminated. However, especially when scanning the supraspinatus tendon, subcutaneous fat as a reference tissue has previously been found to be difficult because this fat layer is often too thin. 4 As described, Zhang et al 39 used SWE in a follow-up study to investigate the use of SEL in the Achilles tendon, and because there are differences between SWE and SEL techniques, the studies are not directly comparable. Generally, SWE is assumed to be superior to SEL, as SWE is independent of a reference region that may change during intervention. However, the majority of US equipment does not have SWE, and most US equipment is not able to measure high-speed shear waves, which are produced in a stiff tendon.
In the current study, the additional SEL variable, the RAW value, is considered independent of a reference area, and therefore RAW could be considered the preferred SEL variable. Unfortunately, an increase in muscle stiffness in the deltoid may affect the force transduction into the deeper lying supraspinatus tendon, which may influence the RAW data provided that the applied external force is the same in baseline and follow-up measurements. Second, in SEL, RAW data are especially sensitive to the operator-applied transducer force, which is not yet measurable, and the lack of changes in RAW could therefore also be due to different applied transducer forces.
As previously described, according to physiological processes related to tendon disrepair, tendinopathy can be graded into different phases (reactive or hypertrophic, degenerative). 6 Therefore, subgrouping tendon stiffness into baseline phases of tendinopathy may have resulted in significant group differences (symptomatic vs asymptomatic tendon) in the change from baseline to follow-up measurements. A reason may be that because of the different tendinopathy phases at baseline (eg, a hypertrophic tendon will be softer [and thicker] than will a degenerative tendon because of edema), change in stiffness may also be different (eg, in hypertrophic tendons vs in degenerative tendons). Therefore, without such subgrouping, possibly with adjustment for covariates, such as sex and stiffness of the contralateral side, changes may be leveled out because of different baseline conditions. The current data showed that variations in total tendon changes of SEL at baseline were present for both the symptomatic and the asymptomatic tendons with no specific relation to the direction and size of the changes. However, because of the relatively low sample size, subgrouping according to baseline conditions was not possible, and therefore these speculations cannot be tested in the current data. To our knowledge, no longitudinal studies of the supraspinatus tendon have investigated the association between SEL and thickness of the supraspinatus tendon.
Limitations and Strengths
One of the limitations was the use of the deltoid as reference tissue because this muscle may be prone to change during training. However, when scanning the supraspinatus tendon, the choice of reference tissue was limited, which is why the RAW SEL data were also included.
Another limitation is the lack of sample size calculations, constituting an increased risk of type 2 error. However, because no previous trial has reported prospective changes using SEL in the supraspinatus tendon, this was not possible; thus, the current study design was exploratory.
Another possibility is that the patient’s pain was caused by an imbalance in the force couples rather than an actual structural change of the tendon, in which case SEL would be an inappropriate modality for evaluating improvements.
The diagnosis was based on clinical examination only and not imaging. However, the risk that the pain was not directly caused by supraspinatus tendinopathy was attenuated because of the use of MRI, US, and other clinical tests to rule out other pathological causes for the pain.
Further, because of ethical considerations, the current study did not include a control group of patients, that is, patients not receiving exercise interventions, which is a further methodological limitation. However, only patients with unilateral pain were included, which made it possible to compare data with that of the asymptomatic or healthy shoulder used as a control. A disadvantage of using the contralateral side as a control, however, is that having pain in 1 shoulder may increase the load on the opposite shoulder, thereby giving extra load stimuli to the asymptomatic shoulder. As the current patients all had long-term discomfort, the potential initial effect of increased activity in the asymptomatic shoulder is considered of limited relevance and not likely to have biased the results.
The strengths of the study are its use of reliable 4 and valid 3 SEL and PROM methods, in addition to the use of 2 different quantitative variables (ratio and RAW), not previously reported in a longitudinal study of SEL of the supraspinatus tendon. The performances of the blinded measurements using SEL, MRI scans, and US are further strengths of this study.
Perspective
In the current study, tendinopathic tendons’ response to training were diverse when measured using SEL. Future studies require large sample sizes including controlled baseline phases of tendon disrepair for investigating the response to exercise, in addition to biopsies to investigate the chemical composition of tendon healing.
Positive self-reported outcomes and improved muscle strength after training do not always seem to be matched by increased tendon stiffness, which may increase the risk of unexpected reinjury in cases of return to high-level sports too early. 26 Future studies may therefore include muscle tissue in the investigation of long-term response on tendon stiffness after training.
As mentioned, SWE is hypothesized to be more reliable and quantitative than is SEL. 30 However, SWE is not ideal for measuring stiff tendons according to the manufacturer (GE Healthcare, personal communication with application specialist in Ultrasound, Heidi Sørensen, 2018), and furthermore, the technology is primarily applied to high-end machines, making research in the musculoskeletal field and application in clinical settings even more challenging.
With increasing focus on the development of gold standards, standardized procedures, and algorithms, SEL may be useful in the future within the musculoskeletal field.
Conclusion
Despite no significant within-group or between-group changes in SEL, significant improvements were found in patient-reported outcomes. An acceptable agreement between patient changes in SEL and PROM was seen. Further studies should explore SEL’s ability to detect changes after tendon repair and long-term training, potentially in subgroups of different tendinopathy phases.
Footnotes
Acknowledgment
We thank our colleagues at the Shoulder Unit of the Orthopedic Department at Lillebaelt Hospital–University Hospital for recruiting patients and our colleagues at the Department of Radiology, Lillebaelt Hospital–University Hospital of Southern Denmark, Kolding, for providing MRI scans of the patients. We also thank Suzanne Capell for editing the manuscript.
Final revision submitted July 6, 2020; accepted August 31, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was funded by the Region of South Denmark (Research Fund and PhD-Fund), the Danish Rheumatism Association, and the Danish Council of Radiographers. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Regional Committee on Health Research Ethics for Southern Denmark (S-20160115).