
Abstract
Background:
Complete understanding of rotator cuff pathology relies on a comprehensive knowledge of the anatomic relationships between the supraspinatus tendon (ST) and the superior capsule (SC) of the glenohumeral joint. However, the native anatomy of these structures across the glenohumeral joint and at their attachment sites remains incompletely understood.
Purpose:
To (1) determine the histological anatomy and absolute and relative thicknesses of the SC compared with the ST across the glenohumeral joint at the anterior, midpoint, and posterior portions of the ST; (2) quantify the percentage of the humeral footprint occupied by the SC versus the ST; and (3) measure the width of the SC insertion on the glenoid.
Study Design:
Descriptive laboratory study.
Methods:
Fourteen right cadaveric shoulders were dissected, fixed in formalin, embedded in plastic, and sectioned into 3 sections encompassing the anterior, middle, and posterior portions of the ST. Sections were then surface-stained with toluidine blue and basic fuchsin. The SC and ST thicknesses at the medial, midpoint, and lateral aspects of the ST; the medial-lateral width of the humeral insertions of the SC and ST; and the width of the SC insertion on the glenoid were measured. Measurements at each location were compared using 1-way analysis of variance with post hoc Bonferroni corrections.
Results:
There was no statistically significant variation in the relative thickness of the SC versus the ST at the medial, midpoint, or lateral aspects of the tendon. The SC and ST were histologically distinct at their insertions on the humeral footprint. The SC comprised 15.2% to 16.2% of the total footprint width. The ST was consistently thicker at its humeral insertion than at its medial-lateral midpoint (P < .05). The anterior and posterior humeral insertions of the SC were significantly thicker than the corresponding midpoints (P = .015 anteriorly; P = .042 posteriorly). The SC was consistently thicker at its glenoid insertion than at its midpoint (P < .05).
Conclusion:
The humeral insertions of the ST and SC were generally thicker than their midpoints. The SC was also thicker at its glenoid insertion compared with its midpoint. The SC occupied approximately 15% of the width of the native rotator cuff insertion, which is smaller than previously defined.
Clinical Relevance:
By providing improved clarity on the histological differences between the SC and ST, these data may allow for a better understanding of rotator cuff pathology, particularly delaminated tears. These results suggest that, when present, the deepest 1 to 2 mm of tissue in the articular layer may represent the SC, while articular-sided layers >2 mm in thickness likely include portions of the supraspinatus musculotendinous unit. This knowledge may serve to enhance intraoperative understanding of tear anatomy, especially in cases of poor tissue quality and retraction. Furthermore, this study demonstrates that the native insertion of the SC covers the medial 15% of the tuberosity. Surgeons should be aware of this anatomic detail when attempting to repair delaminated rotator cuff tears that may involve the underlying SC.
A complete understanding of rotator cuff pathology depends on a precise knowledge of the rotator cuff insertion and intraoperative recognition of tear pattern and morphology. This is particularly important when considering delaminated tears in which the rotator cuff splits horizontally between layers, with the superior layer containing the rotator cuff tendon (most often the supraspinatus tendon [ST]) and the inferior layer containing the superior capsule (SC) of the glenohumeral joint. 12 The prevalence of delaminated rotator cuff tears has been reported to be between 38% and 92%, with incidence increasing in recent years due to an increased awareness and improved ability to recognize this pathology. 8 These tears present a challenging problem for shoulder surgeons due to the significant atrophy and retraction that may be present at the time of surgery. Successful outcomes after repair of delaminated tears depend on deliberate anatomic restoration of both layers to their native insertions on the humerus to avoid overtensioning.5,10,11 However, knowledge of the anatomic insertion sites of each layer, their respective degree of humeral footprint coverage at the enthesis, and the relative anatomy of the SC and ST as they span the glenohumeral joint remains largely unknown.
Both clinical and laboratory studies have emphasized that understanding the anatomy of the SC and ST is essential to understanding rotator cuff pathology.5,10,17 However, previous cadaveric studies investigating these relationships used macroscopic techniques or reported disrupting the native tissue architecture by detaching the tissue for measurement, rendering them prone to measurement error.1,2,7 As such, there are limited data investigating these structures using modern histological techniques and technology.
Therefore, the purpose of this investigation was to (1) determine the histological anatomy and the absolute and relative thicknesses of the SC compared with the ST across the glenohumeral joint at the anterior, midpoint, and posterior portions of the ST; (2) quantify the percentage of the humeral footprint occupied by the SC versus the ST; and (3) measure the width of the SC insertion on the glenoid. We hypothesized that the SC would be histologically distinct from the ST at the humeral footprint and would occupy a relatively smaller percentage of the footprint width.
Methods
To study the intact glenohumeral joint microscopically, undecalcified plastic-embedding histology was used. This specimen preparation method is well established for histological studies of musculoskeletal tissues. 16 Pilot testing of specimen preparation was performed to ensure proper sample positioning for sectioning and perfect protocols for embedding and staining to minimize technical error that could lead to incomplete visualization of structures of interest, poor tissue quality, or inaccurate measurement. Pilot specimens with poor-quality staining or unusable slides were not included in the final analysis.
Gross Specimen Dissection and Preparation
Institutional review board approval was not required for this investigation because we used de-identified cadaveric specimens (Science Care) that were donated for the purpose of medical research. Specimens were excluded if donor age was <18 or >50 years, there was any documented history of previous shoulder surgery or rotator cuff tearing, or there was any evidence of shoulder instability or contracture. Fourteen fresh-frozen right shoulder specimens meeting inclusion criteria were procured. This sample size was based on similar studies investigating SC anatomy.12,18 Before dissection, the frozen specimens were allowed to thaw to room temperature for at least 4 hours. Careful dissection was performed to remove all tissue from the glenohumeral joint, leaving the ST, muscle, and joint capsule undisturbed. The entirety of the ST insertion on the humeral footprint was left intact. The supraspinatus muscle belly was transected medial to the glenoid. The capsule was similarly left intact across the entire glenohumeral joint. An oscillating bone saw was then used to remove the coracoid process and to transect the scapula in the sagittal plane 2 cm medial to the insertion of the SC on the glenoid. The humerus was transected 2 cm below the level of the inferior capsule insertion in the axial plane. Specimens were then pinned in anatomic position based on the native articulation of the humeral head and glenoid using 2 Kirschner wires.
Histological Specimen Preparation and Measurement
After pinning, specimens were fixed in 10% neutral buffered formalin. Pin orientation was verified by contact radiography (Hewlett-Packard Faxitron Cabinet X-ray System). Using a custom water-cooled cutoff saw with a diamond-impregnated blade, the specimens were sectioned along a plane parallel to the ST into 1-cm slabs. Contact radiographs of the slabs were obtained to select the slabs that contained intact humerus, glenoid, and tendon for histology. These slabs were processed for undecalcified plastic embedding in polymethyl methacrylate. After polymerization, the embedded slabs were serially sectioned into slides containing the anterior, middle, and posterior portions of the ST and SC, each including the complete humeral footprint and the capsular attachment to the glenoid. The sections were ground to approximately 250 µm in thickness and surface-stained with basic fuchsin and toluidine blue.
From the stained sections, the ST and SC were identified using a digital microscope (Keyence VHX-6000) at a magnification of 20×. The VHX-6000 provides for high-resolution digital imaging with a 1.95-million pixel complementary metal oxide semiconductor image sensor. Its baseline resolution is 1600 × 1200 total pixels. Large-area image observation at high magnification is possible with an image stitching algorithm that can synchronize positional information from the motorized XY stage to automatically move and stitch together adjacent images measuring up to 20,000 × 20,000 pixels.
The thicknesses of the ST and the SC were measured at the medial, midpoint, and lateral aspects of the ST using the measurement tools incorporated in the digital microscope software. The thicknesses of the ST and SC were measured perpendicular to the long axis of the tendon and capsule, respectively (Figures 1 and 2). The total medial-lateral width of the humeral footprint (Figure 3B), the width of the SC insertion on the footprint (Figure 3B), and the width of the SC insertion on the glenoid (Figure 4) were also measured. The width of the ST insertion was calculated to be the difference between the total footprint width and the width of the SC. All measurements were performed by 2 reviewers: 1 orthopaedic surgeon and 1 scientist (N.M., D.J.H.) with expertise in histological analysis. Any measurement discrepancy >0.5 mm would have been further evaluated by a third reviewer, (D.M.K.) although no such discrepancies were appreciated.

Toluidine blue and basic fuchsin staining of a representative section showing the humeral head, glenoid, supraspinatus tendon (ST) (*), and superior capsule (SC) (★), as well as the division between the SC and ST (red line). The brackets represent the humeral insertion of the ST and SC and the glenoid attachment of the SC. Individual red lines demarcate the locations and orientations at which the thicknesses of the ST and SC were measured. Digitally stitched image; original magnification, 20×.

(A) Magnified (100×) image of the supraspinatus tendon (ST), superior capsule (SC), and humeral head articular cartilage. (B) Representative measurements of the ST (3.71 mm) and SC (2.16 mm) at the midpoint of the ST at its anterior aspect. Magnification, 20×.

(A) Representative sections of the humeral footprint showing the histologically distinct insertions of the superior capsule (SC) and supraspinatus tendon (ST). Magnification, 50×. (B) Representative measurements of the total humeral footprint width (17.45 mm) and width of the SC insertion (3.22 mm). The width of the ST insertion was calculated to be the difference between the total footprint width and the width of the SC (14.23 mm). Magnification, 20×.

Representative section demonstrating the histologically distinct superior capsule (SC) (*) from the superior labrum (L) at the glenoid (G) insertion. Also shown is a representative measurement of the width of the SC insertion (3.95 mm). SS represents the supraspinatus muscle belly overlying the SC. Magnification, 20×.
Statistical Analysis
Descriptive statistics for all continuous variables are reported as mean and standard deviation. Data were assessed for normality using a Shapiro-Wilk test. Statistical comparisons were made using 1-way analysis of variance with post hoc Bonferroni corrections, and paired t tests where appropriate. The threshold for statistical significance for all analyses was set at α ≤ .05. Statistical analysis was performed using SPSS (Version 26, IBM Corp).
Results
ST and SC Thicknesses
A representative section displaying the humeral head, glenoid, ST, and SC is shown in Figure 1. The ST and SC were identified as histologically distinct structures (Figure 2).
The absolute and relative thicknesses of the SC and ST at measured locations along the length of the ST are shown in Table 1. There was no statistically significant variation in the absolute or relative thickness of the SC or ST at the medial, midpoint, or lateral aspects of the ST. The mean absolute thickness of the SC ranged from 0.89 ± 0.37 mm (located at the lateral aspect of the ST, at the middle of the tendon from anterior to posterior) to 1.40 ± 0.76 mm (located at the midpoint of the ST, at the middle of the tendon from anterior to posterior). The mean absolute thickness of the ST ranged from 2.83 ± 0.85 mm (located at the posterolateral aspect of the ST) to 3.39 ± 1.54 mm (located at the central aspect of the tendon). The maximum thickness of the SC at the midpoint of the ST was 2.99 mm, located in the middle of the tendon from anterior to posterior.
Absolute and Relative Thicknesses of the SC and ST at Various Locations Along the ST a
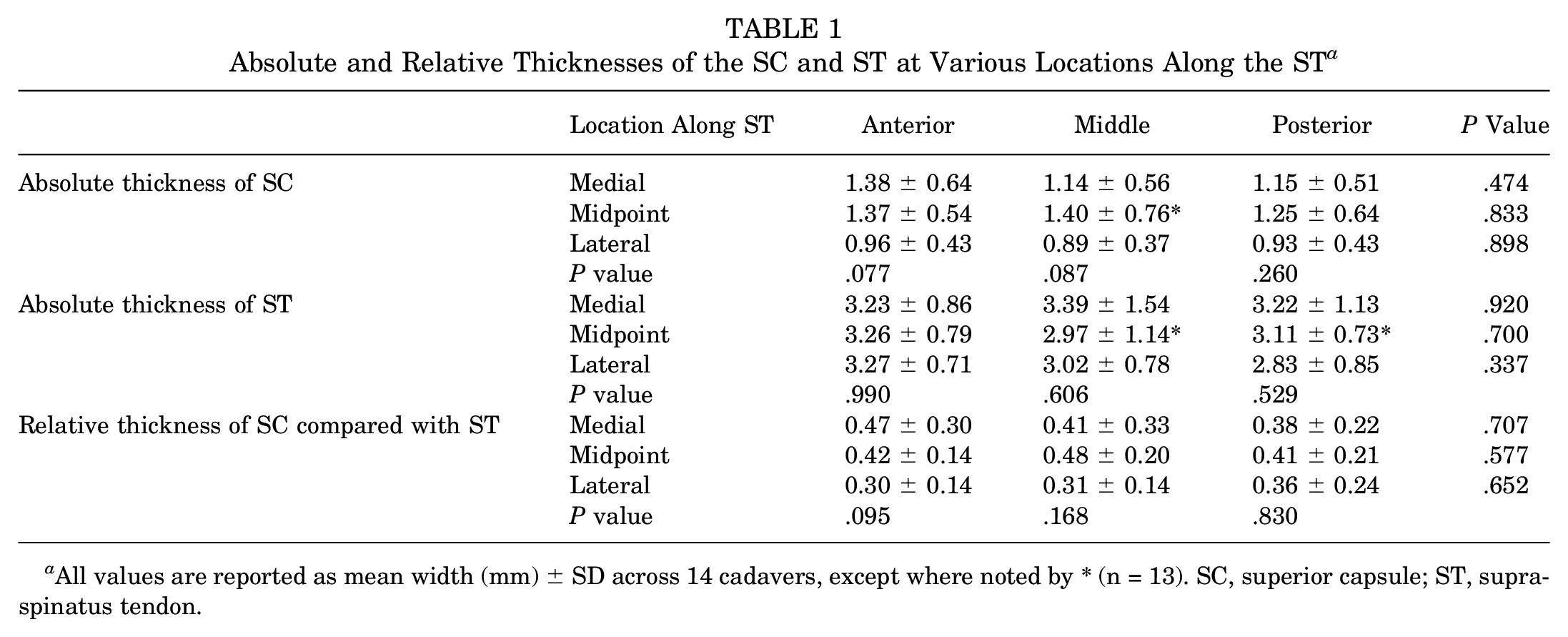
All values are reported as mean width (mm) ± SD across 14 cadavers, except where noted by * (n = 13). SC, superior capsule; ST, supraspinatus tendon.
Anatomy at the Humeral Footprint and Glenoid
The insertions of the SC and ST at the humeral footprint also demonstrated a consistent pattern across all specimens. The SC and ST were histologically distinct with separate attachment points on the humerus (Figure 3). The SC attached just lateral to the articular margin, while the ST insertion occupied the remainder of the medial-lateral width of the footprint. The fibers of the SC and ST remained relatively parallel as they coursed toward their humeral attachment site, increasing in thickness at their humeral attachment. The fibers of the SC and ST inserted relatively perpendicular to the bone; however, at the footprint, the superior-most fibers of the ST diverged to attach along the most lateral aspect of the footprint (Figure 3B).
Similarly, the SC remained histologically distinct from the superior labrum on the glenoid (Figure 4). The morphology of the glenoid attachment of the SC was consistent across all specimens. The fibers of the SC mirrored the contour of the superior labrum near their insertion onto the glenoid. The SC fibers lay on top of the superior labrum at the level of the labral attachment to the glenoid and continued medially beyond the labral attachment to insert onto the glenoid. In contrast to their humeral attachment, the fibers of the SC attached to the glenoid in an oblique orientation (Figure 4).
The total width of the humeral footprint and the width of the SC at its insertion on the humeral footprint were not significantly different from anterior to posterior (Table 2). The SC comprised between 15.2% and 16.2% of the total width of the humeral footprint. The width of the SC insertion on the glenoid was not significantly different at the anterior (3.34 ± 0.78 mm) or posterior (3.12 ± 1.24 mm) aspects of the ST (P = .871).
SC and ST Widths at the Humeral Footprint and Width of the SC at Its Glenoid Insertion a

All values are reported as mean width (mm) ± SD. SC, superior capsule; ST, supraspinatus tendon.
On average, the width of the ST insertion on the humerus was significantly greater than the tendon thickness at its medial-lateral midpoint anteriorly, at the middle of the tendon, and posteriorly (P < .001 for all). The thickness of the humeral insertion of the SC was also significantly greater than the corresponding midpoint thickness anteriorly (P = .015) and posteriorly (P = .042), while there was no significant difference at the level of the middle of the tendon (P = .053).
The width of the SC insertion at the glenoid was significantly greater than the corresponding medial-lateral midpoint thickness anteriorly (P < .001), at the middle of the ST (P = .001), and posteriorly (P = .006) (Tables 1 and 2).
Discussion
This study defined the native anatomy of the SC and ST at the level of the glenohumeral joint using robust histological analyses. We observed that the SC and the ST are histologically distinct structures at their attachments on the humeral footprint with no variation in the absolute or relative thickness as they span the glenohumeral joint before attaching onto the humerus. The SC and ST were generally thicker at their humeral attachments than at their medial-lateral midpoints. Similarly, the SC was thicker at its glenoid insertion than at its midpoint.
Furthermore, the SC occupied a relatively small, although consistent, proportion of the humeral footprint width. The maximum SC thickness at the midpoint of the ST was 2.99 mm. Overall, these results supported our hypothesis and may provide clinical benefit in improving the understanding and treatment of rotator cuff pathology.
Few previous studies have investigated the native anatomy of the SC and ST at the glenohumeral joint at the microscopic level.1,2,7,13 In a cadaveric investigation, Itoi et al 7 reported the thickness of the SC to be 1.6 ± 0.4 mm. Bigliani et al 1 evaluated the thickness of the inferior glenohumeral ligament complex in the context of its biomechanical properties, but did not evaluate anatomic trends of the SC as it spanned from the glenoid to the humerus. Ciccone et al 2 measured glenohumeral capsule thickness in 8 cadavers after releasing the capsule from its humeral attachment, sectioning the capsule into quadrants, and measuring the detached capsule thickness under a microscope. The authors observed that the capsule thickness ranged from 1.32 to 4.47mm, with the capsule thinning significantly laterally from the glenoid (mean thickness, 3.03 ± 1.22 mm) to the humeral insertion (mean thickness, 2.17 ± 1.30 mm) (P < .05). In our investigation, we appreciated a trend with the SC decreasing in thickness from medial to lateral (before attaching to the humerus), although this was not statistically significant. Furthermore, the thickness measurements reported in our study are smaller than those reported by Ciccone et al. 2 These differences are likely reflective of our ability to distinguish these distinct structures histologically under high-power and high-resolution magnification without disrupting the native architecture, allowing for more precise measurements. Other studies have reported incomplete visualization of tissues after sectioning or used imprecise macroscopic measurement techniques.2,12
We found that the SC insertion occupied between 15.2% and 16.2% of the total width of the humeral footprint. In their macroscopic analysis of 13 cadaveric shoulders, Yuri et al 18 reported that the SC insertion occupied approximately one-third of the humeral footprint, with the remaining two-thirds being occupied by the rotator cuff. In the 3 specimens that were examined histologically, the SC and ST were observed to be histologically distinct and demonstrated firm attachments at the footprint. Meanwhile, Nimura et al 12 used gross tissue measurement techniques to quantify the relationship of the SC and ST attachments on the humeral footprint in 12 cadavers fixed in formalin. The authors reported that the mean width of the SC insertion was greater at the anterior margin of the greater tuberosity than at the posterior margin of the ST (5.6 ± 1.6 mm vs 4.4 ± 1.2 mm), although statistical analyses were not performed. Based on their measurements of the ST at the same location, the SC represented 37% to 62% of the total footprint. 12 The differences between previous findings and those reported in the present study may once again be attributed to differences in methodology. Namely, by preserving the native tissue architecture, using tissue-specific staining, and using high-resolution digital microscopy at 20× magnification, our investigation was able to isolate the SC and ST tissues histologically to obtain precise measurements of their separate insertions.
The medial-lateral widths of the SC (2.21-2.35 mm) and ST (11.90-12.32 mm) insertions at their humeral attachment were relatively consistent from anterior to posterior. Ruotolo et al 15 (11.6-12.1 mm) and Dugas et al 4 (mean 14.7 ± 3.2 mm) reported similar measurements of the medial-lateral ST insertion width from anterior to posterior. Using gross tissue measurement in cadavers, Mochizuki et al 9 reported that the width of the SC at the posterior edge of the ST footprint was 4.5 ± 0.5 mm. Our results indicate that when histologically isolated, the thickness of the SC at the humeral footprint is smaller than previously described.
By providing improved clarity on the histological differences between the SC and ST, these data may allow for a better understanding of rotator cuff pathology, particularly delaminated tears. Clark and Harryman 3 defined 5 separate histological layers of the rotator cuff insertion at the humeral head, including a 1.5- to 2-mm fibrous capsular layer. While the authors noted that the precise location of delamination can be variable, the deep layer was thought to contain the SC.3,8,9,17 Our results suggest that, when present, the deepest 1 to 2 mm of tissue in the articular layer may represent the SC, while articular-sided layers >2 mm in thickness likely include portions of the supraspinatus musculotendinous unit. This knowledge may serve to enhance intraoperative understanding of tear anatomy, especially in cases of poor tissue quality and retraction. Furthermore, our study demonstrates that the native insertion of the SC covers the medial 15% of the tuberosity. Surgeons should be aware of this anatomic detail when attempting to repair delaminated rotator cuff tears that may involve the underlying SC. This may have implications in restoring shoulder stability, as biomechanical studies have reported that a defect in the SC in the setting of rotator cuff tears increases glenohumeral translation in all directions, particularly in the anterior-posterior direction.6,14
Limitations
Inherent limitations in specimen preparation were encountered, including the presence of preexisting tissue damage, staining quality, and variability in the axis of sectioning that may have confounded measurement standardization. This variability was minimized by performing extensive pilot testing to ensure that the preparation process was reproducible and robust. Regardless, not all measurements were able to be performed in all specimens, as noted in Tables 1 and 2. In 1 specimen, the staining partially obscured the midpoint measurement location of the SC and ST. Other sections inadvertently cut off the humeral footprint or glenoid attachment of the SC, precluding measurement of these structures. As cadaveric specimens with any evidence or reported history of shoulder pathology were excluded, our measurements represent the normal state and may not be generalizable to individuals with tissue degradation or hypertrophy, which may occur in the setting of chronic rotator cuff disease. Furthermore, specimen sex and mean age were not provided by the supplier. Although a power analysis was not conducted, the sample size of this study is comparable to those of other similar studies in the literature.12,18 Finally, our measurements do not reflect the complex 3-dimensional anatomy of the humeral or glenoid attachment sites of the SC and SC, nor do they provide insight into the biomechanical function of each layer.
Conclusion
The SC and ST were generally thicker at their humeral attachments than at their medial-lateral midpoints. The SC was consistently thicker at its glenoid insertion than at its midpoint. The SC represents approximately 15% of the width of the native rotator cuff insertion, which is smaller than previously defined. These results are relevant in understanding and treating delaminated rotator cuff tears and in other procedures that aim to restore glenohumeral anatomy.
Footnotes
Acknowledgements
The authors thank Jennifer Wright and Mabel Ye for their work on this project.
Final revision submitted November 25, 2024; accepted January 3, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: D.M.K. has received support for education from Smith & Nephew, Elite Orthopaedics, and Medwest Associates; personal fees from DJ Orthopaedics; and a grant from Arthrex. G.E.G. has received consulting fees from Bioventus, Tornier, Mitek, and DJ Orthopaedics; royalties from Tornier and DJ Orthopaedics; other financial support from Arthrex, Zimmer, and SouthTech; and holds stock in Genesys and ROM3. N.N.V. has received consulting fees from Minivasive and Orthospace; research support from Arthrex, Breg, Ossur, Smith & Nephew, and Wright Medical Technology; royalties from Smith & Nephew and Vindico Medical–Orthopedics Hyperguide; and holds stock in Cymedica, Minivasive, and Omeros. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.