
Abstract
Background:
Coracoacromial ligament (CAL) degeneration is thought to be a factor in external impingement in bursal-sided rotator cuff tears, but CAL release is associated with adverse effects.
Purpose:
To investigate the association between CAL degeneration and the patterns of massive rotator cuff tears using multiple modalities and to assess the effect of CAL degeneration on supraspinatus tendon retear rates.
Study Design:
Cohort study; Level of evidence, 2.
Methods:
The authors prospectively recruited 44 patients who had undergone arthroscopic rotator cuff repair without acromioplasty or CAL release. Preoperative radiographs and magnetic resonance imaging (MRI) scans were reviewed to determine acromial morphology and CAL thickness, respectively. Rotator cuff tears were categorized as isolated supraspinatus or massive (involvement of ≥2 tendons), with massive tears categorized using the Collin classification. Acromial degeneration was analyzed using the Copeland-Levy classification. The CAL was biopsied intraoperatively and histologically analyzed using the Bonar score. At 6-month follow-up, the integrity of the repaired supraspinatus tendon was analyzed on MRI using the Sugaya classification. Finally, the associations among CAL degeneration, rotator cuff tear pattern, and arthroscopic grading were investigated.
Results:
Patients with Collin type B rotator cuff tear had significantly higher CAL Bonar scores than those with Collin type A or isolated supraspinatus tears (10.0 vs 6.8 and 3.4; P = .03 and P < .001, respectively). Patients with a degenerative acromial undersurface of Copeland-Levy stage 2 or 3 had CALs with significantly higher Bonar scores than those with an intact acromial undersurface (8.4 and 8.2 vs 3.5; P = .034 and P = .027, respectively). The CAL Bonar scores of patients with different stages of the 6-month postoperative Sugaya classification were comparable (6.5, 7.2, 8.0, and 7.8 for stages 1, 2, 3, and 4, respectively; P = .751).
Conclusion:
CAL degeneration was more severe in anterosuperior-type massive rotator cuff tears. Interestingly, even without acromioplasty, the severity of CAL degeneration did not affect the retear rate of the supraspinatus tendon.
The coracoacromial ligament (CAL) extends from the coracoid process of the scapula to the anterior edge of the acromial undersurface, 21,30 constituting an osseoligamentous restraint to anterosuperior displacement of the humeral head. 5,12,23,27 Many biomechanical studies have shown that CAL release results in increased anterior and superior glenohumeral translation, underscoring the stabilizing role of the CAL. 6,11,18,22,23,32,37,39 A growing number of clinical studies also suggest that sacrificing CAL could lead to shoulder instability, calling into question the benefits of acromioplasty. 3,18,28 Nevertheless, some advocates of acromioplasty regard CAL ossification as a predisposing factor for external impingement syndrome in rotator cuff and still perform acromioplasty or CAL release during bursal-sided rotator cuff tear repair. 17,24,29 While the role of CAL degeneration in partial cuff tear remains controversial, there is a paucity of studies on the association between CAL degeneration and retear rate after repair of massive rotator cuff tears.
With advancements in imaging techniques, CAL can be visualized using multiple modalities. CAL presents as hypointensity on T1-weighted magnetic resonance imaging (MRI); some authors suggest that a thickened CAL on an MRI scan is associated with shoulder impingements, 8,9,31 while others report that reduced CAL thickness at the acromial undersurface is associated with increased rotator cuff tear size. 20,21 The Copeland-Levy classification, an arthroscopic classification for evaluation of subacromial impingement (Appendix Table A1), has been corroborated for its reliability. 1,21 An advanced Copeland-Levy stage is associated with degenerative-type rotator cuff tears (rather than traumatic-type rotator cuff tears) as well as an increased cuff tear size. 21,33 Shibata et al 33 evaluated the histology of the CAL and concluded that compared with traumatic tears, degenerative rotator cuff tears were associated with more severe CAL degeneration.
In this study, we aimed to investigate the association between CAL degeneration and massive rotator cuff tear patterns. We also evaluated the interrelationships of microscopic ratings, arthroscopic grading, and radiographic findings of CAL. We hypothesized that CAL degeneration patterns differ according to the subtype of massive rotator cuff tear and that CAL degeneration is associated with retear rate in specific rotator cuff tear patterns. We also hypothesized that a positive correlation exists among the radiographic, arthroscopic, and microscopic grades of CAL degeneration.
Methods
Population
We prospectively recruited 44 patients who underwent arthroscopic repair of chronic degenerative rotator cuff at a tertiary referral center between January 2021 and June 2021. Patients who had undergone previous shoulder surgery (n = 1) or had a concomitant frozen shoulder were excluded (n = 1). Three patients were excluded because of incomplete radiographic studies or suboptimal MRI quality. Ultimately, 39 patients (19 men and 20 women; mean age, 60.1 ± 9.07 years) were included in the study. The study protocol received institutional review board approval, and written informed consent was obtained from all study participants.
Preoperative Imaging Analysis
All patients underwent preoperative radiography and MRI. Radiographic analysis was independently performed by a senior sports medicine specialist (K.-L.H.) who was not involved in caring for the recruited patients. Complete radiographic examinations included anteroposterior views of the shoulder in internal and external rotation, the Grashey view (true anteroposterior view of the scapula), and the shoulder outlet view.
Parameters related to the subacromial impingement syndrome were assessed. In the Grashey view, critical shoulder angle (CSA), acromiohumeral distance (AHD), lateral acromial angle (LAA), and acromial index (AI) were calculated. In the lateral scapular view, the slope of acromion was quantified by measuring the acromial tilt (AT) 2 (Appendix Figure A1).
In the T1-weighted paracoronal view of the MRI scans, the CAL was defined as the region of hypointensity at the acromion undersurface, and its thickness was measured at the lateral margin of its acromial insertion as previously described 15,20 (Figure 1A).
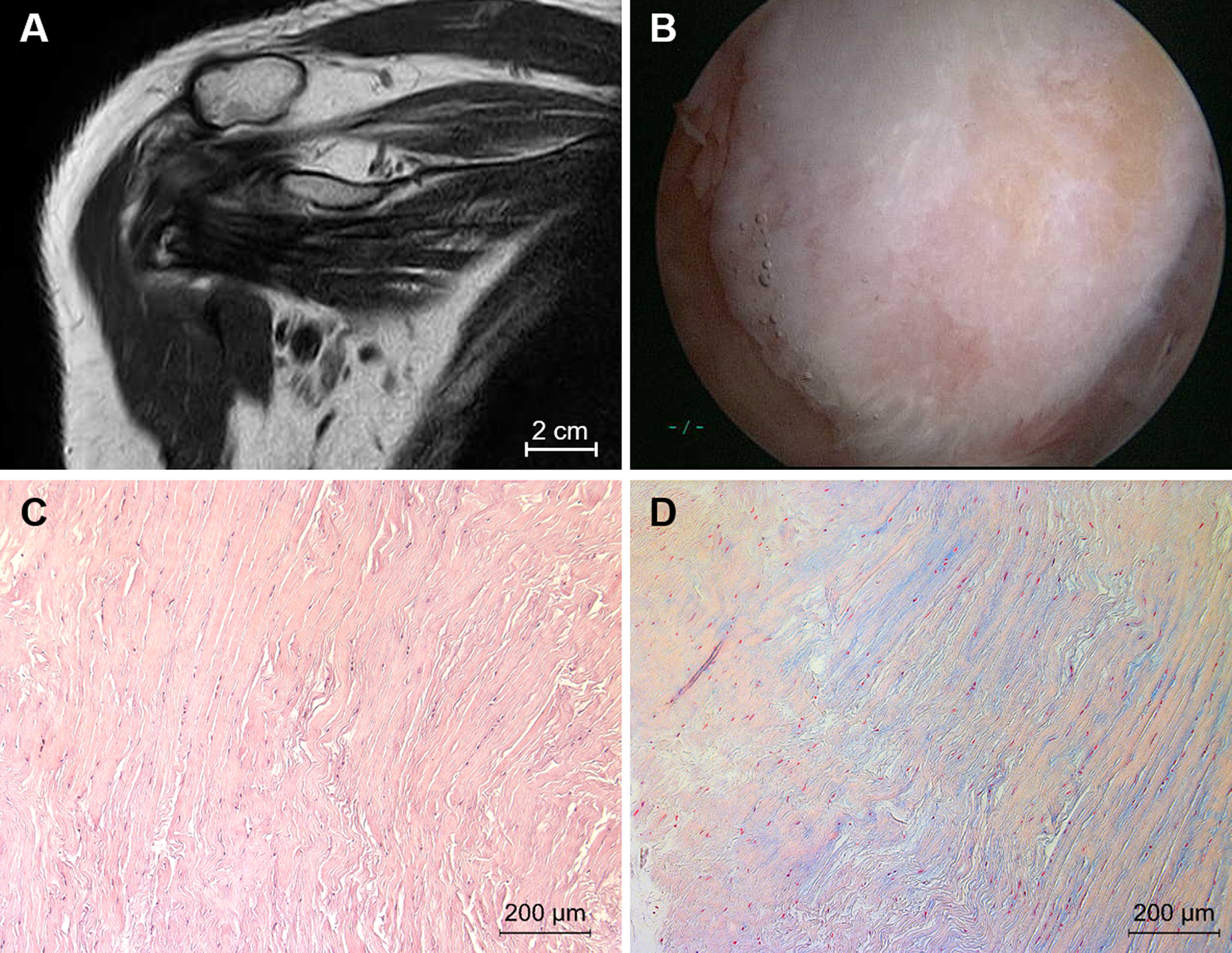
Images of a 68-year-old woman with anterosuperior-type (Collin type B) massive rotator cuff tear. (A) The thickness of the coracoacromial ligament (CAL) is measured on coronal T1-weighted magnetic resonance imaging. (B) During arthroscopic surgery, scuffing of the acromial undersurface is visible and graded stage 2 on the Copeland-Levy classification. (C) Hematoxylin and eosin and (D) Alcian blue staining of the harvested CAL. Cell morphology: increased roundness and small amount of cytoplasm, 2; collagen alignment: separation of individual fiber bundles, 1; cellularity: hypercellularity, 1; vascularity: areas of several clusters of vessels, 2; ground substance: abundant glycosaminoglycans throughout the section, 3; total Bonar score, 9.
Arthroscopic Evaluation
All arthroscopic repairs were performed by the same surgeon (W.-R.S.). Each patient underwent surgery in the lateral decubitus position, with the affected limb abducted at 30° and flexed at 15°, under an axial traction of 3 to 5 kg. The acromial undersurface was visualized via the posterior portal and graded using the Copeland-Levy classification (Appendix Table A1). 1,21 CAL specimens were aseptically collected during surgery. The lateral band of the CAL was biopsied at the lateral-most point of acromial insertion, where enthesophyte formation and degeneration were observed in past studies 12,36 (Figure 1B), and rotator cuff pathology was evaluated during surgery. The CAL was not debrided or released, and acromioplasty was not performed in our cohort. Massive rotator cuff tears, defined as tears involving 2 or more tendons, were assessed using the Collin classification 7 (Appendix Table A1).
Histologic Analysis
Biopsied CAL specimens were fixed in 4% neutral formalin and embedded in paraffin for subsequent histological analysis. Three consecutive longitudinal sections (4 µm thick) were cut on a microtome and stained with hematoxylin and eosin (H&E), Masson trichrome, and Alcian blue. Degenerative changes in the CAL were semiquantified from 0 to 15 points using the updated Bonar score by Fearon et al 13,19 (Appendix Table A1). H&E staining was used to evaluate the cell morphology, cellularity, collagen alignment, and vascularity. Alcian blue was used to determine the stainable mucin content of the ground substance. Histological analyses were independently performed by an investigator (F.-C.K.) on 1 to 10 randomly selected high-power fields (40×) of each sample (Figure 1, C and D).
Integrity of Repair
Patients underwent MRI 6 months after the index surgery. The MRI scans were assessed for the supraspinatus tendon state according to the Sugaya classification 38 (Appendix Table A1). The integrity of the tendon was evaluated by board-certified musculoskeletal radiologists at our institution who were blinded to the clinical outcomes of the patients.
Statistical Analysis
The Kruskal-Wallis test was used to analyze continuous variables (including age, radiographic parameters, CAL thickness on MRI, and Bonar score) among patients with different rotator cuff tear patterns (according to Collin classification), levels of subacromial impingement (according to Copeland-Levy classification), and degrees of supraspinatus retear (according to Sugaya classification). The distribution of categorical variables among the patients was analyzed using chi-square analysis. Correlations among continuous variables, such as age, Bonar score, and radiographic parameters, were analyzed using the Spearman correlation coefficient (r). The threshold for statistical significance was set at P < .05. All statistical analyses were performed using the SPSS software (Version 17.0; IBM).
Results
Patient Characteristis and Radiographic Parameters
There were no statistically significant differences in the distribution of age and sex among the 39 patients included in this study. In patients with Collin type D rotator cuff tear (posterosuperior cuff tear), the CSA was significantly greater, the AHD was shorter, and the LAA was smaller than those in patients with Collin type A rotator cuff tears. The AI and thickness of the CAL were not significantly different among the patients with different types of rotator cuff tear (Table 1, Appendix Figure A2). None of our patients developed anterosuperior escape of the humeral head during follow-up.
Patient Characteristics According to Rotator Cuff Tear Pattern a
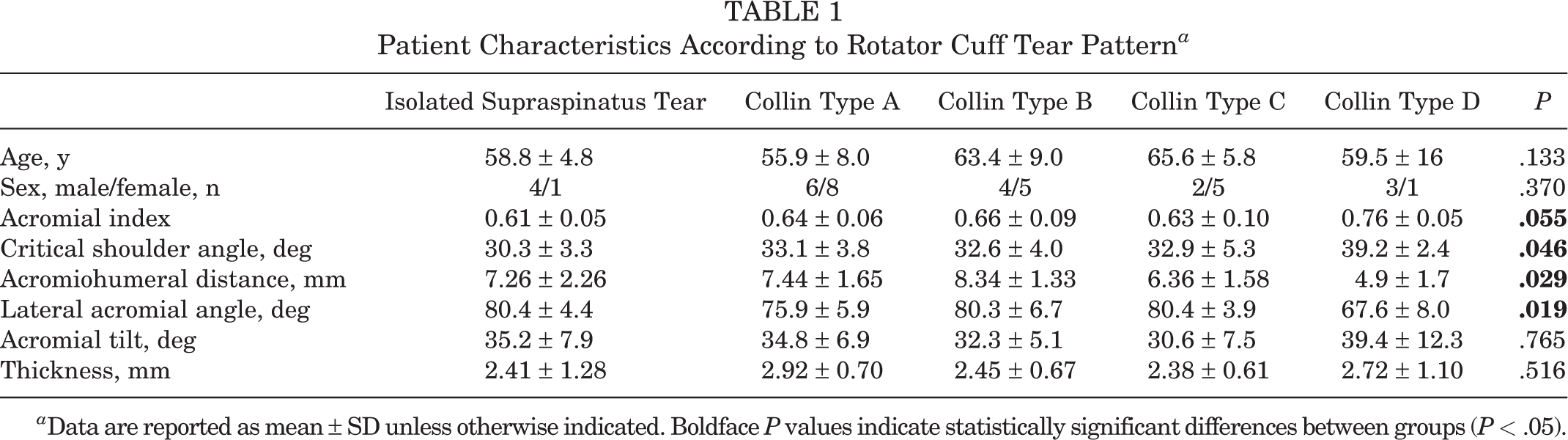
a Data are reported as mean ± SD unless otherwise indicated. Boldface P values indicate statistically significant differences between groups (P < .05).
Factors Associated With CAL Degeneration
There was a weak positive correlation between age and Bonar score (r = 0.359, P = .025) (Figure 2A). Patients with Collin type B rotator cuff tears had significantly higher Bonar scores than those with Collin type A or isolated supraspinatus tears (10.0 vs 6.8 and 3.4; P = .03 and P < .001, respectively), indicating that CAL degeneration was more advanced in anterosuperior-type massive cuff tears than in single-tendon tears (Figure 2B). No statistically significant association was found between the Bonar score and radiographic parameters, including AI, CSA, AHD, LAA, and AT (Appendix Figure A3). CAL thickness measured on coronal MRI scans had no statistically significant association with Bonar score (r = –0.198; P = .228) (Figure 2C).
Patients with acromial lesions of Copeland-Levy stage 2 or 3 had CALs with significantly higher Bonar scores than those with intact acromial undersurfaces (8.4 and 8.2 vs 3.5; P = .034 and P = .027, respectively) (Figure 2D), indicating that the Copeland-Levy staging system, an arthroscopic system of grading gross degeneration at the coracoacromial arch, had pathologic implications and that the stages corresponded to progressive histological CAL deterioration.

Factors associated with coracoacromial ligament (CAL) degeneration. (A) There was a weak positive correlation between patient age and Bonar score (r = 0.359; P = .025). (B) The Bonar score was significantly higher for Collin type B rotator cuff tear (anterosuperior-type massive rotator cuff tears) compared with Collin type A and with isolated supraspinatus tears. (C) CAL thickness measured on coronal magnetic resonance imaging scans was not statistically significantly associated with Bonar score (r = –0.198; P = .228). (D) The Bonar score was significantly higher in those with Copeland-Levy grade 2 or 3 acromial lesions than in those with intact acromial undersurfaces (grade 0). *P < .05, ***P < .001. A-D, Collin type A-D tear; S, isolated supraspinatus tear. In panels B and D, the center line indicates the median, the box indicates the interquartile range, and the error bars indicate the full range.
Supraspinatus Retear and CAL Degeneration
Of the 39 patients, 36 underwent follow-up MRI at 6 months postoperatively. The difference in Bonar scores among patients with different Sugaya grades did not reach statistical significance (6.5, 7.2, 8.0, and 7.8 for stages 1, 2, 3, and 4, respectively; P = .751) (Figure 3). The Copeland-Levy stage of the acromial undersurface was not significantly associated with the Sugaya classification of repaired supraspinatus tendon (P = .491) (Table 2). The Sugaya grade was not significantly different among patients with different types of rotator cuff tear (P = .725) (Table 2). These results imply that neither the microscopic nor the macroscopic degeneration of the coracoacromial arch affected the integrity of rotator cuff repair at 6 months postoperatively.

Coracoacromial ligament degeneration and supraspinatus tendon retear. The Bonar score was not significantly different among patients with different degrees of supraspinatus tendon repair as categorized according to the Sugaya classification. The center line indicates the median, the box indicates the interquartile range, and the error bars indicate the full range.
Relationship of Degree of Supraspinatus Retear to Subacromial Impingement Level and Rotator Cuff Tear Pattern

Discussion
The most important finding of the present study was that CAL degeneration was more advanced in anterosuperior-type massive rotator cuff tears but irrelevant to the retear rate after rotator cuff repair. Regarding the tools for evaluating CAL, increments in CAL degeneration were reflected by the advance in arthroscopic Copeland-Levy classification but not by changes in radiographic parameters or CAL thickness on MRI scans. Our results suggest that the incidence of CAL degeneration depends on the pattern of massive rotator cuff tear. The irrelevance of CAL degeneration to the retear rate suggested that CAL release may not affect retear rates. These findings provide insight into the pathogenesis of CAL degeneration and validate the effectiveness of the modalities for CAL evaluation.
The surgical indications for acromioplasty and CAL release remain controversial. CAL was first reported by Neer 24 to cause external impingement of the rotator cuff, and this observation was recapitulated by many advocates of acromioplasty. 16,17,26,29 In partial rotator cuff tears located on the bursal side, Kanatli et al 16 advised surgeons to perform CAL release and acromioplasty when grade 1 or 2 CAL degeneration was present. Our results concurred with these statements by showing that CAL degeneration was dependent on the location of the rotator cuff tear. CAL degeneration was most severe in anterosuperior-type massive rotator cuff tears (Collin type B) than in isolated supraspinatus and Collin type A tears. Although previous studies have recommended releasing degenerative CAL under such circumstances, the retear rate was not associated with CAL degeneration in our cohort.
In this study, the postoperative Sugaya classification of the supraspinatus tendon at 6 months was independent of the Bonar score of the CAL. We hypothesize that this observation implies that CAL degeneration occurs secondary to rotator cuff tear. Without a functional inferior subscapularis, the humeral head escapes anteriorly, impinging against the coracoacromial arch repetitively and causing psuedoparalysis of the shoulder. 10,40 However, it must be noted that the temporal sequence of rotator cuff tear and CAL degeneration cannot be clarified without a carefully designed longitudinal study. Before clarifying their sequence, we recommend a more cautious approach regarding CAL release and acromioplasty. The efficacy and safety of CAL release and acromioplasty in rotator cuff tears have been questioned. 5,11,18,28,37,39 In summary, CAL degeneration is correlated with the pattern and location of rotator cuff tears. However, the optimal indication for CAL release remains unclear.
Rotator cuff tears and coracoacromial arch morphology have been evaluated simultaneously using various modalities, and their association has been investigated in many previous studies. The thinner the CAL measured on MRI, the larger the rotator cuff tear size, ranging from 3.02 mm in small tears (<1 cm) to 1.87 mm in large tears (>3 cm). 20 An arthroscopic grading system of the acromial undersurface—the Copeland-Levy classification—also exists. 1,21 Worsening damage to the coracoacromial arch on the Copeland-Levy scale is reportedly associated with increasing cuff tear size. 1,21 Microscopic examinations of the CAL found that bursal-sided and degenerative rotator cuff tears were associated with fissuring and fibrillation at the fibrous and fibrocarfilaginous layers of the CAL. 26,33 The present study broadens the horizon by quantitatively evaluating the CAL (using established pathologic scores) and exploring its association with retear rate. Our results verified that age contributed to CAL degeneration, consistent with the findings of Panni et al. 26 Interestingly, only a weak association existed between age and Bonar score, implying the existence of more important factors.
Our findings also contribute to an understanding of the progressive pathogenesis and possible sequelae of the different patterns of massive rotator cuff tears, showing that anterosuperior rotator cuff tears result in more attrition of CAL. Designating pathologic scores to the Copeland-Levy classification of CAL also contributes to surgical treatment strategies. The findings also raised questions about the conclusions regarding clinical significance of CAL thickness on MRI reached in some studies. 20 While previous conclusions on CAL thickness have been conflicting, we found that the Bonar score of the CAL was not correlated with the thickness measured on MRI scans. This suggests that the quality rather than the quantity of CAL is more relevant to the incidence of rotator cuff tears. In summary, our results suggested that arthroscopic grading of acromial lesions correlates well with CAL degeneration. The results also granted arthroscopic grading of the coracoacromial arch with pathologic contexts.
The current study also investigated the associations among radiographic parameters, patterns of rotator cuff tears, and degree of CAL degeneration. CSA is a well-known radiographic parameter associated with rotator cuff tears; a large CSA is associated with posterosuperior-type cuff tear and a small CSA with glenohumeral osteoarthritis. 25,34,35 The acromial morphology has also been intensively studied, with a low LAA and a large AI associated with a higher prevalence of impingement and rotator cuff tears. In patients with rotator cuff tears, an AT >43° and an LAA <70° could exist. 4,15 Our findings corroborated the observations in previous literature, showing that patients with Collin type D (posterosuperior-type tear) rotator cuff tears had a greater CSA, smaller AHD, and smaller LAA than their Collin type A rotator cuff tear (anterosuperior-type tear) counterparts. Nevertheless, radiographic parameters did not correlate with the Bonar score for CAL degeneration, suggesting that CAL degeneration occurred secondary to anterosuperior-type rotator cuff tears. This phenomenon implies that instability of the humeral head after rotator cuff tear (rather than bony acromial structures) causes chronic attrition of CAL.
Limitations
The present study has several limitations. First, the evaluation of CAL was limited to anatomic pathological studies. The underlying molecular mechanisms and signaling transduction pathways were not elucidated. Also, the Bonar score has not been validated for ligaments. Second, the imaging modalities used—radiography and MRI—were primarily static. The effect of bony morphology (AHD, LAA, etc) on retear rates was not examined either. Additionally, only a single observer made measurements and classifications in the current study. We plan to include dynamic modalities such as sonography and test reliability in future studies. Third, the current results provide indirect evidence to support the sequence of CAL degeneration and rotator cuff involvement. Further research with longer follow-up periods is needed in order to provide more evidence and make recommendations regarding the surgical indications of acromioplasty. Fourth, the retear rate of repaired subscapularis tendon was not evaluated in the current study because of the lack of a reliable classification system. 14 Fifth, the numbers in each group were small so the possibility of type I error was fairly high. We did not include the group of patients that underwent CAL release or acromioplasty as well. Finally, this study reports the short-term retear rate of rotator cuff repair. The functional and patient-reported outcomes will be presented in a future study after all participants have completed a 2-year follow-up.
Conclusion
CAL degeneration was more severe in anterosuperior-type massive rotator cuff tears. Interestingly, even without acromioplasty, the severity of CAL degeneration did not affect the retear rate of the supraspinatus tendon. The optimal indication for CAL release requires further investigation. Regarding the evaluation of CAL, histological CAL degeneration correlates better with grading of acromial lesions than CAL MRI thickness.
Footnotes
Acknowledgment
The authors thank Musculoskeletal Research Center, Innovation Headquarter, National Cheng Kung University, Tainan and Skeleton Materials and Bio-compatibility Core Lab, Research Center of Clinical Medicine, National Cheng Kung University Hospital, Tainan, for their assistance with this research.
Final revision submitted February 11, 2023; accepted February 26, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was supported by a grant from National Cheng Kung University Hospital (NCKUH-11202002) and a research grant from the Taiwan Ministry of Health and Welfare (MOHW110-TDU-B-211-124003). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from National Cheng Kung University Hospital (reference No. A-ER-109-414).
APPENDIX
Classification Schemes Used in This Study

| Copeland-Levy Classification for Subacromial Degeneration | ||||||
|---|---|---|---|---|---|---|
| Grade 0: Normal appearance of the acromial undersurface | ||||||
| Grade 1: Minor scuffing | ||||||
| Grade 2: Major damage | ||||||
| Grade 3: Visualization of bare bone area | ||||||
| Collin Classification for Massive Rotator Cuff Tears | ||||||
| Type A: Supraspinatus and superior subscapularis tears | ||||||
| Type B: Supraspinatus and entire subscapularis tears | ||||||
| Type C: Supraspinatus, superior subscapularis, and infraspinatus tears | ||||||
| Type D: Supraspinatus and infraspinatus tears | ||||||
| Type E: Supraspinatus, infraspinatus, and teres minor tears | ||||||
| Sugaya Classification of Rotator Cuff Repair on MRI | ||||||
| Type I: Sufficient thickness compared with normal cuff with homogeneous low signal on T2-weighted images | ||||||
| Type II: Sufficient thickness compared with normal cuff with partial high-intensity area from within the tendon | ||||||
| Type III: <50% thickness compared with normal cuff without discontinuity | ||||||
| Type IV: Minor discontinuity (1-2 slices) on both oblique coronal and oblique sagittal images, suggesting small full-thickness tear | ||||||
| Type V: Major discontinuity (>2 slices) on both oblique coronal and sagittal images, suggesting medium or large full-thickness tear | ||||||
| Updated Bonar Score for Histopathological Assessment of Tendinopathy 13 | ||||||
| Cell Morphology | Collagen Arrangement | Cellularity | Vascularity | Ground Substance | ||
| Grade 0 | Inconspicuous elongated spindle-shaped nuclei with no obvious cytoplasm at light microscopy | Tightly cohesive well-demarcated bundles with a smooth dense bright homogeneous polarization pattern with normal crimping | Mainly discrete cells | Inconspicuous blood vessels coursing between bundles | Not stainable ground substance | |
| Grade 1 | Increased roundness: nucleus becomes more ovoid to round in shape without conspicuous cytoplasm | Diminished fiber polarization; separation of individual fiber bundles but with maintenance of overall bundle architecture; nonhomogeneous polarization | Hypercellularity, in runs and/or increased cell numbers | Occasional cluster of vessel, <2 per 10 high-power fields | Stainable mucin between bundles but bundles still discrete | |
| Grade 2 | Increased roundness and size; the nucleus is round, slightly enlarged, and a small amount of cytoplasm is visible | Bundle changes: separation and loss of demarcation of fiber bundles, giving rise to expansion of the tissue overall and clear loss of normal polarization pattern | Areas of hypo- as well as hypercellularity | 2-3 clusters of capillaries per 10 high-power fields | Stainable mucin within bundles with loss of clear demarcation of bundles | |
| Grade 3 | Nucleus is round, large with abundant cytoplasm and lacuna formation (chondroid change) | Marked separation of fiber bundles with complete loss of architecture | Area of assessment is mostly acellular | Areas with >3 clusters per 10 high-power fields and/or areas of pathological avascularity | Abundant mucin throughout the section with inconspicuous collagen staining | |