
Abstract
Background:
Anterior cruciate ligament (ACL) injuries are among the most common sports-related injuries, and they can have a negative impact on players’ ability to return to play (RTP). There is a paucity of literature focused on RTP after ACL reconstruction (ACLR) in collision sports.
Purpose:
To characterize the impact that an ACL injury has on the ability to RTP and the post-ACLR performance level in American football players.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
An electronic search was performed using the following databases: the Cochrane Database of Systematic Reviews, the Cochrane Central Register of Controlled Trials, PubMed, Embase, and the Cumulative Index to Nursing and Allied Health Literature. Included studies were written in English; were published since the year 2000; examined only American football players; and reported on RTP, performance, and/or career length after primary ACLR.
Results:
The initial search yielded 442 unique studies. Of these, 427 were removed after screening, leaving 15 studies that met inclusion criteria. An additional 2 studies were identified in these studies’ references, yielding a total of 17. The rate of RTP after ACLR for football players was 67.2% (1249/1859), and the mean time to return was 11.6 months (range, 35.8-55.8 weeks). Although considerable heterogeneity existed in the study design and outcomes measured, in general, a majority of football players experienced greater declines from their preinjury performance level than controls over the same time period.
Conclusion:
An ACL injury negatively affected football players’ ability to RTP and their post-ACLR performance. The degree of effect varied by several factors, including playing position, preinjury performance level, and National Football League Draft round. These results may be used by physicians and football players to develop reasonable expectations for returning to play and performance after an ACL injury.
Keywords
Anterior cruciate ligament (ACL) injuries are common in sports that require sudden changes in acceleration and quick jumping, cutting, and pivoting motions, such as American football (subsequently referred to as football). 1,10 As many as 8% of all participants at the National Football League (NFL) Scouting Combine have a history of ACL injuries. 5,8 Previous studies have shown that such injuries require prolonged time away from competition and extensive rehabilitation after primary ACL reconstruction (ACLR), which not only imparts the psychological burden of the fear of reinjuries on players but also a financial burden, given the time missed. 1,27,34,36 Numerous studies have shown that an ACL injury in football is significantly correlated with negative outcomes compared with controls, from decreased on-field performance to shorter careers. 7,8,25,26,32 Given the popularity of football in the United States, it is imperative that a better understanding of how an ACL injury affects participation in football is attained.
A major goal for players after ACLR is to successfully return to play (RTP) at the same preinjury skill and competition level. 1,2,20 Previous literature has suggested that players’ ability to RTP successfully is dependent on numerous factors, ranging from the type of sport to playing position. 12,13,15,26,36 –38 The purpose of this study was to perform a systematic review of the literature reporting RTP data and performance level after ACLR in football players.
Methods
Study Identification and Selection
This study was conducted in accordance with the 2015 PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. 28 A systematic review of literature reporting RTP data after ACLR was performed using the Cochrane Database of Systematic Reviews, the Cochrane Central Register of Controlled Trials, PubMed, Embase, and the Cumulative Index to Nursing and Allied Health Literature. The search was performed on June 19, 2019. The search terms were as follows: “American football” AND “anterior cruciate ligament injuries” (Medical Subject Headings terms).
Studies were included if they met the following criteria: evaluated RTP, performance, career length, and/or injury data after primary ACLR with at least one 12-month follow-up; examined American football players; were written in the English language; and were published in the year 2000 or after. Exclusion criteria were as follows: studies that included nonathletes, examined any sport besides American football, or explicitly included only nonisolated ACL injuries; editorial studies; basic science studies; studies published before the year 2000; case reports; epidemiological studies (without RTP outcome data); non-English studies; systematic reviews; and meta-analyses.
Two investigators (B.J.R., I.S.-E.) independently reviewed the titles and/or abstracts of all identified studies. Subsequently, full texts were reviewed for a further assessment of inclusion and exclusion criteria. Studies that met inclusion criteria were aggregated, and the references from these studies were scanned to ensure that the systematic review encompassed all relevant studies concerning the topic.
Data Collection
Each included study was assigned a study type and corresponding level of evidence as specified by Wright et al. 39 If reported, the following data were collected from each study: player demographics, total number of players who underwent ACLR, number of players who returned to play, percentage of players who returned to play, pre- and post-ACLR performance metrics, games played, games started, and career length. When applicable, this data was recorded both for players who underwent ACLR and for controls who did not. If available, only data for isolated ACLR was recorded; however, some studies did not state explicitly if the patient underwent ACLR alone or in combination with other procedures or did not separate RTP data as such. For continuous variables (age, timing, outcome data, etc), the mean and range and/or standard deviation were recorded unless otherwise specified.
Results
Search Results
The initial search yielded 614 studies (Figure 1). After the removal of 172 duplicates, 442 unique studies remained. Subsequently, 402 studies were removed based on exclusion criteria. The remaining 40 studies underwent a full-text review, and 25 more studies were excluded, yielding 15 studies for inclusion in the study. An additional 2 studies that met inclusion criteria were found in the references of the other 15 included studies. Thus, a total of 17 studies were included in this systematic review.

PRISMA (Preferred Reporting Items for Systematic Meta-Analyses) flow diagram. ACL, anterior cruciate ligament; ACLR, ACL reconstruction; RTP, return to play. *Some articles were excluded for multiple reasons; therefore, the figures outlined in the exclusion explanations do not match the total articles excluded for each screening.
Football Data
The characteristics of the 17 included studies are listed in Table 1. One study 27 reported on high school and college players, 2 studies 14,38 reported exclusively on college players, 4 studies 6,7,8,22 reported on NFL and college players, and the remaining 10 studies § reported exclusively on NFL players. Moreover, 9 studies provided the mean age of players; the weighted mean age of players who were able to RTP in these studies was 26.0 years (range, 25.2-27.3 years). ∥ No studies found significant correlations between age and ability to RTP. The type of graft used for ACLR was reported in 3 studies; bone–patellar tendon–bone autografts were the most frequently used graft in each study, followed by hamstring tendon autografts. 14,27,35 However, only Daruwalla et al 14 found a significant difference in graft type versus RTP percentage, with autografts yielding a higher RTP percentage than allografts (P = .045). Two studies reported on reinjury rate, but no significant associations between the reinjury rate and RTP rate were found. 19,29
Characteristics of Included Studies a

a Allo, allograft; auto, autograft; BPTB, bone–patellar tendon–bone; DL, defensive linemen; HS, high school; HT, hamstring tendon; LOE, level of evidence; N/A, not available; NCAA, National Collegiate Athletic Association; NFL, National Football League; OL, offensive linemen; RTP, return to play.
b Values are presented as mean, mean ± SD, or mean (range).
The 17 studies included a total of 2195 ACLR procedures. Of these, 3 studies (18%) did not specify how many players returned to play after ACLR. 7,22,31 The remaining 14 studies (82%) reported that 1249 players returned to play during the course of each study period (Appendix Table A1). ¶ The mean RTP percentage across these remaining 14 studies was 67.2% (1249/1859). However, there was considerable variance in how each study defined successful RTP and how players were divided into groups (individual positions, “skilled” vs “unskilled” positions, etc) (Appendix Table A1). Brophy et al 6 reported the lowest overall RTP percentage at 45.9% (130/283) for players participating in the NFL Scouting Combine, while Erickson et al 19 reported the highest RTP percentage at 92.9% (13/14) for NFL quarterbacks. Additionally, 8 studies 10,12,14,19,25,29,32,35 explicitly reported the mean time to RTP (weighted mean, 11.6 months [range, 35.8 14 to 55.8 10 weeks]).
There were 7 studies that reported the number of games played by players after ACLR versus controls (Appendix Table A2). 7,8,10,12,19,22,31 Brophy et al 8 found that ACLR significantly reduced games played by NFL offensive linemen compared with controls (P = .003), and Frank et al 22 concluded that players with a history of ACLR at the NFL Scouting Combine played in fewer games in their first 2 NFL seasons following ACLR than controls (P < .05). Additionally, 5 studies analyzed the number of games started (ie, first on the depth chart) for players who underwent ACLR versus controls either before or after the injury (Appendix Table A2). 7,12,22,31,32 Of these studies, 3 found significant differences. Frank et al 22 (P < .01) and Provencher et al 31 (season 1: P = .005; season 2: P = .002) found that players with a history of ACLR at the NFL Scouting Combine started fewer games in the following 2 seasons than controls. Read et al 32 concluded that NFL players who underwent ACLR had started a greater proportion of games before their injury than controls and experienced a greater decline in the proportion of games started after the injury than controls over the same time period (P = .004). Also, 4 studies reported on career length for players who underwent ACLR versus controls (Appendix Table A3). 7,12,19,32 Only Cinque et al 12 found significant differences, concluding that ACLR reduced the total career length of NFL defensive linemen significantly versus control defensive linemen (P = .020).
Three studies compared the number of games played before and after ACLR for football players who returned to play (Appendix Table A2). 25,35,40 Of these, 2 studies found that the number of games played after the injury was significantly lower than the number played before the injury (P = .001 25 and P < .001 35 ), whereas the third study concluded that players who were able to RTP less than 18 months after the ACL injury had played significantly more games before the injury than players who were not able to RTP within 18 months (P = .018). 40 Furthermore, 2 studies analyzed the number of games started among players who underwent ACLR and were able to RTP, and both reported significant results. Yang et al 40 found that players who were able to RTP in less than 18 months after an ACL injury had started significantly more games before the injury than players who were not able to RTP within 18 months (P = .017). Read et al 32 concluded that NFL defensive players who underwent ACLR started in significantly fewer games after their injury than they had before the injury (all positions: P < .001; defensive backs: P = .022). Also, 3 studies analyzed career length for their respective ACLR cohorts (Appendix Table A3). 25,35,40 Of these, 2 studies found that players’ postinjury career length was significantly shorter than their preinjury career length (P = .01 25 and P < .001 35 ).
There were 10 studies that analyzed some degree of performance in players who were able to RTP after ACLR (Appendix Table A4). # The metrics used displayed a high degree of heterogeneity between studies. Furthermore, performance metrics measured typically varied by position (receiving yards by wide receivers, tackles by linebackers, etc). Of these, 5 studies found significant differences in performance metrics between players who returned to play after ACLR versus controls. 10,22,31,32,38 Carey et al 10 found that NFL running backs and wide receivers had higher average power ratings (an artificial statistic that combines yards gained and touchdowns) versus controls in the season before the injury (P = .0008) and lower average power ratings in the season of the injury (P < .0001). Wise and Gallo 38 similarly found that after ACLR, college running backs averaged fewer carries per game (P = .003), yards per game (P = .006), and receptions per game (P = .011) than controls. Their study also found that wide receivers averaged fewer receptions per game (P = .004), yards per game (P = .0009), and touchdowns per game (P = .004) than controls after ACLR. 38 Frank et al 22 found that defensive backs with a history of ACLR had significantly fewer interceptions in their first 2 seasons than controls (P < .05) and that defensive linemen with prior ACLR had significantly fewer quarterback hits than controls (P < .05). Similarly, Wise and Gallo concluded that college linebackers averaged fewer tackles for loss (P = .0003) and sacks (P = .026) than controls after ACLR and that defensive backs also averaged fewer tackles for loss (P = .002) and sacks (P = .043) than controls after ACLR. Provencher et al 31 concluded that NFL players with prior ACLR participated in a lower percentage of plays in both the first (P < .001) and the second (P < .001) seasons after the NFL Scouting Combine compared with controls. Read et al 32 found that NFL defensive players had higher average solo tackles per game in the season before their ACL injury than controls (P = .022). Additionally, their study found linebackers averaged more interceptions per game before the injury than controls (P = .039). 32
There were 3 studies that found significant differences between players who underwent ACLR and were able to RTP versus those who did not RTP (Appendix Tables A2-A4). 27,32,35 Shah et al 35 found that NFL players who were able to RTP after ACLR had played more games (P = .04) than players who were unable to RTP after ACLR. Read et al 32 similarly reported that NFL defensive players who were able to RTP started more games (P = .014) before the injury. Additionally, these players averaged higher combined tackles (P = .002), solo tackles (P < .001), forced fumbles (P = .036), passes defended (P = .002), interceptions (P = .001), and defensive touchdowns (P = .046) per game than players who were unable to RTP after ACLR. McCullough et al 27 found that at 2-year follow-up after ACLR, college football players who were able to RTP had significantly higher International Knee Documentation Committee (P = .04), Marx activity scale (P < .01), and Knee injury and Osteoarthritis Outcome Score (KOOS) Knee-Related Quality of Life (P < .01) scores than similar players who were unable to RTP.
There were 2 studies that found significant declines in performance metrics in players who underwent ACLR and returned to play after the injury compared with before the injury (Appendix Table A4). 25,32 For all included players who returned to play, Read et al 32 found that NFL defensive players averaged fewer combined tackles (P = .013), solo tackles (P < .001), passes defended (P < .05), and interceptions (P = .005) per game than they had before the injury. By position, linebackers and defensive backs averaged fewer solo tackles per game after ACLR, and defensive backs also averaged fewer interceptions per game (all P < .05). 32 Using a unique game statistic–based performance score algorithm, Mai et al 25 found that NFL players performed at a lower level in both the first (P < .001) and second (P = .0001) seasons after the injury compared with their level of performance in the season before the injury.
Discussion
RTP Rates
A primary goal of this review was to report on RTP after ACLR in football players; 82% (14/17) of included studies included adequate data (Figure 2). Our study demonstrated that football players had a mean RTP rate of 67.2% (1249/1859) across all studies that provided adequate RTP data, inclusive of all age groups and positions. As prior studies have reported, RTP rates varied significantly by player position. 3,4,16,40 For example, numerous studies reported that offensive linemen return to play at rates of ∼60%, 8,12,17,35 whereas quarterbacks return to play at rates of >90%. 19,35,38 The risk of developing an ACL injury itself seems to display positional variance as well; previous literature suggests that running backs and linebackers are at the highest risk. 3,4,8,16 Other factors have been associated with the risk of ACL injuries and the ability to RTP, including higher levels of preinjury performance being predictive of future ACL injuries 10,32 and earlier draft round/position, more game experience before the injury, use of autografts, scholarship status (college players), and higher depth chart position for RTP after ACLR. 14,17,35,40 It must be noted, however, that these conclusions are based on the included data which is heavily biased toward NFL and National Collegiate Athletic Association (NCAA) Division I athletes (16/17 included studies). Given the exceptional skill required to participate at this level of competition, as well as the apparent correlation between skill and ability to RTP after ACLR, more research is needed to investigate RTP after ACLR in high school athletes and college athletes competing in lower NCAA divisions.

Return to play (RTP) rates in football players after anterior cruciate ligament reconstruction.
Time to RTP
The studies included in our review demonstrated that the weighted mean time to RTP after surgery for football players was 11.6 months, although considerable variance existed between included studies. It is unclear what factors underlie these differences in RTP rates and time to RTP, but they could be attributed to differences in the definition of successful RTP, time of injury during the season, time between injury and surgery, graft type, or rehabilitation protocol. Because the NFL/NCAA regular season is 4 months long (September-December), if successful RTP is defined by participation in games, an athlete who sustains an ACL injury at the beginning of the season may face a minimum of 12 months to RTP, while an athlete who is hurt in December may instead face a minimum of approximately 9 months to RTP. Most of the studies (15/17) included in this review explicitly defined successful RTP as participating in a game, which limits the ability to understand exactly how long it takes for elite football athletes to recover from an ACL injury from a clinical standpoint.
Despite this limitation, there are some data to suggest that lengthy times to RTP seem to be the norm in football, even when defined by a clinician. For example, a survey of NFL team orthopaedic doctors conducted by Schrock et al 33 found that only 14% (4/29) of physicians would allow a player to RTP at ≤6 months after ACLR. A similar study by Erickson et al 18 found only 56.2% (77/137) of NFL and NCAA physicians would clear a player to return at 6 months, and 12.4% (17/137) would not clear a player in less than 9 months. Further research is needed to investigate the factors that underlie the differences in time to RTP in football players and to elucidate rehabilitation protocols that minimize recovery time.
Determinants of RTP
Returning to competition after an ACL injury is a difficult and complex process, and as such, the determinants of players’ ability to RTP seem to be a range of variables that interact with each other. Although it is possible that differences in surgical care are driving the variance in RTP rates between studies, this possibility seems minimal. In the 3 studies that reported on graft type, bone–patellar tendon–bone autografts were most frequently used for ACLR. 14,27,35 This result aligns with 2 separate surveys of NFL and NCAA team orthopaedic surgeons regarding their preferred ACLR methodology. 11,18 Although this review found that autografts were most commonly used, there is a relative paucity of evidence in the literature connecting specific ACLR graft choices to superior clinical outcomes. 9,21,23,41 More research is needed to elucidate which graft choice is optimal for RTP in collision sports.
The limited ability to RTP after ACLR could reflect a bias against players with a history of ACL injuries in professional football. 34 Three included studies found that a history of ACLR negatively affected players’ NFL Draft position. 22,31,35 Several studies also reported that RTP rates varied significantly by player position. 3,4,16,40 Although the factors underlying these differences remain unclear, it is possible that a bias against players with prior ACLR may be more pervasive for certain playing positions and thus create a greater barrier to RTP. For example, because the quarterback position generally requires fewer cutting and pivoting movements and involves less physical contact, a history of ACLR may have less of an impact on the career of quarterbacks relative to other positions. This notion may be illustrated by the exceptionally high RTP rates for quarterbacks in this review, whereas an ACL injury was largely a significant derailment for athletes who played positions such as lineman, linebacker, and running back. Although our results suggest differences in RTP rates and time to RTP between studies and player positions, statistical analysis is needed to both validate and quantify these differences. Further studies are also needed to investigate the underlying factors driving the continued limitations in RTP after ACLR in football.
Athletic Performance After ACLR
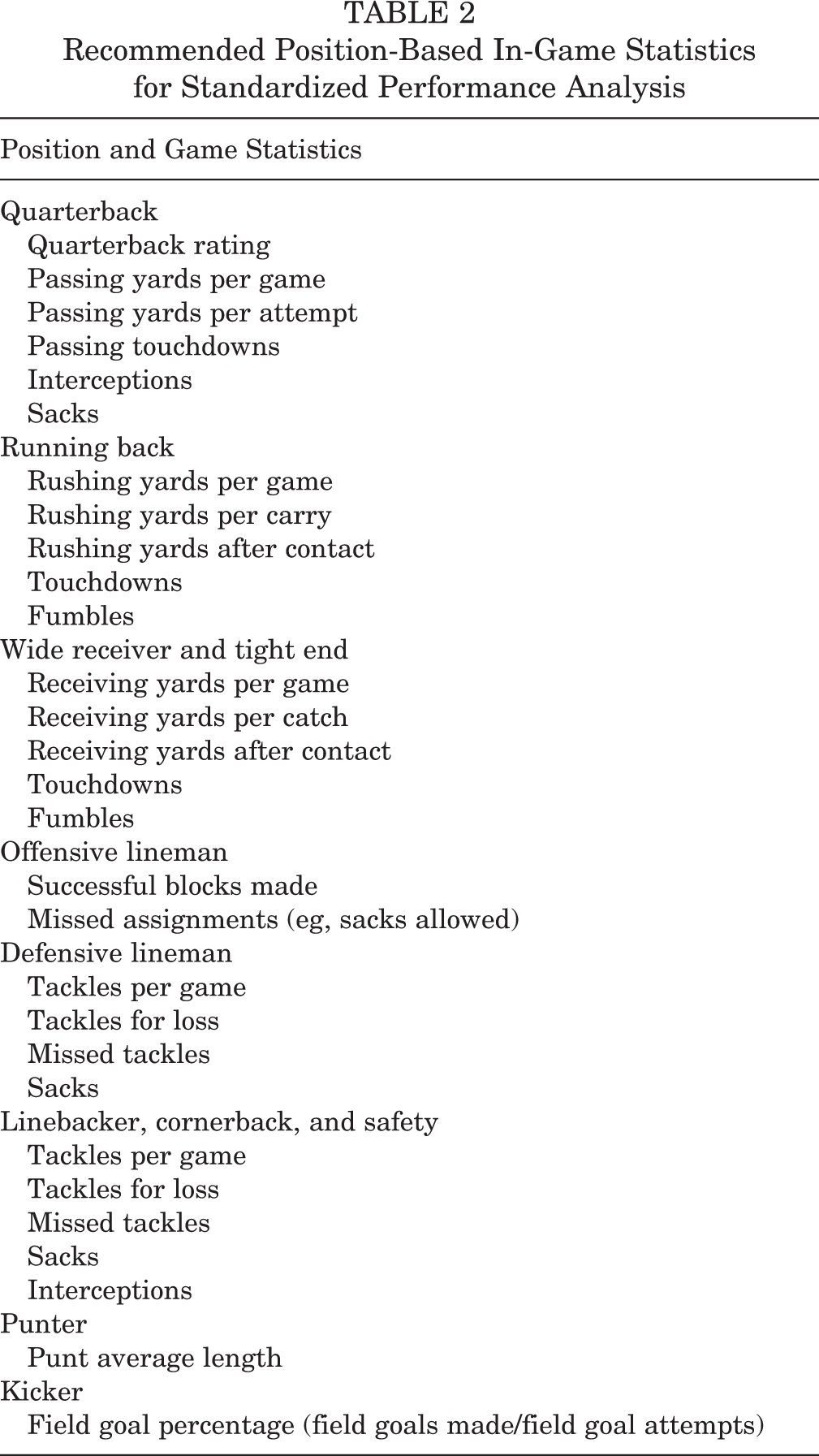
After ACLR, most athletes seek to reach their preinjury level of performance. However, it is difficult to synthesize the results from the 10 studies that included post-ACLR performance data in this systematic review, given the high degree of heterogeneity in how each study measured performance, the different athlete populations, and the scarce use of control groups (only 7 studies). These limitations make it difficult to draw concrete conclusions. In general, compared with control groups, players who underwent ACLR and returned to play subsequently played and started in fewer games and had shorter careers, although there was considerable positional variance. 8,12,22,31 These players also tended to start more games and were higher performing players compared with controls before their injury but experienced marked declines in performance after surgery. 10,22,25,31,32,38 This result may suggest that high-performing players are at a higher risk of ACL injuries because of increased opportunities for such an injury. Future studies should standardize the collection of performance data by position so that statistical analysis can be adequately powered to provide more accurate data points. A substantial amount of data is readily available to the public, especially for NFL and NCAA athletes. Defining a standardized set of position-based statistics (Table 2) that could be used for the purpose of academic analysis, although not inclusive of all tracked statistics, may strengthen the conclusions that can be drawn from the data in future studies.
Recommended Position-Based In-Game Statistics for Standardized Performance Analysis
Previous Work
Previous systematic reviews have analyzed outcome data in players after ACLR. Lai et al 24 performed a systematic review and meta-analysis of RTP and performance after ACLR across several sports, including collision sports such as football and rugby. The authors found that the average time to RTP for football players ranged from 8.2 to 13.0 months after ACLR. However, while Lai et al concluded that RTP rates did not depend on playing position, the present review suggests that positional variance does play a role. This difference may be attributed to the fact that this review includes more studies specific to football as well as more recently published literature. Thus, to our knowledge, this review is unique in its breadth of coverage, inclusion of recent literature, and targeted focus on football. Further research is warranted on numerous topics including position-specific RTP comparisons, collision sports–focused reviews, and further stratification based on graft type.
Limitations
There are several limitations to this study. As with any systematic review, variation limits the ability to draw conclusions from the data. The lack of standardization in RTP definitions, performance outcome measures and reporting methods, control groups, and reporting of polytrauma versus isolated injuries limited our ability to make cross-comparisons between studies. There was a broad time frame of data collection, with players from as early as 1987 and as late as 2015 being included. Advances in sporting techniques, surgical care, and rehabilitation protocols could skew the uniformity of the results; RTP rates have been, in fact, increasing steadily over time. 6 Additionally, the risk of bias was identified in several studies. A total of 3 studies only measured outcome data for players who successfully returned to play after ACLR, thus introducing selection bias by not including data for players who underwent ACLR but could not return to play. Therefore, the results of those studies cannot necessarily be applied to the average player. Only 1 included study collected data prospectively, introducing the risk of recall bias. Studies classified as level of evidence 3 or 4 (16/17 studies) may be affected by selection and/or performance bias because of the lack of randomization and prospective comparative control groups. Additionally, all 17 studies reported on only male players, and therefore, this analysis should not be extrapolated to female players who are known to be at a higher risk of ACL ruptures while participating in the same sports as male athletes. 30 Furthermore, given that 16 of 17 included studies reported exclusively on NFL or NCAA Division I athletes, the results of this study cannot necessarily be applied to younger athletes or athletes of lower skill levels.
Conclusion
This systematic review demonstrated that after ACLR, the rate of RTP for football players was 67.2%, although rates varied considerably between studies and by playing position. The majority of football players who returned to play experienced significant post-ACLR performance declines compared with controls and their own preinjury level of performance. While previous RTP literature has been more broadly focused, these data may be helpful in characterizing the burden of ACL injuries on the ability to RTP for players participating in football or other collision sports. With more focused data, physicians and players can develop more targeted and accurate expectations for collision sports participation and performance after ACLR. Further research in the form of prospective comparison trials or meta-analyses is warranted, as these injuries are common in football and other collision sports, and rates of RTP remain variable.
Footnotes
Final revision submitted April 28, 2020; accepted May 15, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: M.K.M. has received educational support from Arthrex, Alon Medical Technology, and Quest Medical; nonconsulting fees from Arthrex; and hospitality payments from Zimmer Biomet. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.