
Abstract
Background:
Return to sport is a goal for most patients who undergo anterior cruciate ligament (ACL) reconstruction. However, at a nonelite level, there are limited sport-specific data regarding rates or factors associated with return to play.
Purpose:
To report rates and determinants of returning to play Australian Rules football after ACL reconstruction in male nonprofessional athletes.
Study Design:
Case-series; Level of evidence, 4.
Methods:
A total of 354 male nonprofessional Australian Rules football players who had undergone primary ACL reconstruction were asked to complete detailed sports activity questions at 12 months and 2 to 5 years (mean, 3 years) after surgery. Rates of return to play were calculated for both timepoints, along with preoperative patient expectations and postoperative sport performance. The following predictors of return to play were examined: age at surgery; height; weight; frequency of weekly football participation; sport participation level; psychological readiness to return to sport; and knee-related quality of life. Further ACL injuries were also documented. Descriptive statistics were used to summarize return-to-play data and contingency analysis for predictors of return to sport.
Results:
The rate of return to any level of play was 35% (95% CI, 30%-41%; n = 284) at the 12-month follow-up and 78% (95% CI, 72%-83%; n = 233) at the 2- to 5-year follow-up. Overall, 64% (95% CI, 57%-70%) of the patients were able to return to their same or higher level of play. Before surgery, 92% of the patients expected to return to their same preinjury level of Australian Rules football participation. At the 2- to 5-year follow-up, 61% who returned to play felt that they could perform as well as they could before their ACL injury. A greater psychological readiness to return to sport preoperatively and higher level of sport participation were significant predictors of a return at 2 to 5 years. Further ACL injuries were sustained by 21% of the cohort (15% graft rupture; 6% contralateral ACL injury).
Conclusion:
Most male athletes who participate in Australian Rules football returned to some level of play after ACL reconstruction; however, only 64% returned to preinjury levels. Preoperative expectations were not met, and high reinjury rates are a cause for concern.
Most athletes who sustain an anterior cruciate ligament (ACL) injury undergoing reconstruction surgery expect to be able to return to sport. 10,20 However, for many, this expectation is not always met. For nonelite-level athletes, it is estimated that only 42% return to competition sport, which is markedly less than for elite-level athletes, where more than 80% return. 2 At the elite level, some differences in return rates have been reported among different sports. In elite soccer, the return-to-sport rate has been estimated at 85%, whereas a slightly lower rate has been estimated for American football (78%). 13 At the nonelite level, it may also be of benefit to examine whether return rates vary according to sport to give patients realistic expectations regarding return to play.
Australian Rules football is the most popular of the various codes of football played in Australia, with the number of participants is estimated to exceed 1.7 million. 5 Players can move the ball by hand or foot and dispose of the ball in any direction. When in control or possession of the ball, a player may be tackled from any direction and therefore have to try to evade opposition players. Consequently, players perform many landings, cutting and pivoting movements, per game, which exposes them to significant risk for ACL injuries.
Australian Rules football is played in organized competitions or leagues. Clubs typically consist of 30 to 50 players. The premier professional competition is the national Australian Football League, which is supported by semiprofessional state leagues that provide opportunities for national league–listed players either not currently playing or not selected to play in the national league as well as elite-level players who typically have another occupation. Below these levels are numerous leagues with different grades. Although fundamentally amateur, in some instances, individual players may receive some financial support from their club. Some of these recreational leagues can in fact be elite, such as the “under-18 competition” in which aspiring elite footballers are selected to play, as well the highest grades of geographically organized leagues. In addition, there are high school competitions. University- or college-based teams compete in the geographically based leagues rather than intercollegiately.
Audits of the Australian Football League have shown that 74% to 77% of players return to competition play after ACL reconstruction, with those who had played more matches before injury and who were higher draft pick (first round or priority pick) players more likely to return. 8,14,15 At the nonprofessional level, there is a paucity of data. Ardern et al 4 reported a return-to-play rate of 42% at 12 months after ACL reconstruction in a cross-sectional study of 197 athletes who participated in Australian football. A subsequent study of 40 athletes who played Australian football showed that only one-third more had returned to play between 1 and 2 years postoperatively. 3 There are no further published data on return rates after ACL reconstruction in nonprofessional Australian footballers beyond the first postsurgical year to determine how many players eventually make a return, nor has there been an exploration of factors associated with a return to play.
The aim of this study was to report rates and determinants of returning to Australian Rules football in nonprofessional male athletes at 12 months and 2 to 5 years after ACL reconstruction surgery.
Methods
Patients
All study procedures received ethics committee approval. Consecutive patients who had undergone primary ACL reconstruction surgery between January 2014 and December 2017 were identified from a practice database of 3 specialist knee surgeons. Patients were included if they had listed nonprofessional Australian Rules football as their primary sport before their ACL injury on a preoperative questionnaire, were male, and aged between 14 and 40 years at the time of surgery. The following exclusion criteria were applied: additional knee ligament surgery at the time of the reconstructive surgery; prior contralateral ACL injury; professional athlete; did not play Australian Rules football on a weekly basis before injury; and use of allograft or autograft obtained from contralateral side.
Surgical and Rehabilitation Details
All ACL reconstruction surgeries were performed arthroscopically using either hamstring tendon, patellar tendon, or quadriceps tendon autograft. Graft selection was made by the patient and, in the case of minors, their family, after discussion of graft options with the treating surgeon. A variety of factors influenced graft choice, including previous experiences of friends and relatives, advice from primary care practitioners, and media attention paid to professional athletes undergoing ACL reconstruction. Patient preference was paramount, unless there was a specific contraindication such as open growth plates, in which case patellar tendon and quadriceps tendon graft were not used. During the period in which patients had their surgery, the hamstring tendon was the default graft preference for all 3 surgeons. Femoral fixation was by means of an Endobutton (Smith & Nephew, Andover, Massachusetts, USA) and tibial fixation by means of an interference screw, regardless of graft type.
All patients underwent the same rehabilitation protocol, with a focus on early recovery of full active knee extension and quadriceps function. Weightbearing was allowed on an as-tolerated basis from the first postoperative day. No braces or splints were used. Progression was guided by the presence and degree of pain and swelling. Typical timeframes were stationary cycling from 3 to 4 weeks; gymnasium-based strengthening exercises and plyometric exercises from 8 to 10 weeks; running from 12 to 14 weeks with progression to change-of-direction work after 4 weeks; and sports-specific drills from 5 to 6 months with a gradual resumption of team-based training from 9 to 10 months. 6 The minimum requirements for return-to-sport clearance from the treating surgeon were no effusion, an essentially full range of motion, good quadriceps strength with good control of a single leg squat, observation of normal running and landing, and at least 4 weeks of unrestricted training. These minimum requirements were not assessed as part of a formalized return-to-sport test battery.
Return-to-Sport Measures and Data Collection Procedures
Patients completed a preoperative questionnaire in which they documented their level and frequency of sport participation before ACL injury. They also answered several questions regarding their postoperative return-to-sport expectations, which have been previously used in this population. 20 In addition, patients completed the Anterior Cruciate Ligament–Return to Sport after Injury (ACL-RSI) scale, 21 which measures psychological readiness to return to sport, as well as the Knee-related Quality of Life subscale of the Knee injury and Osteoarthritis Outcome Score (KOOS-QOL), 18 and the Marx activity scale.
At 12 months after surgery, patients completed an additional questionnaire during a routine clinical follow-up appointment in which they reported whether they had returned to their sport as well as the level of return (no return, return to training, return to lower level, or return to same or higher level). Those who had not returned were also asked to indicate whether they still planned to return and, if not, the reason why.
The same patient group was then evaluated at between 2 and 5 years after surgery when they were sent an electronic survey and asked to respond to the same return-to-sport questions (Appendix Figure A1). Questions related to return-to-sport performance and further injury were also included. For performance, patients who had returned to sport were asked whether they “felt as though they could play (or perform) as well as before their ACL injury” (yes/no response). Regarding injuries, patients were asked to report the number and type (graft rupture, contralateral ACL injury) of any second ACL injury and the date of occurrence. Any patient who did not complete the survey was individually contacted via telephone. Medical records of the entire cohort were also checked to confirm reinjury details, and demographic (age at surgery, sex), injury, and surgical information were also recorded from our prospectively collected patient databases.
Analysis
Return-to-sport rates and 95% CIs were calculated for both the 12 month and 2- to 5-year timepoints. Descriptive statistics were used to summarize return-to-sport expectations, discontinuing sport participation responses, self-rated performance measures, and reinjuries. Predictors of return to sport were examined and included age at surgery and preoperative height, weight, preinjury sporting level, frequency of weekly football participation, psychological readiness to return to sport (ACL-RSI score), and knee-related quality of life (KOOS-QOL score). Predictor variables were categorized with cutoff values of 20 years, 180 cm, 80 kg, and score of 50 (out of a possible 100), and the Pearson chi-square test used to determine significance between patients that had and had not returned to play. These cutoff values were pragmatic and similar to those that have been used in our prior studies or are midpoints of the measurement scale. 14,19 Data were analyzed with SPSS Version 27 (IBM), and statistical significance was set at P < .05.
Results
Of 491 patients for whom Australian Rules football was their primary sport, 137 did not meet the study inclusion criteria, which left 354 eligible patients. There were 17 patients who did not complete any follow-up data, and 77 patients completed only 1 of the 2 follow-up timepoints, leaving 284 patients with 12-month return-to-sport data and 233 patients with 2- to 5-year data. Figure 1 shows the flow of patient selection and numbers available at each assessment timepoint. All patients who completed 12-month return-to-sport measures had been cleared for return to sport by their treating surgeon.

Flowchart of patient selection and patient follow-up. ACL, anterior cruciate ligament; CL, contralateral; RTS, return to sport.
Of the 354 included patients, 343 (97%) sustained their ACL injury playing sport and 324 (94%) of these sporting injuries occurred while playing Australian Rules football. Of the ACL injuries that were sustained playing Australian Rules football, 181 (56%) were noncontact, 92 (28%) involved direct knee contact, and 51 (16%) involved upper body contact. Further patient demographics of the cohort are detailed in Table 1.
Participant Demographic Characteristics and Surgical Details (N = 354) a
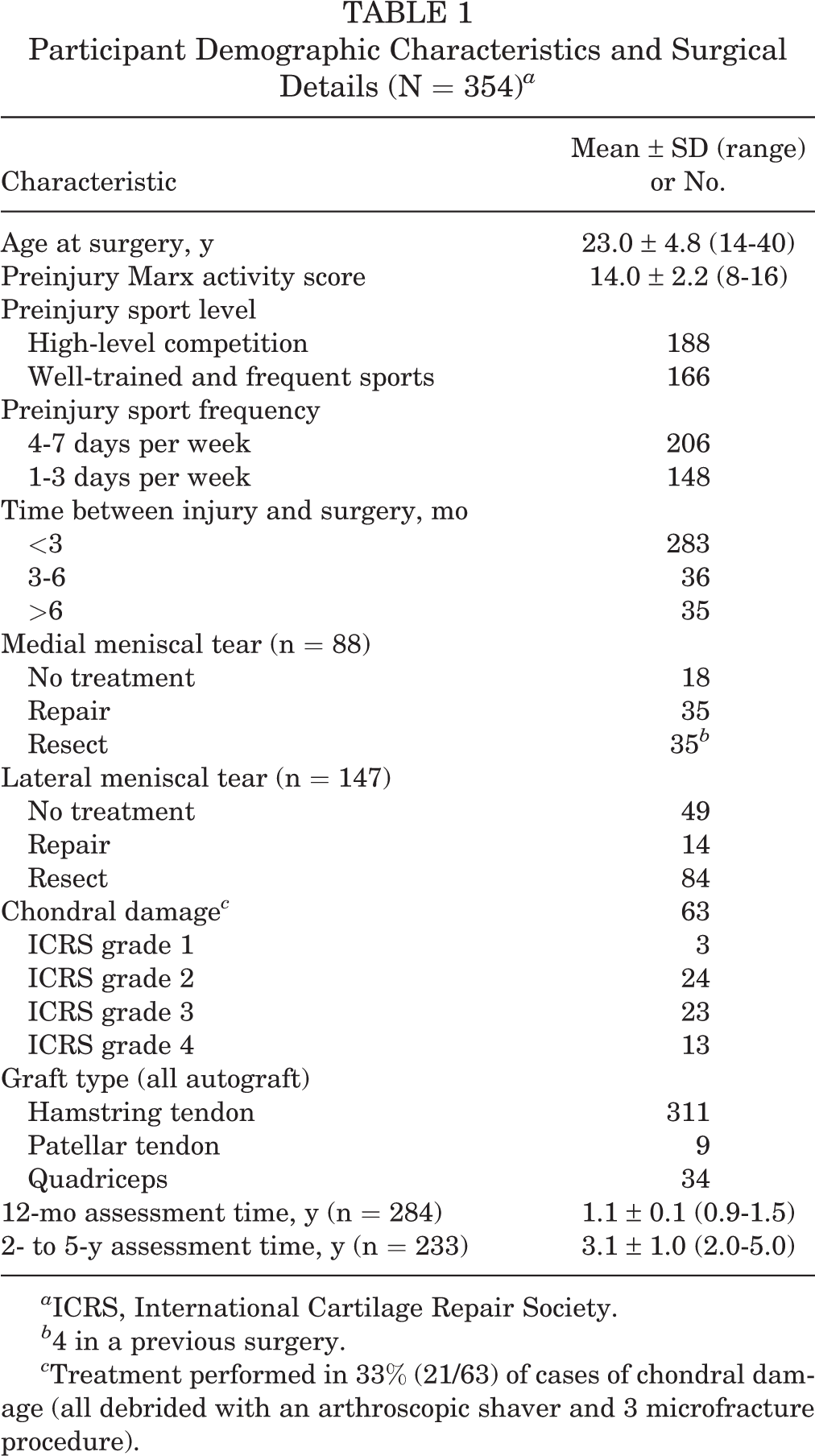
a ICRS, International Cartilage Repair Society.
b 4 in a previous surgery.
c Treatment performed in 33% (21/63) of cases of chondral damage (all debrided with an arthroscopic shaver and 3 microfracture procedure).
Return-to-Sport Expectations
Before surgery, 96% (339 of 354) of the cohort expected to return to Australian Rules football and 92% (324 of 354) expected to return to their same preinjury level of sport participation. Of the 30 patients who did not expect to return to their preinjury level of sport, 25 patients were considering changing sports, and 2 patients were considering giving up sport.
Return-to-Sport Rates
The rate of return to play at any level of Australian Rules football was 35% (95% CI, 30%-41%) at 12 months after ACL reconstruction surgery and 78% (95% CI, 72%-83%) at the 2- to 5-year follow-up, which was on average 3 years after surgery. Overall, 64% (95% CI, 57%-70%) of the patients were able to return to the same or higher preinjury level of play (Table 2). Of those who returned to any level of competition, 82% (149 of 182) returned to the same or higher level of play as before their injury (Table 2).
Level of Australian Rules Football Played at 12 Months and 2 to 5 Years After ACLR a

a ACLR, anterior cruciate ligament reconstruction.
Reasons for Not Returning to Sport and Self-rated Performance
Of the 44 patients who never returned to play, 5 indicated that they still planned to return (all were between 2 and 3 years’ postsurgery), and 16 stated that they had not returned due to fear of further injury. One patient stated physical problems with their knee as the reason for nonreturn, and 15 stated that they had not returned for reasons other than their knee (ie, work or family commitments). Seven patients did not offer a response as to why they had not returned or whether they planned to return in the future.
For the 182 patients who had returned to play Australian Rules football at the 2- to 5-year follow-up, 104 (61%) of 171 who responded felt they could perform as well as they had before their ACL injury. However, when this group was divided by level of return, 70% (96/138) of those who returned to their preinjury level felt that they could perform as well as before their ACL injury, whereas only 24% (8 of 33) felt they could perform as well if they returned to a lower level. Patients who returned to the same or higher preinjury level of Australian Rules football had 7 times the odds of reporting that their performance was equivalent to before their ACL injury than those who returned to a lower level (odds ratio [OR] = 7.2 [95% CI, 3-17]; P < .0001). Eleven patients did not respond to the performance question.
Predictors of Return to Sport
Two preoperative factors were significantly associated with an increased chance of returning to play: an ACL-RSI score of more than 50 and a higher preinjury level of play (Table 3). Frequency of preinjury football participation, age, height, weight, or knee-related quality of life presurgery were not significantly related to the 2- to 5-year postoperative return-to-sport rate.
Factors at the Time of First ACL Injury Associated With Differing Rates of Return to Play a
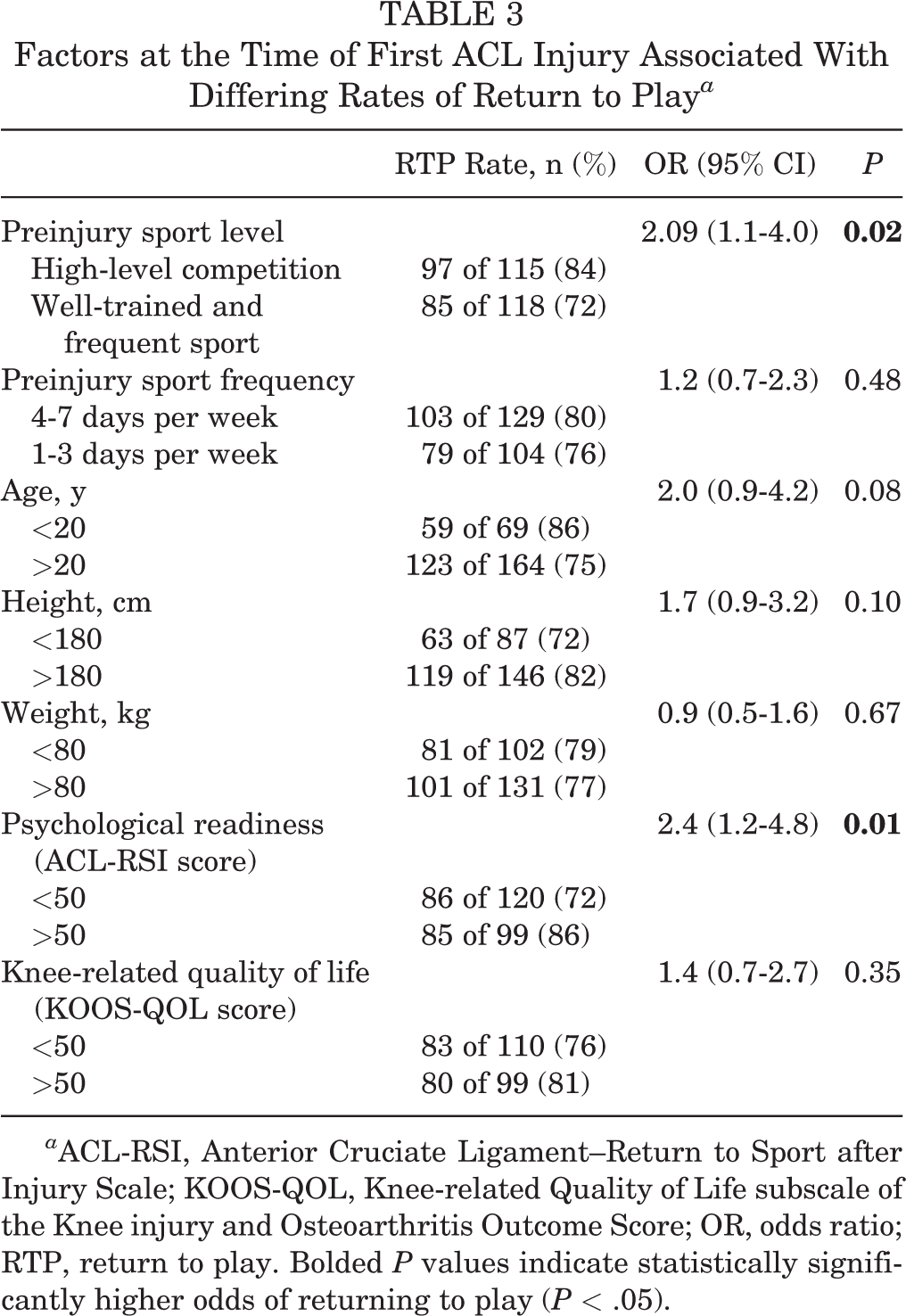
a ACL-RSI, Anterior Cruciate Ligament–Return to Sport after Injury Scale; KOOS-QOL, Knee-related Quality of Life subscale of the Knee injury and Osteoarthritis Outcome Score; OR, odds ratio; RTP, return to play. Bolded P values indicate statistically significantly higher odds of returning to play (P < .05).
Further ACL Injuries
There were 13 graft ruptures and 2 contralateral ACL injuries within the first 12 months of surgery (15 of 303 = 5%). Of the graft ruptures, 8 occurred during Australian Rules football match play, 3 during training, and 2 during non-Australian Rules–football-related sport activities. For the 2 contralateral ACL injuries, 1 occurred during match play and the other in a workplace accident.
At the 2- to 5-year follow-up, there were a further 46 ACL injuries, 31 of these were graft ruptures and 15 contralateral ACL injuries. Graft ruptures occurred while playing competition Australian Rules football for 24 patients and during training for 3. There was 1 non-sport-related graft rupture, and 3 that occurred during participation in different sporting activities (rugby, skateboarding, Ironman competition). Of the 15 contralateral ACL injuries, 13 occurred during Australian Rules football match play, 1 during training, and 1 as a result of a non-sport-related injury.
For both timepoints combined, there were a total of 61 (21%) further ACL injuries in the cohort of 294 who were followed-up, with 44 (15%) graft ruptures and 17 (6%) contralateral ACL injuries. The rate of further ACL injuries was slightly higher in younger (<20 years) patients than older patients (>20 years), but the difference was not statistically significant (24% vs 19%, respectively; P > .05).
Discussion
Despite Australian Rules football being associated with a high rate of ACL injuries, published outcomes specifically related to this sport are lacking for the community level of participation. This study sought to address this gap and provide return-to-sport data in a large cohort of nonprofessional athletes for whom Australian Rules football was their primary sport before injury. Results showed that 78% returned to any level of play and 64% returned to the same preinjury level of competition at an average of 3 years after surgery. Although these rates are lower than preoperative expectations, they are greater than the return rates previously reported when all sports in nonelite athletes are considered together: a 60% rate for returning to the same preinjury sport; and a 42% rate for a return to competition. 2
While there is a paucity of data with which to directly compare the current findings, return-to-sport rates for nonprofessional American football and soccer players have been reported as part of the Multicenter Orthopaedic Outcomes Network (MOON) cohort and can provide a reference against which to compare outcomes for Australian football. 7,16 In soccer, data from the MOON cohort showed a return rate of 76% for male players, with 85% of those who returned playing at the same or higher level as before injury. 7 This is very similar to the current findings for Australian football. In contrast, high school and college-level American football players who were part of the MOON cohort showed lower rates of return to play: 63% and 69%, respectively. 16 Therefore, the rate of return to play after ACL reconstruction in Australian Rules football players are comparable, if not slightly superior, with other sports in which ACL injuries commonly occur.
Only one-third of the cohort had returned to any level of play at 12 months after surgery. This low rate was not unexpected and is consistent with previous data. 4 In addition, the treating surgeons did not encourage football players, particularly younger aged players, to return to competition before 12 months due to the high rates of second ACL injuries that have previously been found in this group. 19 This is in contrast to professional level Australian football players in whom most have returned to competition around the 12-month mark. 14,15 However, there is often significant pressure for professional athletes to make a timely return that does not exist to the same extent at the nonprofessional level. As such, most of the current nonprofessional cohort waited to return until after the first postoperative year.
Similar to previous studies 1,4,12,16 that have included athletes from a range of sports, the reason cited most commonly by those who did not return to Australian football was fear of reinjury. However non-knee-related reasons such as work or study commitments were also noted as a reason for nonreturn. Only 1 patient cited problems with their knee. These data continue to highlight the psychological impact of ACL injury, and psychological readiness was one of the preoperative factors currently found associated with return to play. The level of preinjury sport participation was also associated with return to play, with higher return rates seen for those who had played at higher levels of competition. This may suggest increased motivation or investment in sport, or higher skill level in these athletes, and is consistent with the higher return-to-sport rates that are previously reported for elite-level athletes. Age was not significantly associated with return to play; however, the cohort was relatively young, with only 21 athletes older than 30 years. This may suggest that patients self-select out of playing Australian Rules football at a relatively early age. Of course, there may be other factors predictive of return to play that were not considered, which may include such things as measures of early postoperative recovery of function.
Athletes do not simply aim to return to the field after ACL reconstruction; they also aim to return to their prior level of performance ability. McCullough et al 16 reported that a third of high school and nearly half of college athletes who returned to football did not return to their preinjury performance level at 2 years after ACL reconstruction surgery. In contrast, Webster et al 23 reported that 65% of a similarly young (< 20 years) cohort felt as though they could perform at the same preinjury level across a variety of level 1 and 2 sports when surveyed between 3 and 7 years after reconstruction surgery. In the current study, 61% of the cohort who returned to play felt they had also returned to their preinjury level of performance.
Based on these varied data, it is difficult to provide a precise estimate of return to preinjury level of performance. It is therefore hoped that future studies will continue investigating performance measures in nonprofessional athletes across a range of sports so that more robust estimates can be provided. However, as performance statistics are not typically publicly available in the nonprofessional athlete, there is a reliance on self-reported measures. This offers an important perspective, but further work is needed to confirm the validity of this approach and whether other factors, such as athletes’ preoperative expectations being met, influence or confound the athletes’ perceptions and therefore, rating.
One in 5 patients sustained a further ACL injury over the follow-up period that averaged 3 years. While further ACL injuries were greater in younger patients, with a 24% further injury rate compared with 19% for patients over 20 years, the age difference in further injury rates was not as great as previously reported when all sports are combined. 22 This may highlight the inherent high-risk nature of Australian football for ACL injury. It also supports the idea that it is continued exposure to such sporting environments that places high demands on the knee, rather than age per se, which presents the most significant risk factor for further ACL injury. However, it should be noted that younger patients are more likely to participate in these high-risk sports after ACL reconstruction. 23 Interestingly, there were more than double the number of graft ruptures compared with contralateral ACL injuries. Although the cause of this imbalance is unclear, it is a consistent finding across the literature that male athletes experience a greater proportion of graft ruptures compared with contralateral ACL injuries. 17
A limitation of the current study was the inclusion of only male football players. Although the start of the women’s professional competition (Australian Football League Women’s; AFLW) in 2017 has seen a rapid growth in the number of girls and women participating in community-level Australian football, during the time data for the current study were collected, there were only 30 women (compared with 491 men) who underwent ACL reconstruction and listed Australian football as their primary sport. Given that ACL injuries are the most common injury for women in the AFLW and that they have been estimated to occur at a 6 times higher rate in the professional women’s competition compared with the men’s, we anticipate that we will see a growth in community level ACL injuries in female players. 11,24 We therefore plan to report return-to-sport data for female Australian football players once it is available.
A further limitation was the predominant use of hamstring tendon grafts, and as such, we could not compare return-to-sport rates between different graft types. Although previous findings have been mixed in this regard, a recent review 9 did show graft differences in return-to-sport rates. Finally, only first-time primary ACL reconstructions were included, and as such, return rates for Australian football in patients who undergo revision or bilateral ACL surgeries are unknown and should be determined in future work. Strength and other functional outcomes were not measured to see if they influenced return-to-play rates. Finally, there was some loss to follow-up (14% at 12 months and 17% at 2-5 years), and although overall follow-up rates were acceptable, any loss does affect the validity of the results.
Conclusion
This study showed that 3 of 4 nonprofessional male athletes who participate in Australian Rules football as their primary sport returned to some level of play after a primary ACL reconstruction surgery. However, only 64% return to preinjury levels of participation. Further ACL injuries occurred in 21% of players, which remains a cause for concern.
Footnotes
Acknowledgment
The authors acknowledge the support of Timothy Whitehead and Cameron Norsworthy as part of the OrthoSport Victoria Research Program.
Final revision submitted November 8, 2021; accepted November 12, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.A.F. is a paid associate editor for The Orthopaedic Journal of Sports Medicine. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from La Trobe University (reference No. HEC18439).