
Abstract
Background:
The return-to-sports rate is often used as an outcome measure after anterior cruciate ligament (ACL) reconstruction (ACLR). Although most soccer players want to return to sports after their ACL injury, up to 40% do not believe they will return to soccer after their ACL injury.
Purpose:
To investigate whether self-reported presurgical beliefs regarding return to soccer correspond to registered official match participation after ACLR.
Study Design:
Cohort study; Level of evidence, 2.
Methods:
Included were soccer players with a primary unilateral ACL injury who were ≥15 years at the time of ACLR and who had completed a presurgical question about their future sports participation beliefs. ACLR surgical data were extracted from the Swedish National Knee Ligament Registry, and game participation data were extracted from the Swedish Football Association's administrative data system.
Results:
A total of 959 soccer players (617 [64%] male and 342 [36%] female) were included. The follow-up time after ACLR ranged from 18 months to 5.5 years. Of 720 soccer players (75%) who believed that they would return to play (RTP), 462 (64%) players actually did. Of the players who believed that they would not RTP, 181 (76%) did not. Presurgical beliefs predicted RTP (odds ratio [OR], 5.59; P < .001). Younger age at the time of ACLR favored RTP, where 61% of the players aged 15-20 years had RTP (OR, 3.85; P < .001). At the top competitive level, 84% of the players RTP compared to 14% at the recreational level. Players active at higher levels were more likely to believe that they would RTP, and they also actually did so (OR, 33.06; P < .001). Overall, 67% of players followed their presurgical intention to return to soccer.
Conclusion:
The findings indicated that presurgical beliefs, age, and level of play helped to predict the actual RTP of soccer players after ACLR.
An anterior cruciate ligament (ACL) injury is a severe sports-related knee injury. Soccer is one of the most common sports in which ACL injuries occur. 38 Soccer is a popular sport, with more male than female athletes participating; however, the risk of experiencing an ACL injury is 2 to 3 times higher for female players compared to male players. In addition, female athletes also tend to incur the injury at a younger age. 41
One of the main indications for reconstruction of a torn ACL to restore stability in the knee is the athlete's desire to return to play (RTP) in pivoting sports.6-8,19,20 The RTP rate serves as a crucial outcome measure for ACL reconstruction (ACLR) and rehabilitation.4,6,7,28 Therefore, exploring factors that can affect the RTP rate is vital.6,12,17,29 After ACLR, the majority of athletes report regaining good knee function, but only 50% to 96% actually RTP, with higher numbers for professional athletes. Older age, female sex, cartilage injuries, concomitant or subsequent knee surgery, and pain during physical activity have been presented as negative predictors of RTP.8,35 The reasons reported for non-RTP vary. Sandon et al 32 showed that two-thirds of soccer players who did not RTP reported that it was because of the injured knee, whereas Fältström et al 17 found that only 14% of female soccer players reported poor knee function as the reason for not returning to play. These authors reported that 28% 32 and 25% 17 of the players did not trust their knee because of the fear of a new injury. In most cases, the reason for not returning to play has been discussed as probably being multifactorial2,17,31,34 in which psychological factors such as the fear of new injuries and low confidence are important considerations.
High knee-specific self-efficacy16,21,39 and great motivation17,36 to return to the preinjury level have also been reported as contributing factors for successful RTP. In addition, patients’ expectations have been presented as a prognostic factor for physical recovery30,36; at the same time, unrealistically high expectations can lead to postoperative dissatisfaction for the athlete. 10 As one main reason for undergoing ACLR is to RTP, 84% to 96% of patients expect to RTP.36,42 However, results from a 2022 study of patients in the Swedish National Knee Ligament Registry (SNKLR) showed that only 60% of Swedish soccer players reported believing that they would RTP after their ACL injury. 33
The present study aimed to investigate if self-reported presurgical beliefs toward RTP would correspond to registered official match participation after ACLR, hypothesizing that there would be a significant positive correlation between belief and actual return to participation.
Methods
Study Design
After receiving approval from the Swedish Ethical Review Authority for this study's protocol, we identified all patients with an ACL injury who responded to a soccer-specific questionnaire in the SNKLR between April 2017 and August 2020. The criteria for study inclusion were primary unilateral ACLR registered in the SNKLR within 12 months of answering the questionnaire, age ≥15 years at the time of ACLR, registration on a Swedish soccer league team, and possession of a license in the Swedish Football Association's administrative data system, FOGIS. Included patients were also required to have a minimum follow-up of 18 months since ACLR (ie, no surgery date later than March 2021) to ensure at least an 18-month interval between ACLR and RTP.
A total of 959 soccer players were included (Figure 1). Given the extraction date of registry data in September 2022, the study encompassed follow-up times of up to 5.5 years.

Study flow chart presenting the selection of eligible patients from the SNKLR and FOGIS. SNKLR, Swedish National Knee Ligament Registry; ACL, anterior cruicate ligament; ACLR, ACL reconstruction; RTP, return to play.
Data Collection
Registry data from the SNKLR and FOGIS databases were extracted using players’ social security numbers for comparison. Both female and male soccer players meeting the study criteria were included.
Swedish National Knee Ligament Registry
Established in 2005, the SNKLR serves as a national surgical registry for ACL injuries, with surgical data entered by orthopaedic surgeons. Currently, 90% of all surgical procedures in Sweden are registered. The SNKLR includes self-reported data and patient-reported outcomes on knee function and quality of life before ACLR and at 1, 2, 5, and 10 years after ACLR. According to the annual report from the SNKLR, the registration rate for presurgical patient-reported outcomes overall is approximately 60%. 38
The soccer-specific questionnaire, available in the SNKLR since 2017, captures soccer-related details, including beliefs about RTP. The questionnaire was developed in Germany to identify soccer-specific characteristics of ACL injuries after an increase in ACL injuries among German professional male soccer players. 24 The question “Do you believe that you will continue playing soccer after the ACL injury?” (“yes”/“no” response) measures participants’ RTP beliefs. The participants’ soccer level at the time of the injury, self-registered in the questionnaire, is categorized based on the Swedish soccer league system: “top” (men’s and women's highest and second highest Division), “high” (Division I-II), “middle” (men’s Division III-IV, women's Division III), “low” (women’s Division IV-V, men's Division V-VIII), and “recreational” (recreational sports level).
FOGIS Database
The Swedish Football Association's administrative database, FOGIS, is a comprehensive system that contains registered information on player participation in Swedish soccer league games. All players aged ≥15 years must have a registered license in FOGIS to participate in league games. Extracted information from FOGIS included all official soccer games that the study's players participated in and served as an indicator for return to competition after ACLR.
Statistical Analysis
Statistical analyses were conducted using SPSS Statistics (Version 29; IBM). Descriptive statistics were calculated for all the study variables. Age at the time of ACLR was categorized into 6 groups: 15-20, 21-25, 26-30, 31-35, and ≥36 years. The primary outcome variables (presurgical belief [yes/no] and RTP [yes/no]), both binary in nature, underwent analysis using logistic regression. Adjusted odds ratios (ORs) with 95% confidence intervals were calculated for all covariates in the models. Statistical significance was set at a P value of <.05. Sex-specific relationships were explored through separate analyses for female and male players.
Results
The characteristics of the 959 included soccer players are presented in Table 1. There were 617 (64%) male and 342 (36%) female players, and the follow-up time after ACLR ranged from 18 months to 5.5 years. Overall, 520 (54%) of the players had RTP at a competition level, while 439 (46%) were not. Players who believed before surgery that they would RTP had a significantly higher RTP rate compared to those who did not share this belief (64% vs 24%, respectively; OR, 5.59 [95% CI, 4.01-7.79]; P < .001) (Table 1). Of the 720 (75%) players who believed that they would RTP, 462 (64%) successfully returned. The characteristics of these 720 players based on their ability to actually RTP are shown in Table 2.
Characteristics of Study Population a

Data are presented as n (%) unless otherwise indicated. Boldface P values indicate a statistically significant difference between RTP groups (P < .05) . ACLR, anterior cruciate ligament reconstruction; OR, odds ratio; RTP, return to play.
Reference category for OR comparisons.
Characteristics of Players Who Believed That They Would RTP a

Data are presented as n (%) unless otherwise indicated. Boldface P values indicate a statistically significant difference between RTP groups (P < .05). ACLR, anterior cruciate ligament reconstruction; OR, odds ratio; RTP, return to play.
Reference category for OR comparisons.
The remaining 239 (25%) players did not believe that they would RTP after ACLR. Of these, 181 (76%) did not RTP, while 58 (24%) did RTP (Table 3). In total, the expectations about RTP both before and after surgery (either returning or not returning to soccer) aligned for 643 players (67%), while presurgical expectations were not fulfilled for 316 (33%) players.
Characteristics of Players Who Did Not Believe That They Would RTP a
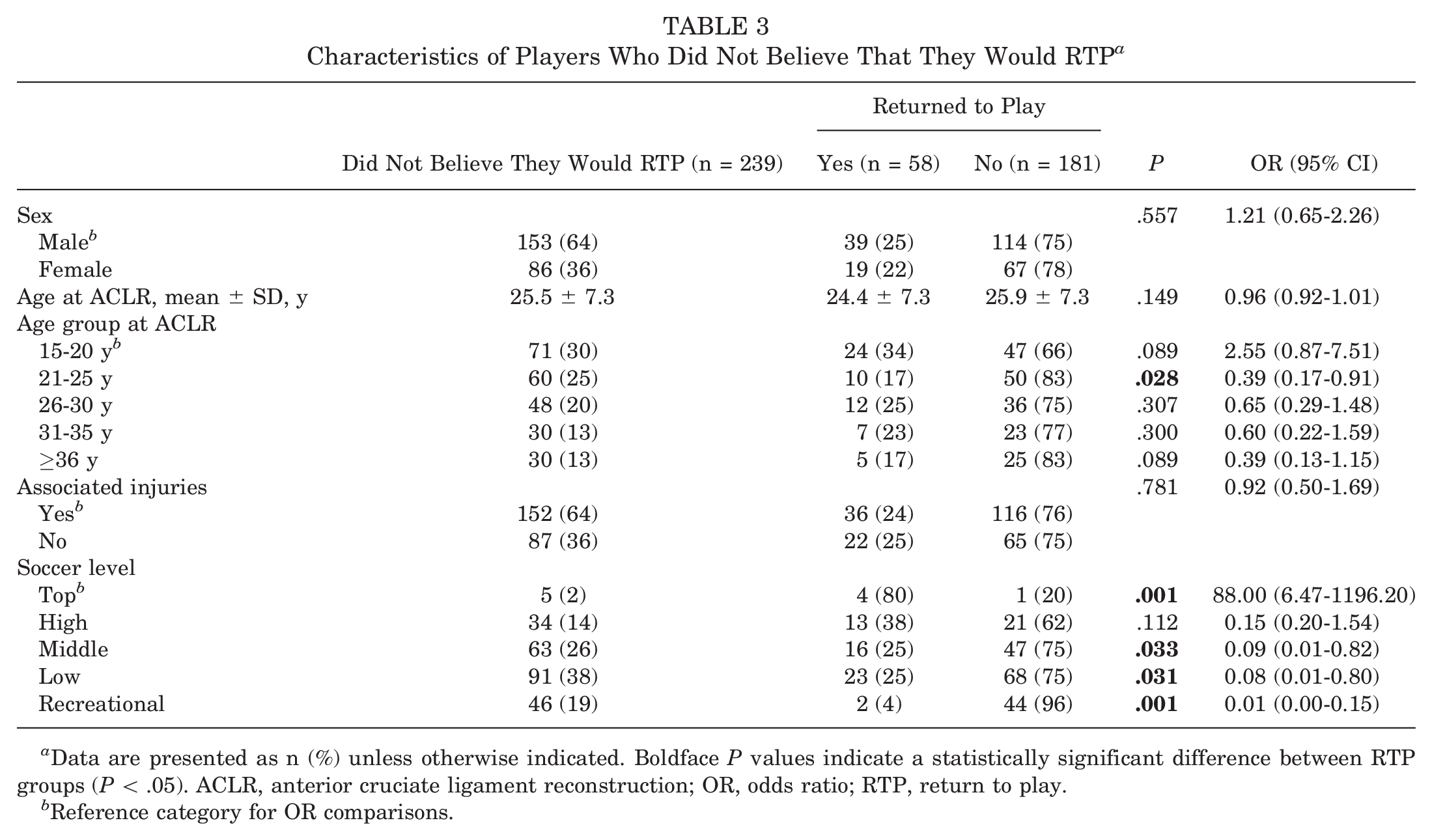
Data are presented as n (%) unless otherwise indicated. Boldface P values indicate a statistically significant difference between RTP groups (P < .05). ACLR, anterior cruciate ligament reconstruction; OR, odds ratio; RTP, return to play.
Reference category for OR comparisons.
Analysis of Covariates
Player Sex
There was no significant difference between female and male players regarding RTP (55% and 54%, respectively) (Table 1) or presurgical beliefs about RTP (75% for both sexes) (Tables 4 and 5).
Characteristics of Female Players a

Data are presented as n (%) unless otherwise indicated. Boldface P values indicate a statistically significant difference between RTP groups (P < .05). ACLR, anterior cruciate ligament reconstruction; OR, odds ratio; RTP, return to play.
Reference category for OR comparisons.
Characteristics of Male Players a
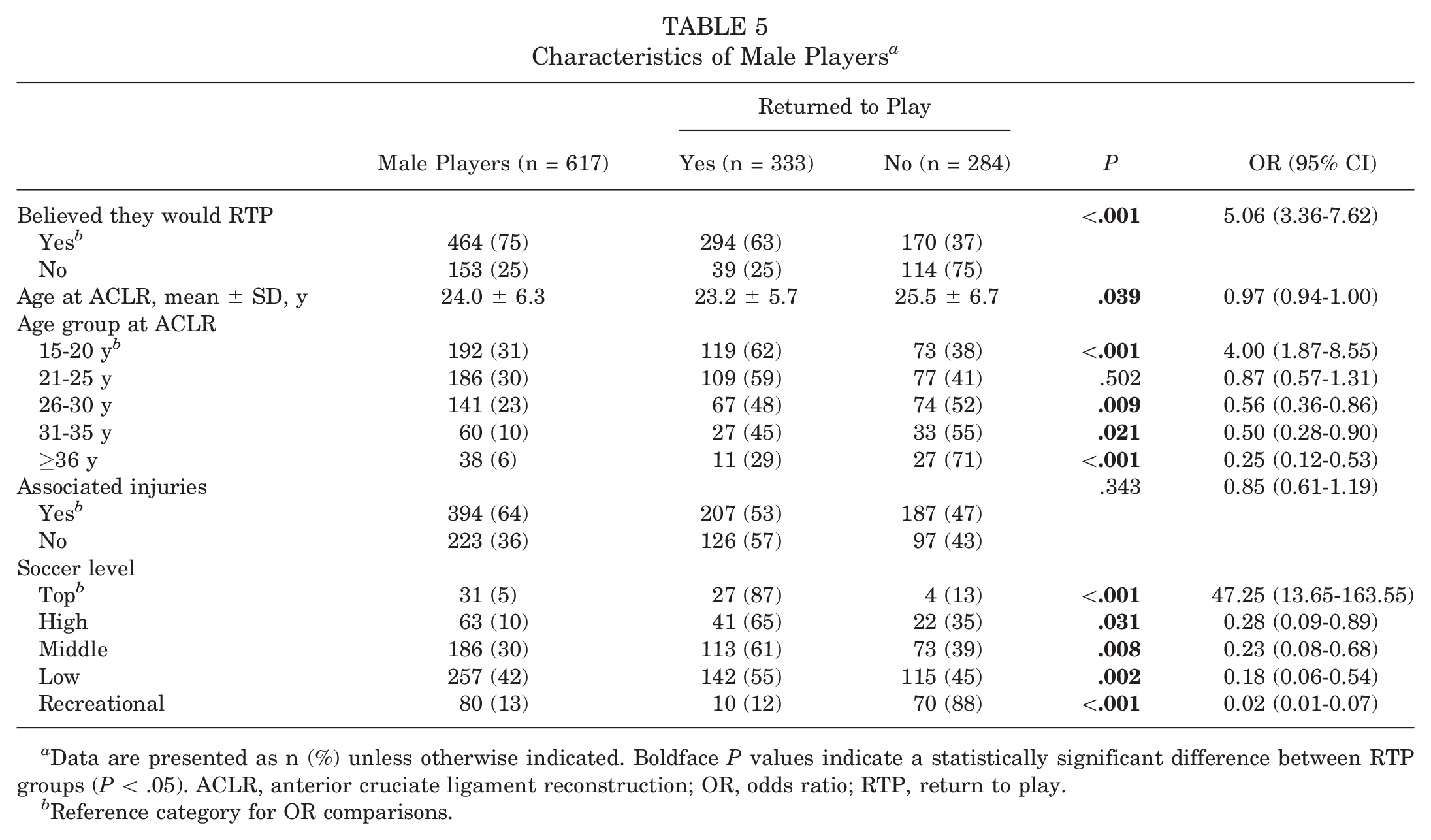
Data are presented as n (%) unless otherwise indicated. Boldface P values indicate a statistically significant difference between RTP groups (P < .05). ACLR, anterior cruciate ligament reconstruction; OR, odds ratio; RTP, return to play.
Reference category for OR comparisons.
Age at ACLR
The mean age of the players at the time of ACLR was 23.0 ± 6.3 years. There was no significant difference in the RTP rate according to age at the time of ACLR among female players (OR, 0.99 [95% CI, 0.95-1.03]; P = .531) (Table 4). However, among male players, younger age at the time of ACLR favored RTP (OR, 0.97 [95% CI, 0.94-1.00]; P = .039) (Table 5).
The highest RTP rate occurred among players aged 15-20 years at the time of ACLR, with 237 (61%) of the players had RTP, and lower RTP rates occurred in older age groups (OR, 3.85 [95% CI, 2.00-7.39]; P < .001) (Table 1). Among male players, those who were younger had a higher RTP rate than players in older age groups (OR, 4.00 [95% CI, 1.87-8.55]; P < .001) (Table 5). No significant difference was observed among female players regarding age.
Soccer players in the youngest age group (15-20 years) were most likely to believe that they would RTP, with 320 (82%) having this belief and 213 (67%) fulfilling this expectation (Table 2). Older age groups were less likely to believe in RTP, although age at the time of ACLR was not found to be significant for presurgical beliefs (Tables 2 and 3).
Associated Injuries
Of 959 players, 572 (60%) players had associated injuries, with 296 (52%) of them RTP (Table 1). No significant differences were observed in the RTP rate or presurgical beliefs for RTP between those with an isolated ACL injury and those with associated injuries or among female or male players (Tables 2-5).
Soccer Level
Players active at a lower level before the ACL injury were less likely to RTP compared to those active at higher levels before the injury (OR, 33.06 [95% CI, 13.33-81.97]; P < .001). At the top level, 49 (84%) of the players returned to play, contrasting with 14 (14%) at the recreational level (Table 1). This trend held true for female and male players separately, with 81% of female players at the top level returning to play compared to 21% at the recreational level (OR, 16.50 [95% CI, 3.80-71.72]; P < .001) (Table 4) and 87% of male players at the top level returning to play compared to 12% at the recreational level (OR, 47.25 [95% CI, 13.65-163.55]; P < .001) (Table 5).
A significant difference in the soccer level variable was observed regarding presurgical beliefs (OR, 19.22 [95% CI, 7.14-51.70]; P < .001) (Table 2). At the top level, 45 (85%) players who believed in RTP actually returned, while the RTP rate decreased at lower soccer levels. At the recreational level, 53 (54%) players thought that they would return, of whom 12 (23%) actually did (Table 2). However, 96% of players in the recreational group who did not believe that they would RTP did not return at a competition level (Table 3).
Discussion
The principal finding in the present study was that a significantly greater proportion of the soccer players who believed that they would RTP before surgery actually did return compared to those who did not share this belief (64% vs 24%, respectively). In other words, despite only half of the players RTP, 67% of players adhered to their presurgical beliefs. These findings underscore the pivotal role of presurgical beliefs and expectations in influencing postsurgical outcomes.
Overall, 25% of players stated preoperatively that they did not believe that they would RTP. Among these players, 24% did in fact return to competition. While the present study lacks information on the reasons for fulfilling RTP despite presurgical disbeliefs, a reasonable hypothesis is that some players achieve higher motivation 17 or improved knee-related self-efficacy 21 during postsurgical rehabilitation. To gain deeper insights into a player's experience and potential contributing factors for fulfilling RTP against initial beliefs, qualitative research would be valuable.
Because of the registry design, we could not provide information about individual reasons for not returning to play among players who initially believed that they would RTP. According to previous studies, the reason for not returning to soccer after ACLR could be knee related. According to Sandon et al, 32 1 of 3 athletes did not RTP because of knee problems; other mentioned reasons were change of career, shifting priorities, and family obligations. Reasons for RTP after ACLR have been presented to be multifactorial in other studies.27,37 Psychological factors have been reported to have an impact on athletes’ ability to return to sports after ACLR,18,22,25 and fear of a new knee injury can be a hindrance for athletes to return to preinjury levels after surgery. 9 High motivation to RTP has been reported as a positive factor for return to sports after an ACL injury.5,17,18
There was no significant difference between male and female players in presurgical beliefs, with 75% of both sexes believing in RTP. This contrasts with previous findings, as Webster and Feller 42 found that male players had greater presurgical expectations to RTP after ACLR compared to female players (90% vs 84%, respectively). The current study also did not reveal a sex-based difference in the actual RTP rate, which differs from other studies. Ardern et al 7 reported male athletes to be more likely to return to preinjury levels after ACLR compared to female athletes, and Sandon et al 35 reported female sex to be a negative predictor for return to soccer after ACLR. In the present study, 36% of the participants were female, which is representative of Swedish ACL injuries. In the annual report from the SNKLR, 34% of the patients experiencing ACL injuries while playing soccer and undergoing primary ACLR were female, and 66% were male. 38 According to Waldén et al, 40 female patients experience an ACL injury at a younger age than male patients. Female patients also undergo ACLR at a younger age than male patients. 38
In the present study, there was no significant sex-based difference in age at the time of ACLR. However, among male players, a younger age at the time of ACLR predicted a higher likelihood of RTP compared to older age at the time of surgery. Soccer players with a younger age at the time of ACLR also exhibited a higher RTP rate than those of older ages. This aligns with previous findings, as Lentz et al 26 reported older age to be a negative influencing factor regarding RTP after ACLR, and Ardern et al 3 showed younger age to be favorable for RTP. In most cases, a younger age does not imply the same responsibilities or demands outside of sports participation as for athletes of an older age. At an older age, priorities such as career or family-related liabilities may be a bigger focus, 3 which may be a reasonable factor for lower RTP rates at higher ages. Previously, Sonesson et al 36 demonstrated higher motivation during rehabilitation to be associated with RTP.
Associated injuries were common at the time of surgery (60%) but did not significantly affect return to soccer in either female or male players. Having an associated injury in the form of a cartilage injury has earlier been presented to be a negative predictor for RTP after ACLR, without a significant difference in rates of return to soccer related to having a meniscal injury. 35 Thus, the presence of associated injuries in the knee may delay or influence the RTP rate. Returning to soccer after ACLR implies a higher risk of new injuries,1,32 and associated injuries (ie, chondral and meniscal injuries) have been presented as predictive factors for the development of osteoarthritis after ACLR. 13
Players at higher levels of competition were more likely to RTP, irrespective of their initial beliefs. Those participating at lower levels were less likely to RTP. This result is in line with results from previous studies.14,15,17,23 Athletes playing at higher soccer levels often benefit from better access to qualified medical teams, better caretaking, and a shorter time to diagnosis compared to those playing at lower levels, positively influencing the RTP rate. 14 Being active at higher levels may also include expectations regarding RTP to a greater extent, both from oneself and the social environment, compared to players active at lower levels. The financial incentive and motivators for RTP may also be higher for elite-level players compared to nonelite players. 11
The findings of this study suggest that, on a group level, a complex interplay of age, level of competition, and individual priorities is a major factor in determining whether the player opts to RTP after ACLR. However, 36% of players did not RTP, despite believing that they would, indicating potential failures related to the knee or a lack of psychological readiness. Understanding the reasons for not returning to play in these athletes requires further investigation beyond the scope of the present study.
In previous studies, one of the main reasons and indicators to recommend an athlete for ACLR, and for the athlete to choose to undergo surgery, has been to enable the player to achieve physical activity demands and return to sports.19,20 However, the present study challenges the assumption that all soccer players aspire to RTP after ACLR. The findings revealed that while 75% of players believed that they would RTP, 25% did not believe that they would return. Of these, 24% did actually RTP, although they preoperatively stated that they believed that they would not. This highlights the need to reconsider RTP as the sole objective outcome of the success and effectiveness of ACLR and rehabilitation protocols. The RTP rate was significantly influenced by athletes’ presurgical beliefs toward RTP and the level of competition at which they were engaged, emphasizing the complex interplay between physical recovery and the athlete's mental outlook. Researchers often use the RTP rate as a critical metric for assessing ACLR effectiveness, but the present study challenges this perspective, suggesting that not returning to game participation should not necessarily be seen as a failure.
Strengths and Limitations
One strength of the present study is the extensive and diverse study population, encompassing both female (n = 342) and male (n = 617) soccer players aged 15 to 47 years, active at various soccer levels. The results of this study can be seen as generalizable to similar pivoting team sports in which an ACL injury is a commonly occurring injury. The study's longitudinal design, combining questionnaire data from the SNKLR and game participation data from FOGIS, contributes to robust findings, as it was possible to control for whether the athlete had returned to playing soccer after ACLR.
Limitations of the present study include the inability to delve into individual reasons for beliefs about RTP because of data constraints and the study design. As the questionnaire is available on the SNKLR website for anyone to voluntarily complete, another limitation is the possible loss of participants in this study because of the low rate of responders. According to the SNKLR's yearly report, 6074 patients who had undergone primary ACLR from 2017 to 2020 sustained their ACL injury while playing soccer, and approximately 50% of these had answered the questionnaire before surgery. While efforts were made to match patients who did not respond to the questionnaire with FOGIS data, the actual player status of nonresponders remained unknown. The follow-up from ACLR ranged from 18 months to 5.5 years. The minimum follow-up was determined to be 18 months to allow for adequate time for RTP, assuming a 12-month rehabilitation period. However, this might result in a loss of participants, as some athletes returned to play after this time frame. Even though some of the registry data were registered during the Coronavirus Disease 2019 pandemic, the study results were not affected by the pandemic.
The study's implications extend to health care professionals, coaches, and sports organizations. Recognizing the pivotal role of presurgical beliefs in RTP decisions can inform tailored rehabilitation strategies and support athletes more effectively. Understanding individual priorities facilitates informed discussions about the potential risks and benefits associated with returning to soccer after ACLR.
Conclusion
The findings of this study indicated that the presurgical beliefs, age, and level of play of soccer players helped to predict their actual return to game participation after ACLR.
Footnotes
Acknowledgements
The authors thank Henrik Hedevik at Linköping University for statistical support.
Final revision submitted August 4, 2024; accepted September 17, 2024.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Swedish Ethical Review Authority (No. 2021-07044-01).