
Abstract
Background:
A discoid meniscus is a morphological variant of normal knee joint meniscus shape and ultrastructure that can lead to traumatic tearing of this tissue and early joint osteoarthritis.
Purpose/Hypothesis:
The purpose of this study was to determine the prevalence of discoid menisci in a large, ethnically diverse regional cohort and to evaluate possible risk factors. The hypothesis was that there would be no difference in the epidemiological distribution of discoid menisci based on ethnicity or sex.
Study Design:
Descriptive epidemiology study.
Methods:
The study population was from a regional, integrated health care system cohort from Kaiser Permanente of Southern California that, as of 2016, included more than 4.5 million patients. Patient demographics included age, sex, and ethnicity within this cohort. Potential risk factors analyzed included age, sex, ethnicity, and body mass index (BMI). Unique characteristics of a discoid meniscus were analyzed, including a symptomatic versus asymptomatic meniscus, location of meniscal tear and type of meniscus, and frequency of meniscal surgical treatment.
Results:
A total of 223 patients with a confirmed discoid meniscus were identified, yielding an overall prevalence rate of 4.88 per 100,000 patients. Those identifying as Black had the lowest prevalence (2.68/100,000), while Hispanic ethnicity had the highest (6.01/100,000). However, there was no significant difference with regard to ethnicity (P = .283), nor any significant difference between sexes. BMI did not significantly influence the rate of discoid menisci (P = .504). A majority (77.5%) of patients were symptomatic, while 22.5% of patients with discoid menisci were asymptomatic and discovered incidentally. Symptomatic discoid menisci were more likely to be operated on compared with asymptomatic discoid menisci (71% vs 14%, respectively; P = .001; odds ratio, 14.8 [95% CI, 5.8-37.2]). Horizontal and bucket-handle tears were the more common tear types. Of the discoid menisci in this cohort, 55.6% underwent surgery, with 95.2% undergoing reported saucerization.
Conclusion:
In this very diverse population-based cohort of patients, there did not seem to be a significant predilection of discoid menisci with regard to ethnicity. Neither sex nor BMI significantly influenced the rate of discoid menisci. More than three-quarters of those with a diagnosed discoid meniscus were symptomatic. Of the tears that occurred with discoid menisci, horizontal and bucket-handle tears made up the largest proportion.
A discoid lateral meniscus is a meniscal abnormality first described by Young in 1889 60 and characterized as an enlarged and/or thickened meniscus with variable peripheral stability. 15,23,32,35,38,40,53 Recently, it has also been described as a histological structural variant with documentation of abnormal collagen fibril organization. 46 Because of its abnormal size, stability, and structure, a discoid meniscus is prone to tearing, pain, and mechanical symptoms. †† The mechanical symptoms include snapping, meniscal subluxation (often referred to by patients as shifting, popping, or dislocating), and loss of extension. ‡‡ A discoid lateral meniscus can be asymptomatic throughout life or can present very early in childhood with the abovementioned symptoms. 14,18,21,23,29,34,44,45 Treatment methods have changed over time from more aggressive open total meniscectomy to arthroscopic techniques aimed at preserving as much functional meniscal tissue as possible in cases of symptomatic and/or torn discoid menisci. §§ Current techniques also allow for peripheral rim stabilization and repair of torn but salvageable tissue. 3,8,17,28,38,40,55
Prior studies investigating the prevalence of discoid lateral menisci have produced variable results. In the United States and Europe, cadaveric studies have shown a 5% to 7% rate in the general population. 18 A similar study from Japan revealed that 33.2% of specimens had some degree of a discoid meniscus (29.6% partial and 3.6% complete), 34 and a study from the Republic of Korea revealed that 8.1% of specimens had a discoid meniscus. 52 Studies have determined that the prevalence in patients undergoing either open or arthroscopic surgery ranged from 0.4% to 5% in mainly White populations in Europe and the United States. 11,18,43,45,53,57 Surgical reports from non-White populations have tended to have higher rates of discoid menisci; examples include Indian (5.8%), 48 Korean (10.5%), 37 and Japanese (16.6%) 31 case series. While these studies likely provide a reasonable estimation of the prevalence of discoid menisci and have been valuable, all of these studies are relatively underpowered in nature.
Finding a true value for the prevalence of discoid menisci can be difficult because of asymptomatic cases being found only incidentally. 18,32,40,44,58,59 With that being said, better powered epidemiology studies can help provide a better estimation of the prevalence of discoid lateral menisci in the general population. This information can be useful to the clinician not only from a counseling perspective but also in providing appropriate clinical suspicion to guide the diagnostic work-up when a patient presents with appropriate symptoms. The purpose of this study was to determine the underlying patient demographics and epidemiology of discoid lateral menisci using a large population-based cohort.
Methods
The methods for this study were modeled on those previously used by Kessler et al 36 in a similar epidemiology study on osteochondritis dissecans of the knee. Institutional review board approval was obtained. Kaiser Permanente of Southern California (KPSC) was selected for this study, as it maintains a large racially, ethnically, and socioeconomically diverse population 39 with more than 4.5 million people. 19 Patients from the years 2011 to 2014 were included from this population. Inpatient, outpatient, and emergency department electronic health records of each patient member were retrospectively reviewed for the International Classification of Diseases, 9th Revision (ICD-9) code corresponding to a discoid meniscus. ICD-9 codes that were used as markers of patients with a discoid meniscus included 717.4 (derangement of lateral meniscus), 717.5 (derangement of meniscus), and 836.1 (tear of lateral cartilage or meniscus of knee). The patients with these ICD-9 codes were further classified by using a sophisticated word crawl to search all patient records for the words “discoid” and “Wrisberg.” All patient records fulfilling these criteria were reviewed to confirm the diagnosis of a discoid meniscus. A chart review of clinical notes, operative reports, and imaging studies was performed. Inclusion criteria consisted of patients with a confirmed diagnosis of a discoid meniscus. Exclusion criteria included those with meniscal tears in the absence of a discoid meniscus diagnosis, issues not consistent with a discoid meniscus, or those lacking confirmatory magnetic resonance imaging or arthroscopic data.
The variables studied included age at presentation, sex, ethnicity, body mass index (BMI), laterality, time from presentation to surgery, presence of tearing, flexion contracture, surgical procedure, repeat surgery, and follow-up. Ethnicity was categorized as non-Hispanic White, Hispanic, non-Hispanic Black, Asian or Pacific Islander, and other. This is based on administrative and self-reported data by patients in this cohort. 22
The frequency of discoid menisci and laterality were calculated by age group, sex, and ethnicity. Univariate logistic regression was used to determine the risk factors for a discoid meniscus that were significant using an alpha value of .05. Multivariate logistic regression was used to estimate odds ratios and 95% CIs while controlling for potential confounders. The outcomes assessed were discoid meniscus and laterality, and the models included race, age, and sex. Possible interactions between age, sex, and ethnicity were examined using likelihood ratio tests. SAS Enterprise Guide version 4.2 (SAS Institute) was used for all analyses.
Results
The KPSC had 4,566,649 patients enrolled as of 2016. 19 Within this population, there were 223 patients with a diagnosis of a discoid meniscus that could be confirmed. This yielded an overall prevalence rate of approximately 4.88 per 100,000 patients. The relative prevalence with regard to ethnicity can be seen in Table 1, which shows the highest prevalence among patients identifying their ethnicity as other (16.42/100,000), compared with the lowest prevalence in those who identified their ethnicity as Black (2.68/100,000). Despite the relative differences in prevalence, there was no significant difference in the rate of discoid menisci based on ethnicity (P = .283). The age range was broad, from 3.1 to 70.8 years, at the time of diagnosis, with a mean age of 25.3 years. Interestingly, based on linear regression, for every 10-year increase in age, the surgical rate decreased by approximately 6% (P = .003; beta = –0.006).
Distribution and Prevalence of Discoid Menisci by Ethnicity a

a Among enrollees with known race/ethnicity (n = 3 not reported).
Of the 223 patients with diagnosed discoid menisci, 77.5% had a clinical history of being symptomatic, while 22.5% were noted to be asymptomatic and were found incidentally. Symptomatic discoid menisci were significantly more likely to be operated on compared with asymptomatic discoid menisci (71% vs 14%, respectively; P = .001), with an odds ratio of 14.8 (95% CI, 5.8-37.2). However, the rate of symptomatic discoid menisci did not significantly vary by age (P = .097). The distribution showed no predilection for sex (Figure 1). Patients who were designated as being underweight had the lowest proportion of discoid menisci. However, those with a BMI categorized as normal, overweight, or obese had roughly similar distributions of discoid menisci (Figure 2). Furthermore, the rate of symptomatic discoid menisci was not significantly different based on BMI (P = .504), nor were rates of surgery significantly different (P = .204).

Distribution of discoid menisci by sex.

Distribution of discoid menisci by body mass index.
The frequency of tears in all patients with a diagnosed discoid meniscus was 55.2%, with patients with symptomatic discoid meniscus showing a 70.5% tear rate. Of those with a meniscal tear, the distribution of the tear location can be seen in Figure 3; the most frequent tear location was in the body of the meniscus. Interestingly, no specific tear location was found to be significantly more symptomatic (P = .072). The most common types of tears seen in discoid menisci were horizontal and bucket-handle tears (Figure 4). Of all the patients with a diagnosed discoid meniscus, 55.6% underwent a surgical intervention regardless of symptoms, and of those who underwent surgery, 95.2% had saucerization as the reported procedure.
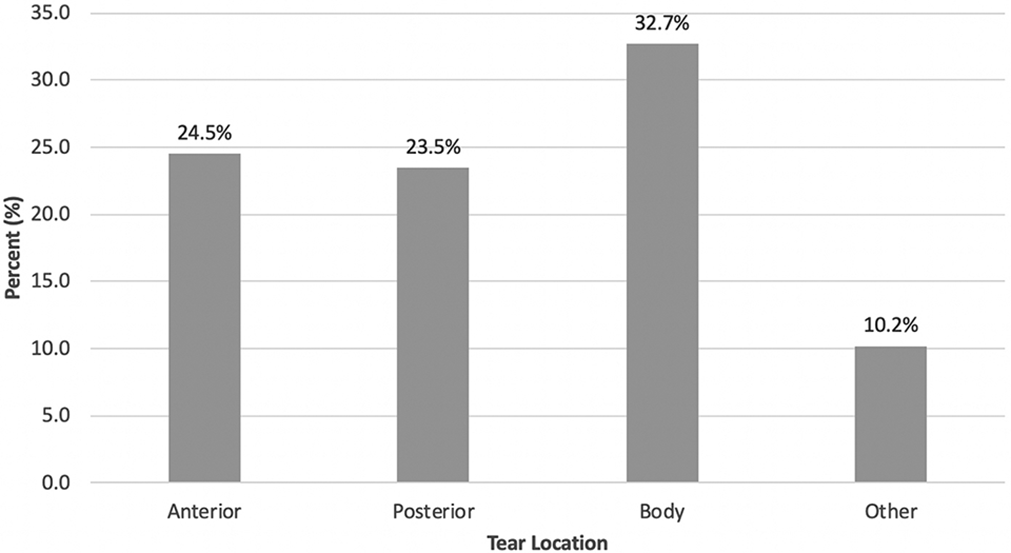
Distribution of discoid menisci by tear location.
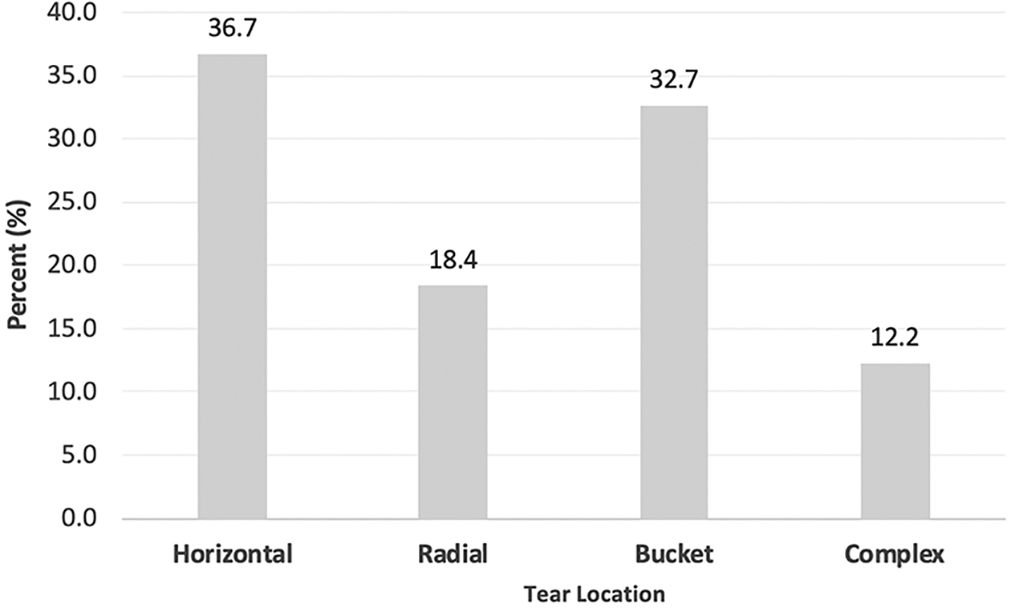
Distribution of discoid menisci by tear type.
Discussion
Compared with previous studies that have looked at the epidemiology of discoid menisci, 32,51,53 to our knowledge, our cohort of patients is the largest and most diverse population analyzed to date. True estimates of epidemiological parameters such as prevalence are difficult to obtain; however, large single-insurer groups such as KPSC allow for a heterogeneous, diverse population to be analyzed. It is known that the presence of a discoid meniscus in a patient portends the potential for pain, tearing, surgical meniscectomy, and subsequent arthritis. 5 As such, physician awareness of and attention to this anatomic variant is essential to provide adequate care to these patients. A discussion of the treatment of discoid menisci must acknowledge that not all discoid menisci are symptomatic. In our large cohort, approximately a quarter of all discoid menisci were judged to be asymptomatic and an incidental finding on magnetic resonance imaging and/or at the time of arthroscopic surgery for other knee abnormalities. Given the asymptomatic nature of a subset of this population, the actual incidence of discoid menisci is unknown. Many previous reports have indicated that the rate of symptomatic lateral discoid menisci in the general population is between 0.4% and 17%. 49,51,58
Our study attempted to look at a diverse population and indicates an estimate on the lower end of this range at 4.88 per 100,000. Additionally, although our data show that Asian ethnicity had a higher prevalence than both White and Black ethnicities, Hispanic ethnicity was found to be the highest.
It is important to recognize that previous published literature shows a wide range of variations on the prevalence of discoid menisci. One reason for these variations may be that the studies that utilize cadaveric specimens to estimate the prevalence are grossly underpowered and methodologically flawed, making their estimates unreliable. 18,34 For example, Casscells’s 18 suggestion of a 5% prevalence is based on 300 cadaveric specimens from a medical school, of which 92% were older than 50 years and of uncertain ethnicity. Similarly, Kato et al’s 34 dissection of 298 cadaveric specimens did not have a single participant younger than 42 years, with 19 of these specimens having menisci that were absent or so torn that they were unable to classify them. In fact, studies with better methodology and greater power show large differences in the estimated incidence. For example, Neuschwander et al 43 reviewed 3468 knee arthroscopic procedures and reported a prevalence of only 0.8% with discoid menisci. Using similar methodology, Albertsson and Gillquist 11 reviewed 7056 knee arthroscopic procedures and found an even smaller prevalence of discoid menisci of 0.4%, albeit in a Swedish population. It appears that better designed, more powered studies show a lower prevalence of discoid menisci.
In our study, we had a very diverse population with millions of patients. This would, in theory, better represent the true statistic of the abnormality. However, the challenge lies in the true prevalence of asymptomatic discoid menisci. Neither previously published studies nor our large, diverse study population can accurately estimate this, and therefore, current statistics on this subset of discoid menisci should be taken with caution.
Sabbag et al 51 did an excellent job of estimating the incidence of symptomatic discoid menisci in a small controlled cohort from a single county. They found the incidence of symptomatic discoid lateral menisci to be 3.2 per 100,000. 51
Ellis et al 24 indicated, in a recent publication, that 97% of patients younger than 13 years with lateral meniscal abnormalities had a discoid lateral meniscus, and 66% of these patients had atraumatic presentation of their pain. For this reason, the early identification of patients with discoid menisci may be beneficial to allow for an early diagnosis and subsequent intervention. However, nearly a quarter of our patients with a discoid meniscus remained asymptomatic, leading one to question whether an early intervention before the development of symptoms should be undertaken.
Limitations of our study include the wide scope of our patient collection. By nature of querying a large database, we lack information that is not included within the data registry, such as specific arthroscopic details of the meniscus. In addition, given that this review was retrospective in nature, there is likely a significant amount of underreporting of the abnormality in our population. Patients with a torn discoid meniscus may have simply been reported as having a “meniscal tear” rather than a “torn discoid meniscus,” given that physicians were not specifically queried as to the meniscal morphology. Furthermore, patients who were not specifically screened for a discoid meniscus were likely not included in our study group, contributing to a low sensitivity of this method for detecting a discoid meniscus. Another potential limitation to consider is the generalizability of our data. The study statistics reflect a specific population from the southwest United States with a differing demographic distribution than other areas of the country. A large multicenter study to assess the prevalence and outcomes of discoid menisci across the United States would be the ideal design to assess epidemiological variance.
Strengths of our study include the large, all-encompassing nature of our population. Our study population was quite diverse in terms of race and socioeconomic status. Future work should focus on a prospective strategy to identify patients, specifically in the pediatric population, and follow them longitudinally. Moreover, it will be important for future work to establish an outcome registry for patients who undergo various interventions (repair, partial or total meniscectomy, and saucerization) to better understand the long-term implications of our treatment modalities.
Conclusion
Our analysis of a large, diverse regional cohort showed that there was no significant difference in the prevalence of discoid menisci based on ethnicity. Similarly, there was no difference in the prevalence based on sex or BMI. Approximately a quarter of discoid menisci were found incidentally, and of the approximately three-quarters that were symptomatic, 70.5% were associated with a meniscal tear, with horizontal and bucket-handle tears being the most common. Of those treated with surgery, most underwent simple saucerization.
Footnotes
Final revision submitted March 27, 2020; accepted April 10, 2020.
Notes
Ethical approval was not sought for the present study.