
Abstract
Background:
As a subset of symptomatic discoid lateral meniscal (DLM) tears, anterior horn (AH) meniscal tears are not well studied in the pediatric population. There are even fewer studies reporting patient-reported outcomes after surgical treatment of AH tears in DLM.
Purpose:
To compare reported outcomes after surgical treatment of DLM tears involving the AH versus other locations in pediatric patients.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A retrospective review of prospectively collected patient data between 2013 and 2020 was conducted. Patients aged <18 years who underwent arthroscopic treatment of a symptomatic DLM were included. Pathology was classified as tears of the AH or tears not involving the anterior horn (NAH). Demographic data along with patient-reported outcome scores (Pediatric International Knee Documentation Committee [Pedi-IKDC] and Patient Assessment Questionnaire [PAQ]) were collected preoperatively through 24 months of follow-up.
Results:
A total of 41 patients were included (median age, 12.9 years; range, 7-17 years; 32% female, 68% male). The mean follow-up time for was 25 months (range, 8-58 months). There were 17 (41%) patients in the AH group and 24 (59%) patients in the NAH group. Of the AH group, 16 (94%) were treated with meniscal repair (vs menisectomy), while 19 (79%) of the NAH group were treated with meniscal repair. All patients achieved significant pre- to postoperative improvement on both the Pedi-IKDC and the PAQ. At 24-month follow-up, there were no differences between the AH and NAH groups on the Pedi-IKDC (92.51 vs 89.72; P = .18) or the PAQ (2.57 vs 2.61; P = .06).
Conclusion:
Patients who underwent meniscal repair for AH DLM reported positive postoperative outcomes.
Pediatric patients with symptomatic lateral meniscal pathology have a high incidence of discoid menisci: up to 75% in patients aged <16 years and 97% in patients aged <13 years. 5 The histologic features of discoid lateral meniscus (DLM) consist of an irregular ultrastructure with disorganized fibril structures, reduced vascularity, and low collagen density. 15 This leads to abnormal force distribution through the meniscus and increased susceptibility to injury. 12
There are no studies analyzing anterior horn (AH) DLM tears nor are there reports concerning outcomes of surgical treatment of AH DLM tears in the pediatric population. We believe there are 3 potential reasons for this. First, the classic Watanabe classification defined unstable DLM as lacking posterior peripheral attachments. Lack of posterior peripheral attachments was also an important part of DLM imaging classification. 2 This established the importance of the posterior horn of the DLM. Focus was then directed to elucidating and studying the role of posterior instability and meniscal tears in symptomatic DLM.1,18 The Pediatric Research in Sports Medicine DLM classification system was created to address the shortcomings of previous DLM classifications and includes anterior tears as components of its classification system.7,11 However, this classification system is not widely used. Second, static magnetic resonance imaging (MRI) does not reliably identify AH peripheral tears. 4 Third, the AH of the lateral meniscus is easily overlooked during arthroscopy because of its proximity to the arthroscope when placed in the lateral portal as well as limitations of the 30° arthroscope.18,19
The aims of this study were to (1) compare patient-reported outcomes (PROs) after arthroscopic treatment of DLM tears involving the AH versus other locations and (2) report the incidence of AH pathology in DLM injuries. We hypothesized that surgically treated AH tears would have similar outcomes to tears in other locations.
Methods
Patient Data Collection
The study protocol received institutional review board approval, and an analysis of patients aged <19 years who underwent primary, isolated arthroscopic repair or saucerization of a symptomatic DLM between 2013 and 2020 at a large, urban academic pediatric orthopaedic center was performed. All surgeries were performed by 2 pediatric sports medicine fellowship–trained orthopaedic surgeons. A total of 159 patients were recruited to the study. Patients with concurrent ligamentous or cartilaginous injuries, congenital or acquired lower extremity deformities, previous ipsilateral knee surgeries, significant medical comorbidities, and those aged >19 years were excluded from collection, leaving 79 patients with imaging findings showing discoid menisci. These 79 underwent operative treatment for their discoid meniscus, and 23 were excluded for intraoperative diagnosis of incomplete discoid meniscus. Of the remaining 56 patients, 15 were excluded for incomplete follow-up, leaving 41 patients in the final study group. Seventeen (41%) of these patients had AH tears (AH group), while 24 (59%) patients had tears of the body, posterior root, or posterior horn that did not involve the anterior horn (NAH group). Figure 1 outlines the patient-selection process.

Flowchart showing cohort selection process. MRI, magnetic resonance imaging.
Surgical Technique
The patient was prepared and draped with standard sterile pretechniques, and a sequential compression device was placed on the nonoperative leg for deep venous thrombosis prophylaxis. A thigh tourniquet was placed on the operative upper thigh. At this point, standard anterolateral and superomedial arthroscopy portals were then made.
Diagnostic arthroscopy was performed in the following order:
Suprapatellar pouch: checked for loose bodies
Patellofemoral joint: checked for central tracking of patella and signs of chondromalacia or malalignment
Medial and lateral gutters: checked for loose bodies
Medial compartment: checked for stability of meniscus, as well as no articular damage
Notch: checked for intact ACL and PCL
Lateral compartment: checked for tears/degenerative changes within known discoid meniscus (Figure 2)
The lateral meniscus was addressed by saucerization with a combination of arthroscopic shavers and meniscal baskets until there was an approximate 8-mm peripheral rim throughout. The anterior portion of the lateral meniscal tear has usually 2 separate outside-in No. 0 PDS sutures placed (Ethicon). Two 18-gauge spinal needles, spaced approximately 4 mm apart and threaded with PDS suture, were introduced percutaneously through the anterior lateral joint line, through the capsule and meniscus, then out through the central portion of the meniscus. The 2 joint suture ends were grasped into the anterolateral portal. With one of the sutures as a shuttling suture, the other PDS suture was shuttled such that a horizontal mattress suture was in the meniscus. A vertical 5-mm incision was made between the percutaneous entrance sites of the spinal needles. A hemostat was used to spread the subcutaneous tissue in this incision to the anterior capsule. A probe was used to pull the 2 sutures on either side of the incision into the incision. The suture was tied over the capsule (Figure 3).

An anterior horn discoid lateral meniscal tear in a right knee as it appears from the medial arthroscopic portal.

The end result of a standard outside-in technique. The blue structure is the suture from the repair.
After repair, a probe demonstrated that the meniscus was stable. The arthroscopic equipment was removed from the knee. The portal incisions were closed with No. 3-0 Monocryl simple interrupted sutures (Ethicon). Sterile dressings were applied. A cold therapy unit was placed over the knee, followed with a hinged knee brace locked in extension.
Postoperative Protocol
The postoperative protocol was limited weightbearing for 6 weeks with transition to full-weight bearing after that. Range of motion was allowed from 0° to 50° for the first 3 weeks, then 0° to 90° for the following 6 weeks in conjunction with a focused physical therapy program. Patients undergoing DLM saucerization were allowed to weightbear as tolerated and perform range of motion as tolerated in conjunction with a focused physical therapy program.
Outcome Evaluation
Demographic data including age, sex, insurance type, race, and body mass index were collected preoperatively. The time elapsed from injury to operative treatment was recorded. Two validated pediatric PRO scores, the Pediatric International Knee Documentation Committee (Pedi-IKDC) and the Patient Assessment Questionnaire (PAQ), were collected preoperatively and at 6-, 12-, and 24-month follow-up intervals.13,17 Each DLM was classified arthroscopically by tear location (AH, body, posterior horn, anterior root, posterior root, or multiple tears) and tear pattern (horizontal, longitudinal, radial, or complex [which includes any tear with >1 tear pattern].
Univariate analysis was used to compare demographic data, tear pattern, treatment type (repair vs meniscectomy), and wait time from symptom onset to surgery between the AH and NAH groups. Comparative analyses of the continuous variables were completed with the chi-square and t tests, with the utilization of a 2-tailed method for categorical variables. Comparison of PRO scores between the AH and the NAH groups was performed using a linear mixed-effects regression model. Because PRO scores are nondependent in nature and variability existed both within and between groups, a linear mixed-effects regression was utilized to allow for both fixed and random effects when comparing patient groups. Due to limited available data, marginal estimates were created from the available data to provide weighted means at each follow-up interval. 16 In other words, this created predicted means at each time point from the data recorded. Patients who had data available at all follow-up intervals were weighed more heavily in our model. Additionally, differences in the change in scores over time between AH and NAH patients were assessed using a time-by-tear interaction term. This allowed for a more thorough evaluation of the effect of tear location at each follow-up interval and to elucidate whether the location of tear had a variable statistical interaction with the respective PRO score over time. Analysis was carried out in R Version 3.3.1 (R Core Team; R Foundation for Statistical Computing). Significance was determined as P < .05.
Results
The median age of the cohort was 12.9 years (7-17 years old). 32% were female, while 68% were male. The mean follow-up time for the overall cohort was 25 months (range, 8-58 months). The majority (83%) of the study patients were publicly insured. Patients were primarily Hispanic (35 patients; 85%), with 2 non-Hispanic White patients (5%). The mean time from symptom onset to surgery was 289 days (29-1308 days). There were 20 left-sided pathologies and 21 right-sided pathologies. Demographic data of the study groups is outlined in Table 1.
Demographic Characteristics of Study Groups a
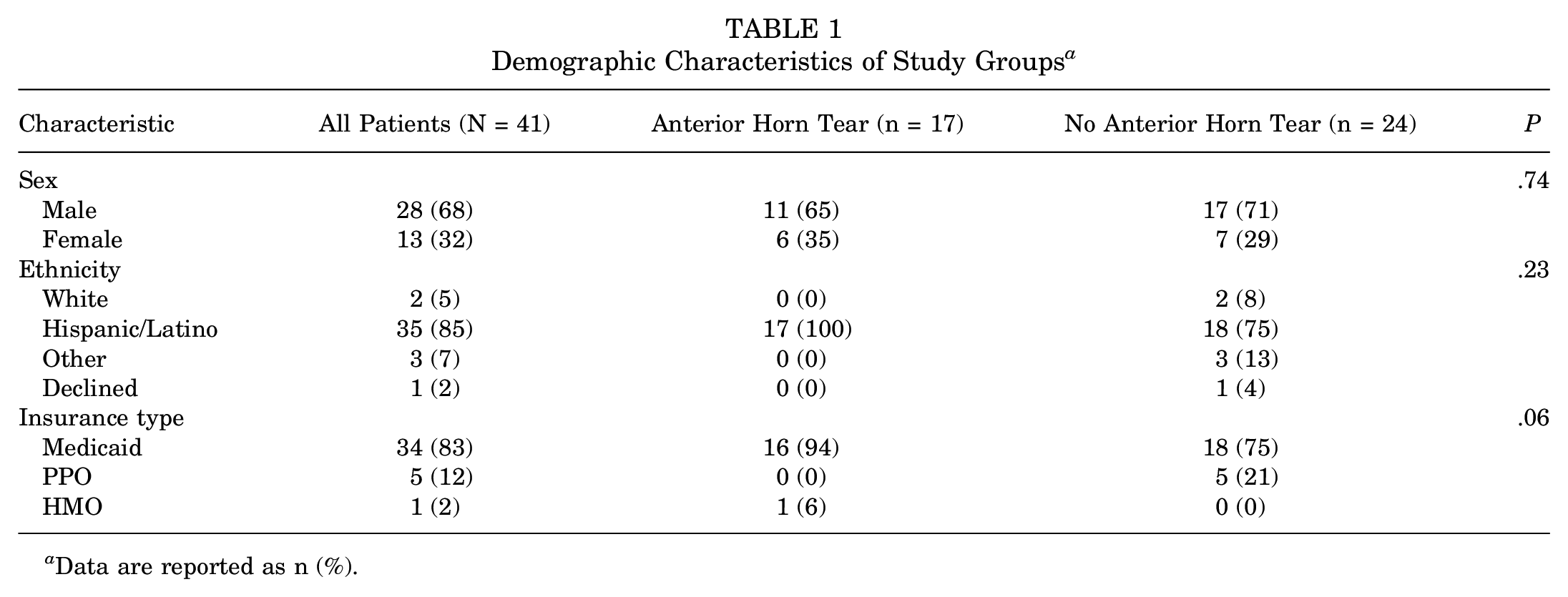
Data are reported as n (%).
Of the 41 study patients, 35 were treated with meniscal repair and 6 were treated with saucerization, which was not statistically significant between groups (P = .37) (Table 2). There was no difference in tear patterns between groups (P = .48), with complex tears being most common among both groups (Table 2).
Treatment Types and Meniscal Tear Types by Study Group a
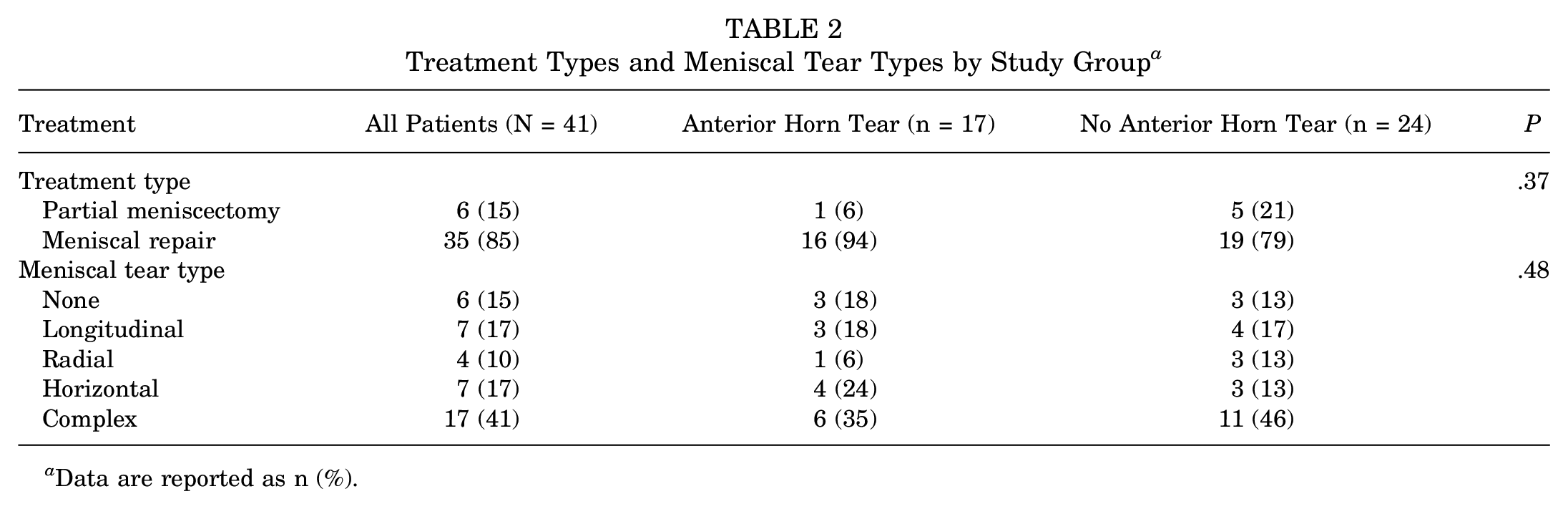
Data are reported as n (%).
The results of the linear regression analysis are shown in Figure 4. There was no difference between the NAH and AH groups in preoperative Pedi-IKDC or PAQ scores, and patients in both groups saw significant pre- to postoperative improvement on both scores. There were no differences between the AH and NAH groups in Pedi-IKDC scores at the 1-year (89.19 vs 90.80; P = .12) or 2-year (92.51 vs 89.72; P = .18) follow-up; furthermore, the effect of tear location on Pedi-IKDC scores did not change over time (P = .19). Similarly, there were no differences between the AH and NAH groups in PAQ scores at the 1-year (2.14 vs 2.63; P = .06) or 2-year (2.57 vs 2.61; P = .06) follow-up, nor did the effect of tear location on PAQ scores change over time (P = .23).

The mixed-model linear regression model predicted values of the (A) Pediatric International Knee Documentation Committee (Pedi-IKDC) scores and (B) Patient Assessment Questionnaire (PAQ) scores in the groups with and without anterior horn tear over 2 years.
No reoperations or complications were noted within the follow-up period. Four (10%) patients (3 NAH and 1 AH) had surgery on their contralateral knee for DLM pathology during the follow-up period. Three patients (1 in NAH and 2 in AH) reported pain at one point during follow-up but had negative MRIs for retears and were successfully treated with physical therapy. Of the 17 patients with AH tears, 15 had PRO scores available for analysis at 1 year follow-up and 7 were available at 2-year follow-up. Of the NAH group, 19 had PRO scores available for analysis at 1-year follow-up and 12 had scores available at 2 years.
Discussion
In our retrospective cohort, 41% of patients who were surgically treated for DLM had AH tears. To our knowledge, this is the first prospective study looking at PROs after AH DLM tears.
Short-term PROs after surgical treatment of DLM showed significant improvement, whether patients were treated with repair, saucerization, or a combination of treatments.5,7,9 Similarly, the AH group had equivalent outcomes to the NAH group in this study. Klingele et al 8 and Good et al 6 reported an incidence of 47% and 53% rates of anterior meniscal pathology, respectively in their studies, similar to our 41% with AH tears. Outside of these reports, there are few studies describing AH tears. Previously, studies have solely focused on posterior horn tears or failed to mention tear location.3,10
Along with tear location, there was no significant difference in tear pattern between the AH and the NAH groups. The most common tear pattern in both groups was complex, with 17 (41%) patients being evaluated for a complex, mulitplanar tear. Horizontal cleavage tears were the second most common tear pattern in the AH cohort, making up 24% of the tears, and 13% of the NAH cohort were evaluated with horizontal cleavage tears. Due to intrasubstance microstructural disorganization, DLM is more prone to horizontal meniscal tears. This is why horizontal tears are classified independently from all other tear patterns.3,11,14
Limitations
There are several limitations to this study. Although the data were prospectively collected, all the limitations inherent to retrospectively reviewing prospective data apply. Additionally, this study population is small given the rarity of this condition, and <50% patients had available PRO data at 2 years for comparison despite having clinical follow-up. Also, a number of patients did not have 2-year follow-up PRO data available: Data were available for 7 of the 17 patients in the AH group and 12 of the 24 in the NAH group. Our study population is rather homogeneous, which also limits the applicability of our results to all patient populations.
Conclusion
Surgical management of symptomatic DLM tears in the pediatric population may involve the AH. At 2-year follow-up, there was no difference in PRO scores between tear locations. Surgeons should thoroughly evaluate imaging and arthroscopic findings for AH tear location when treating pediatric DLM patients.
Footnotes
Final revision submitted August 6, 2023; accepted August 21, 2023.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from University of California, Los Angeles (ref No. 17-000389).